Aortic Regurgitation Causes, Symptoms, Diagnosis
•Download as DOCX, PDF•
4 likes•1,172 views

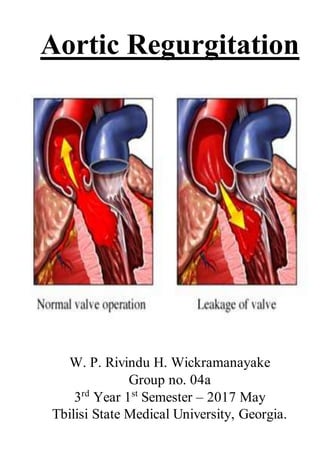
Aortic regurgitation occurs when the aortic valve does not close properly, allowing blood to flow back into the left ventricle. It can be caused by conditions that damage the aortic valve such as rheumatic fever or a congenital heart defect. Symptoms may include breathlessness, fatigue, and chest pain. Diagnosis is made through echocardiogram which can assess the severity. Treatment depends on severity but may involve lifestyle changes, medications, or aortic valve replacement surgery if symptoms worsen or damage to the heart progresses. Prognosis depends on severity and treatment, with severe untreated cases having a high risk of heart failure or sudden cardiac death.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Aortic Regurgitation Causes, Symptoms, Diagnosis
Similar to Aortic Regurgitation Causes, Symptoms, Diagnosis (20)
More from Rivindu Wickramanayake
More from Rivindu Wickramanayake (20)
Recently uploaded
Recently uploaded (20)
Aortic Regurgitation Causes, Symptoms, Diagnosis
- 1. Aortic Regurgitation W. P. Rivindu H. Wickramanayake Group no. 04a 3rd Year 1st Semester – 2017 May Tbilisi State Medical University, Georgia.
- 2. Etiology and Pathophysiology This condition is due to disease of the aortic valve cusps or dilatation of the aortic root. The LV dilates and hypertrophies to compensate for the regurgitation. The stroke volume of the LV may eventually be doubled or trebled, and the major arteries are then conspicuously pulsatile. As the disease progresses, left ventricular diastolic pressure rises and breathlessness develops.
- 3. Clinical Features Until the onset of breathlessness, the only symptom may be an awareness of the heart beat, particularly when lying on the left side, which results from the increased stroke volume. Paroxysmal nocturnal dyspnoea is sometimes the first symptom, and peripheral oedema or angina may occur. The characteristic murmur is best heard to the left of the sternum during held expiration, a thrill is rare. A systolic murmur due to the increased stroke volume is common and does not necessarily indicate stenosis. The regurgitant jet causes fluttering of the mitral valve and, if severe, causes partial closure of the anterior mitral leaflet leading to functional mitral stenosis and a soft mid-diastolic (Austin Flint) murmur. In acute severe regurgitation (e.g. perforation of aortic cusp in endocarditis) there may be no time for compensatory left ventricular hypertrophy and dilatation to develop and the features of heart failure may predominate. In this situation, the classical signs of aortic regurgitation may be masked by tachycardia and an abrupt rise in left ventricular end-diastolic pressure; thus, the pulse pressure may be near normal and the diastolic murmur may be short or even absent.
- 4. Symptoms Mild to Moderate AR Often asymptomatic Awareness of heart beat, ‘palpitations’ Severe AR Breathlessness Angina Signs 1)Pulses Large-volume or ‘collapsing’ pulse Low diastolic and increased pulse pressure Bounding peripheral pulses Capillary pulsation in nail beds: Quincke’s sign Femoral bruit (‘pistol shot’): Duroziez’s sign Head nodding with pulse: de Musset’s sign 2) Murmurs Early diastolic murmur Systolic murmur (increased stroke volume) Austin Flint murmur (soft mid-diastolic) 3) Other Signs Displaced, heaving apex beat (volume overload) Presystolic impulse Fourth heart sound Crepitations (pulmonary venous congestion)
- 5. Causes of Aortic Regurgitation Any condition that damages a valve can cause regurgitation. Causes of aortic valve regurgitation include: Congenital heart valve disease. Been born with an aortic valve that has only two cusps (bicuspid valve) or fused cusps rather than the normal three separate cusps. At risk of developing aortic valve regurgitation at some time in the life. Endocarditis. The aortic valve may be damaged by endocarditis — an infection inside heart that involves heart valves. Rheumatic disease. Rheumatic fever — a complication of strep throat and once a common childhood illness — can damage the aortic valve. Many older adults were exposed to rheumatic fever as children, although they may not have developed rheumatic heart disease. Disease of Aortic Dilatation. Other rare conditions can enlarge the aortic valve and lead to regurgitation, including Marfan syndrome, a connective tissue disease, Aneurysm, Dissection, Syphilis, Ankylosing spondylitis. Trauma. Damage to the aorta near the site of the aortic valve, such as damage from injury to your chest or from a tear in the aorta, also can cause backward flow of blood through the valve. High blood pressure (hypertension). High blood pressure may stretch the root of the aorta where the aortic valve sits. The valve flaps (cusps) may no longer meet, resulting in leakage. Age. By middle age, you can develop some aortic valve regurgitation caused by natural deterioration of the valve.
