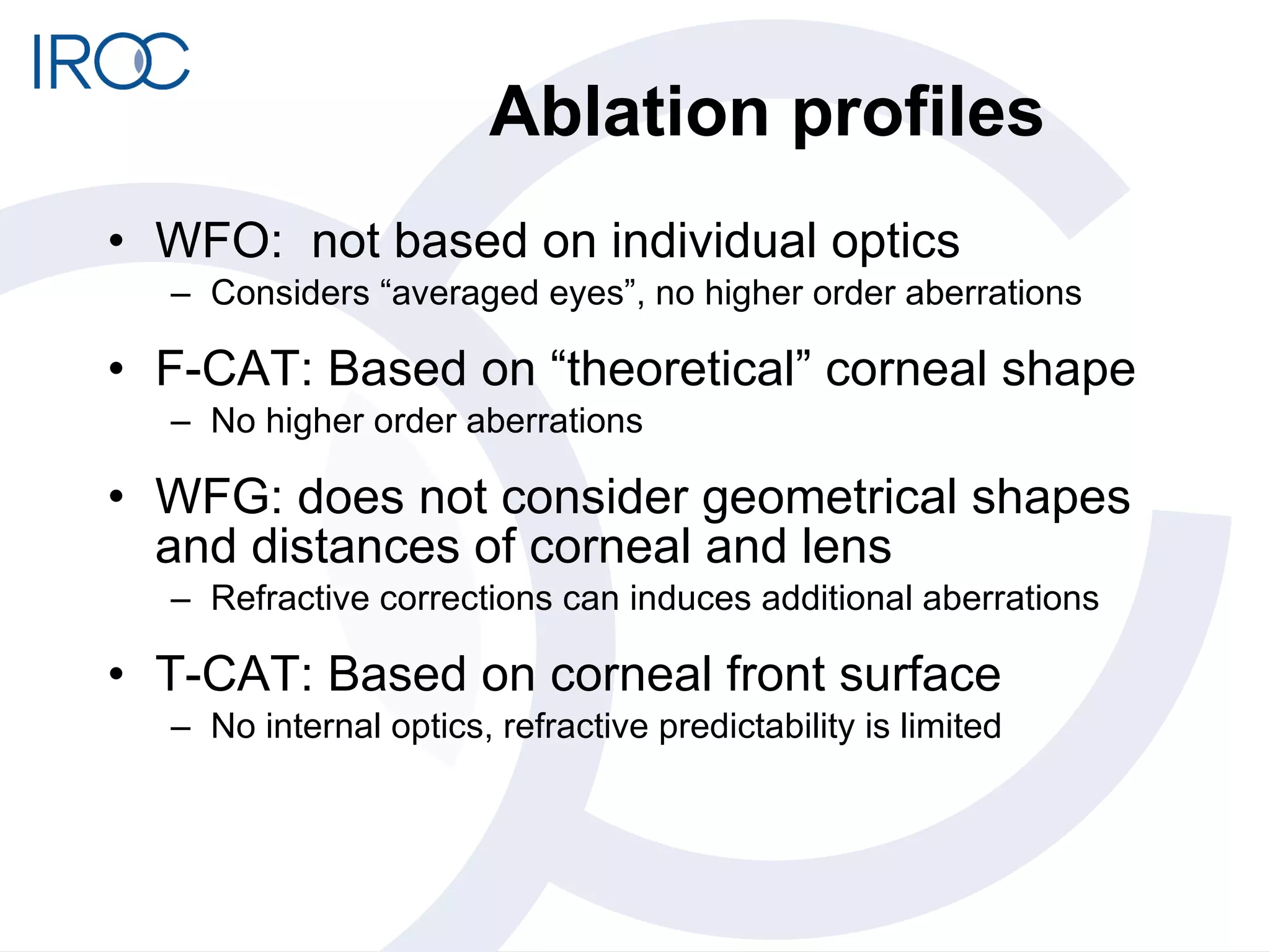
