Downloaded 16 times
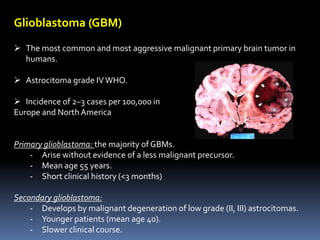
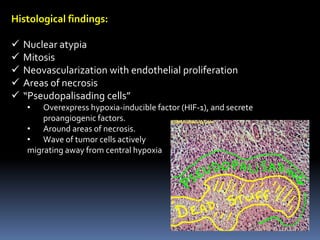
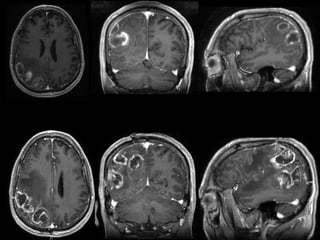
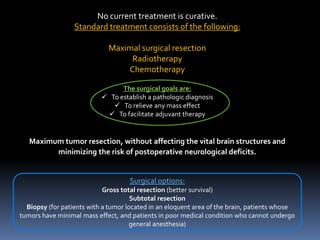
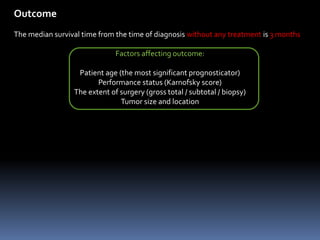
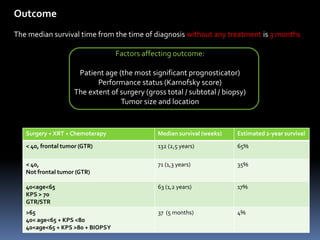
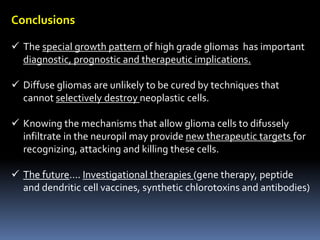


Diffuse gliomas, particularly glioblastomas, exhibit unique infiltrative growth patterns that contribute significantly to their aggressive nature and therapeutic challenges. The document discusses the histological characteristics, growth mechanics, and limitations of current treatment strategies for gliomas, emphasizing the need for innovative approaches targeting the tumor's invasive capabilities. The prognosis remains poor, with median survival around three months without treatment, underscoring the importance of understanding glioma biology for future therapies.


































































