- 6. Investigations Regurgitation is detected by Doppler echocardiography. In severe acute aortic regurgitation, the rapid rise in left ventricular diastolic pressure may cause premature mitral valve closure. Cardiac catheterisation and aortography can help in assessing the severity of regurgitation, and dilatation of the aorta and the presence of coexisting coronary artery disease. MRI is useful in assessing the degree and extent of aortic dilatation. Diagnostic Tests Echocardiogram. Dilated LV Hyperdynamic LV Fluttering anterior mitral leaflet Doppler detects reflux Exercise tests. Different types of exercise tests help measure your tolerance for activity and check your heart's response to exertion. Cardiac magnetic resonance imaging. Using a magnetic field and radio waves, this test produces detailed pictures of your heart, including the aortic root. Electrocardiogram (ECG). Initially normal, later left ventricular hypertrophy and T-wave inversion Chest X-ray. Cardiac dilatation, maybe aortic dilatation Features of left heart failure Cardiac catheterization. Dilated LV Aortic regurgitation Dilated aortic root
- 7. Echocardiogram Less Invasive Techniques Aortic valve replacement generally requires open-heart surgery under general anesthesia and with the use of a heart-lung bypass machine. Less invasive surgical techniques, such as using a small, lighted tube through a small incision to see the surgical area (laparoscopy), are being explored for aortic valve surgery. Minimally invasive cardiac surgery is associated with less pain, a shorter hospital stay and fewer complications. However, the surgery is more complex than open-heart surgery, partly because the surgeon can't see the valve as well.
- 8. Management Treatment may be required for underlying conditions such as endocarditis or syphilis. Aortic valve replacement is indicated if aortic regurgitation causes symptoms, and this may need to be combined with aortic root replacement and coronary bypass surgery. Those with chronic aortic regurgitation can remain asymptomatic for many years because compensatory ventricular dilatation and hypertrophy occur, but should be advised to report the development of any symptoms of breathlessness or angina. Asymptomatic patients should also be followed up annually with echocardiography for evidence of increasing ventricular size. If this occurs or if the end-systolic dimension increases to ≥ 55 mm, then aortic valve replacement should be undertaken. Systolic BP should be controlled with vasodilating drugs such as nifedipine or ACE inhibitors. There is conflicting evidence regarding the need for aortic valve replacement in asymptomatic patients with severe aortic regurgitation. When aortic root dilatation is the cause of aortic regurgitation (e.g. Marfan’s syndrome), aortic root replacement is usually necessary. Prognosis The prognosis for patients with severe AR depends on the presence or absence of LV dysfunction and symptoms In asymptomatic patients with normal EF, the following has been found: Rate of progression to symptoms or LV dysfunction - Less than 6% per year Rate of progression to asymptomatic LV dysfunction - Less than 3.5% per year Rate of sudden death - Less than 0.2% per year In asymptomatic patients with decreased EF, the rate of progression to symptoms is greater than 25% per year, while in symptomatic patients, the mortality rate is over 10% per year. The strongest predictors of outcome are echocardiographic parameters (EF and LV end- systolic dimension), underscoring the crucial role of serial echocardiography in the management of patients with severe AR. Exercise LV end-systolic volume index (LVESVi) may have prognostic value as an independent predictor of outcomes in in patients with asymptomatic moderate or severe AR. Severe acute AR, if left untreated, is likely to lead to considerable morbidity and mortality from either the underlying cause (typically infective endocarditis or aortic dissection) or from hemodynamic decompensation of the LV. Potential complications in patients with severe chronic AR include progressive LV dysfunction and dilation, congestive heart failure, myocardial ischemia, arrhythmia, and sudden death. Additional complications may arise as a result of the patient's underlying condition (such as aortic root dissection in a patient with a bicuspid aortic valve and a severely dilated aortic root).
- 9. Morbidity and Mortality Severe acute AR carries a very high short-term rate of morbidity and mortality owing to the imposition of a greatly increased regurgitant volume upon a relatively noncompliant LV. Increased LV end-diastolic pressure leads to elevated left atrial and pulmonary pressures with resulting pulmonary edema, as well as decreased coronary perfusion gradients that potentially can cause myocardial ischemia and even sudden cardiac death. In most cases, early (if not emergent) surgical intervention is warranted. Severe chronic AR tends to follow a more gradual clinical course. This is typically characterized initially by a long, relatively asymptomatic period. However, once symptoms ensue, the patient's clinical status may deteriorate relatively rapidly. Thus, current guidelines recommend surgical intervention before symptoms develop, usually based on echocardiographic parameters. References ; 1. Heart valve disease. National Heart, Lung, and Blood Institute. http://www.nhlbi.nih.gov/health/dci/Diseases/hvd/hvd_all.html. Accessed June 2, 2014. 2. Roles of your four heart valves. American Heart Association. http://www.heart.org/HEARTORG/Conditions/More/HeartValveProblemsandDisease/Roles- of-Your-Four-Heart-Valves_UCM_450344_Article.jsp. Accessed June 2, 2014. 3. Gaasch WH. Pathophysiology and clinical features of chronic aortic regurgitation in adults. http://www.uptodate.com/home. Accessed June 16, 2014. 4. Aldea GS. Minimally invasive aortic and mitral valve surgery. http://www.uptodate.com/home. Accessed June 6, 2014. 5. Foster E. Echocardiographic evaluation of the aortic valve. http://www.uptodate.com/home. Accessed June 17, 2014. 6. Maganti K, et al. Vascular heart disease: Diagnosis and management. Mayo Clinic Proceedings. 2010;85:483. 7. http://emedicine.medscape.com/article/150490- overview?pa=Cz4LfRR0tInYaGS%2Fq6RVEV64%2BOu0xMreMErhw2qZJO7FP%2FGC WB8ObFLwEoAzPsLwN%2F22ndcxWXDSwAlwdxI7jWzYrTvKGH%2BN6IWvoAuvVog %3D#showall 8. http://www.mayoclinic.org/diseases-conditions/aortic-valve- regurgitation/basics/definition/con-20022523 9. https://patient.info/health/aortic-regurgitation-leaflet 10. http://www.heart.org/HEARTORG/Conditions/More/HeartValveProblemsandDisease/Proble m-Aortic-Valve-Regurgitation_UCM_450611_Article.jsp#.WS6_-mh97IU 11. www.webmed.com