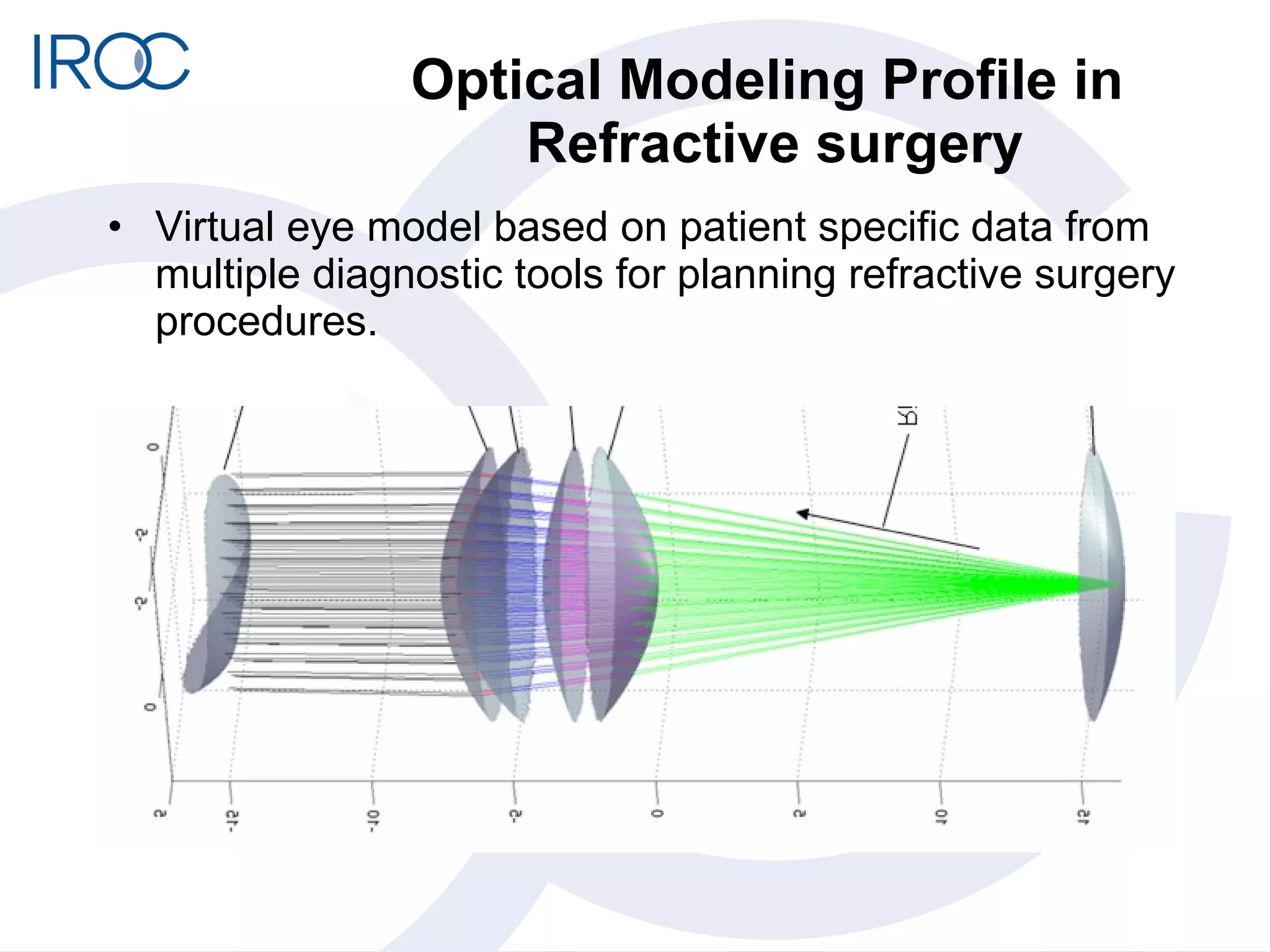
