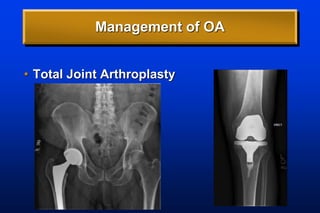
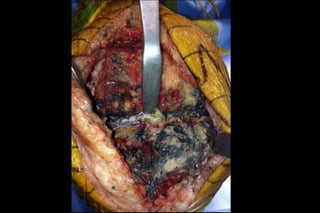
Osteoarthritis is a chronic disease with no cure that affects over 27 million Americans. It is the leading cause of disability in the US. While there are no disease modifying treatments, management focuses on non-operative options like exercise, weight loss, and medications. For severe osteoarthritis, total joint arthroplasty provides significant pain relief and functional improvement, but carries risks if patients have uncontrolled medical comorbidities. Referral for joint replacement requires exhausted non-surgical options and optimization of patient health to achieve the best outcomes.