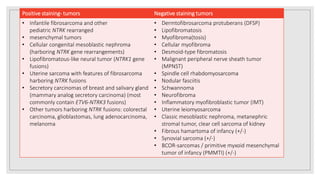
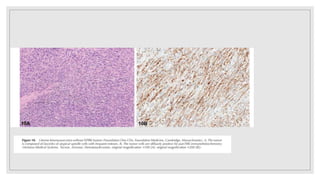
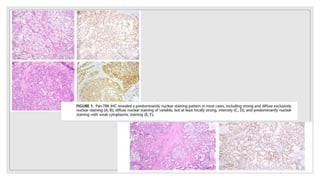
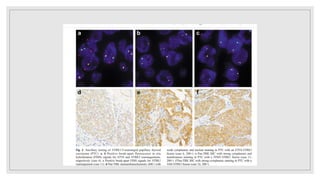
Pan-trk is an immunohistochemical marker used to detect overexpression of NTRK protein fusions linked to various tumors, particularly secretory carcinomas and pediatric tumors. NTRK fusions are considered oncogenic drivers and have been identified in over 20 tumor types, with varying frequency across different cancer morphologies. The sensitivity and specificity of pan-trk IHC make it a valuable tool for diagnosis, although confirmatory testing with methods like ETv6 FISH may be necessary in ambiguous cases.








































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