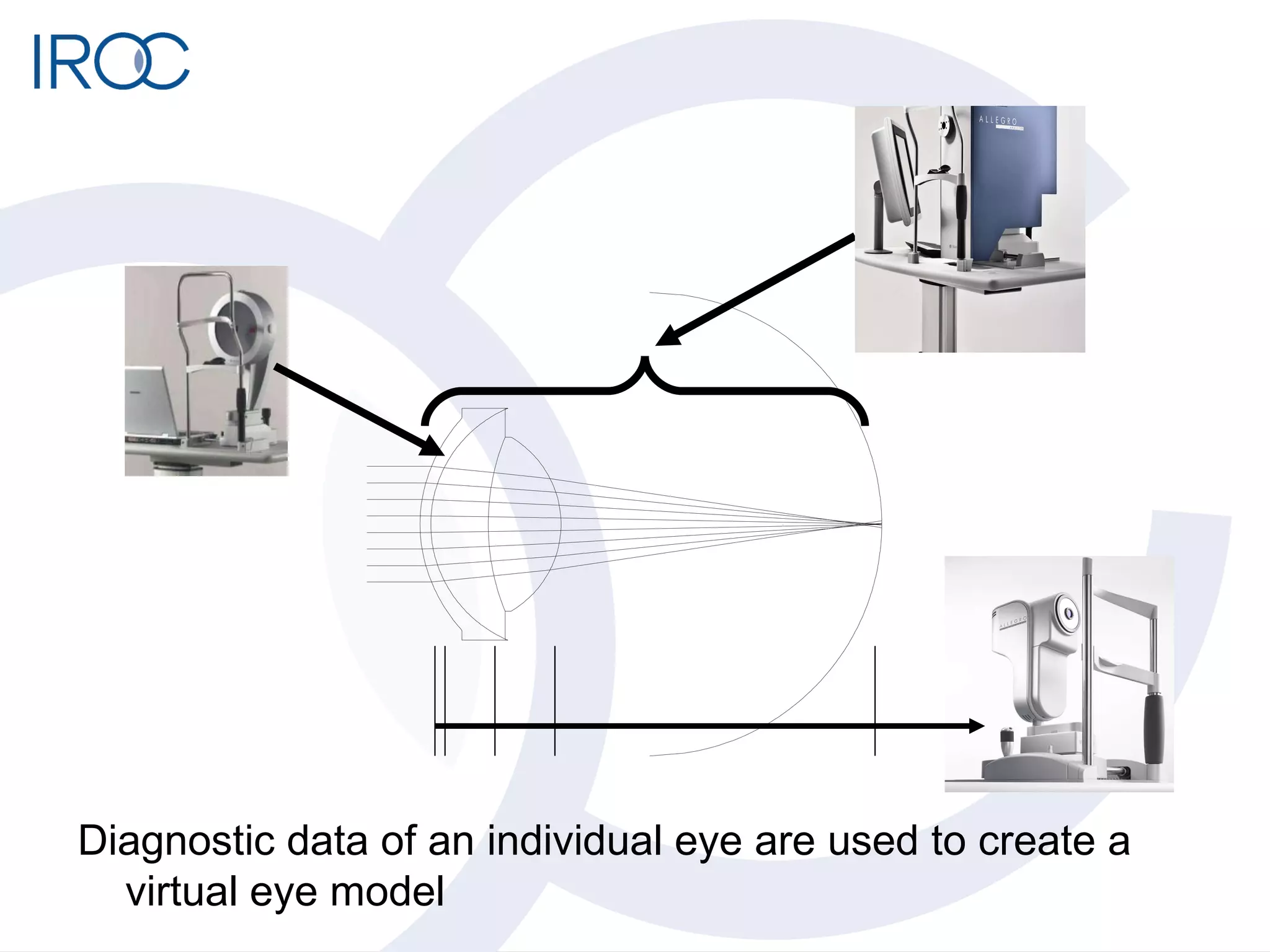
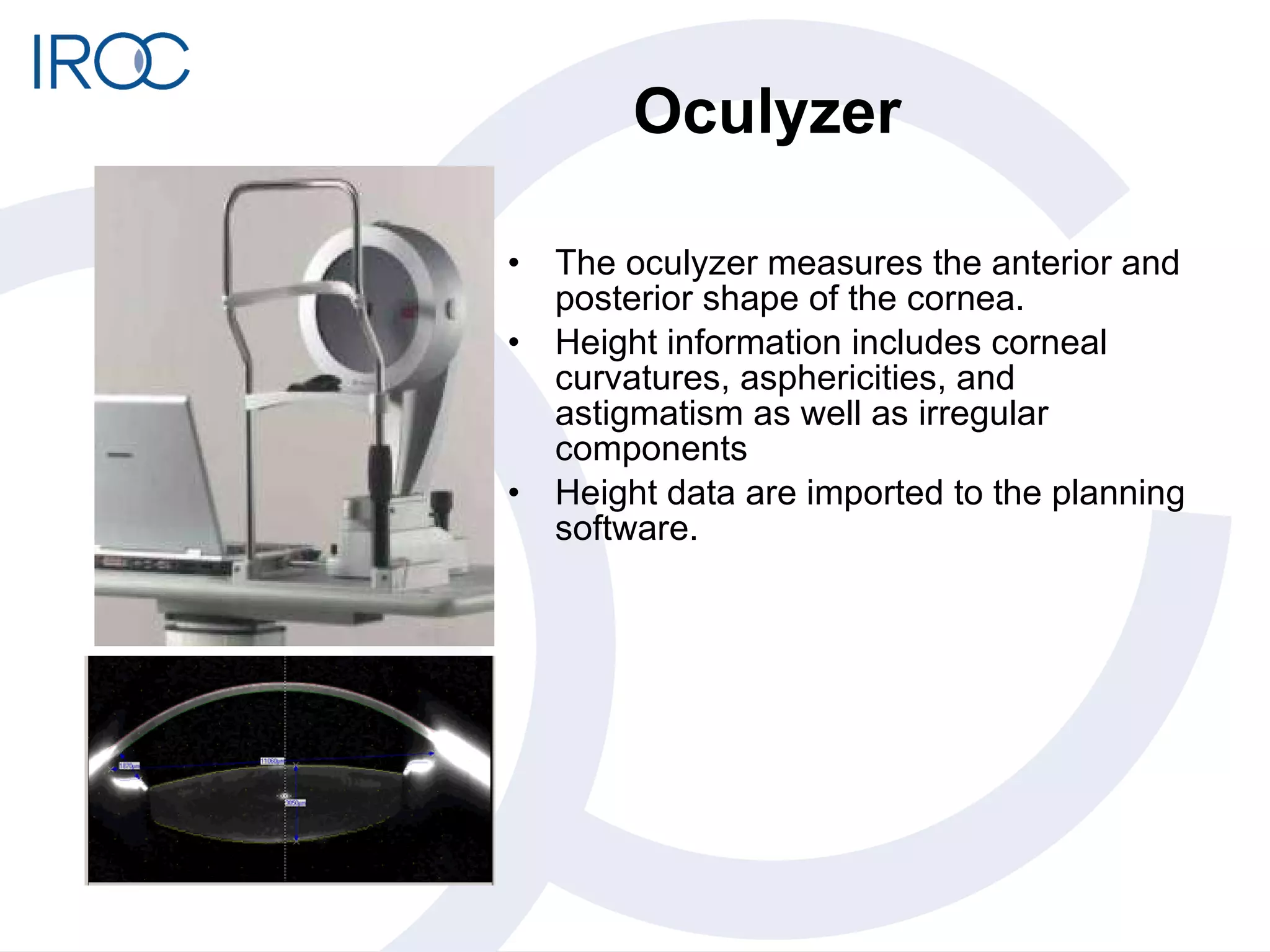
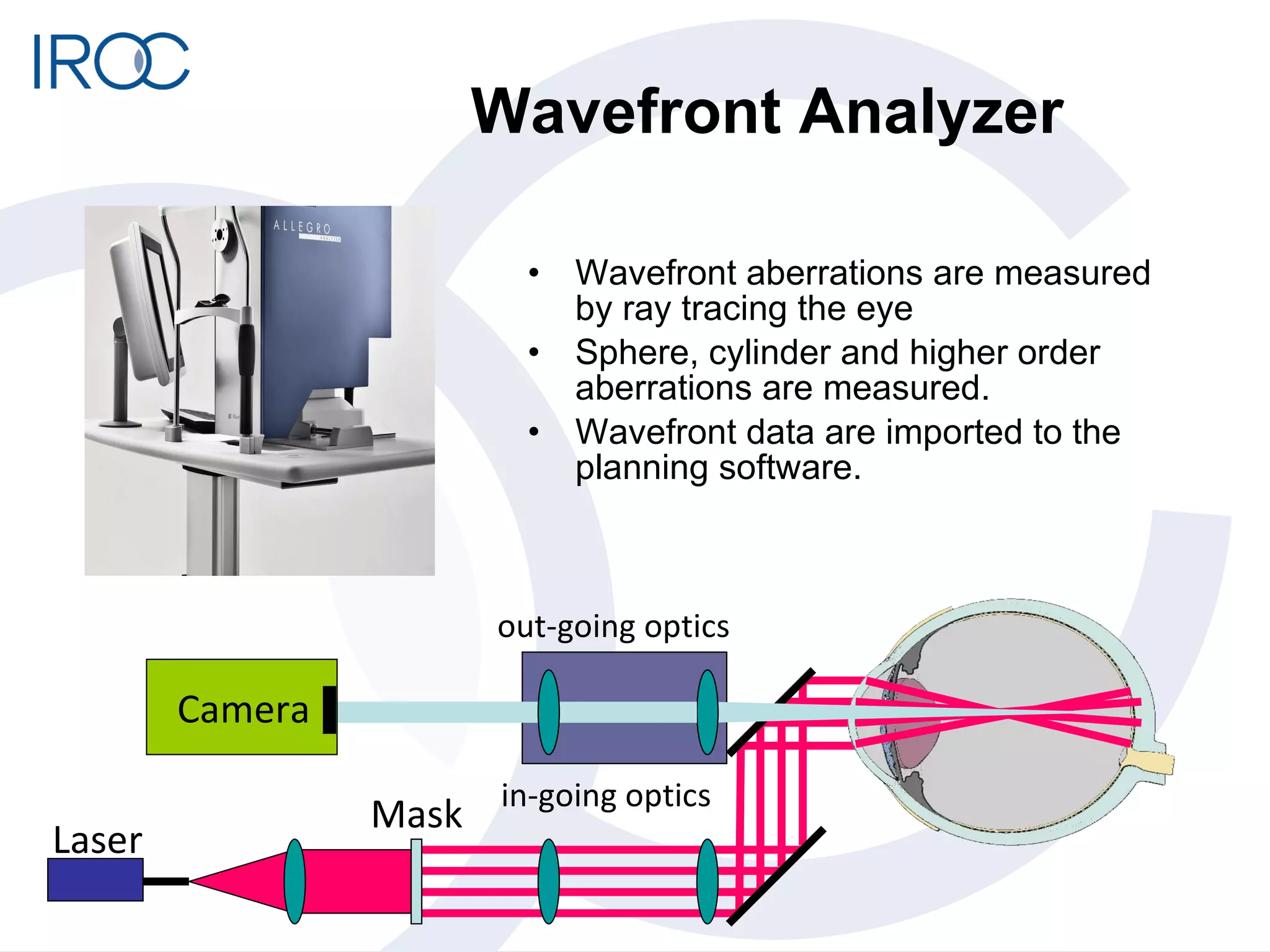
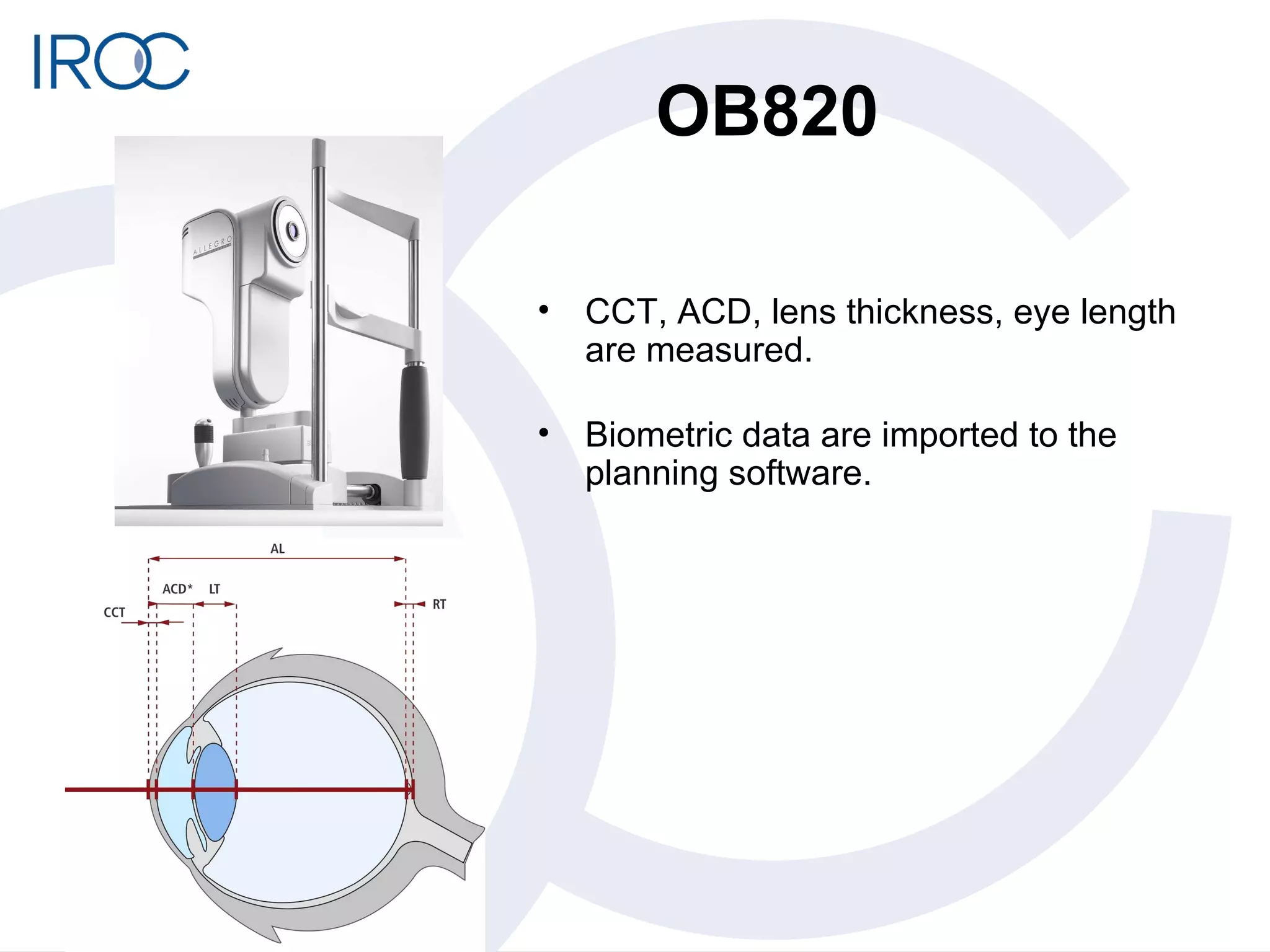
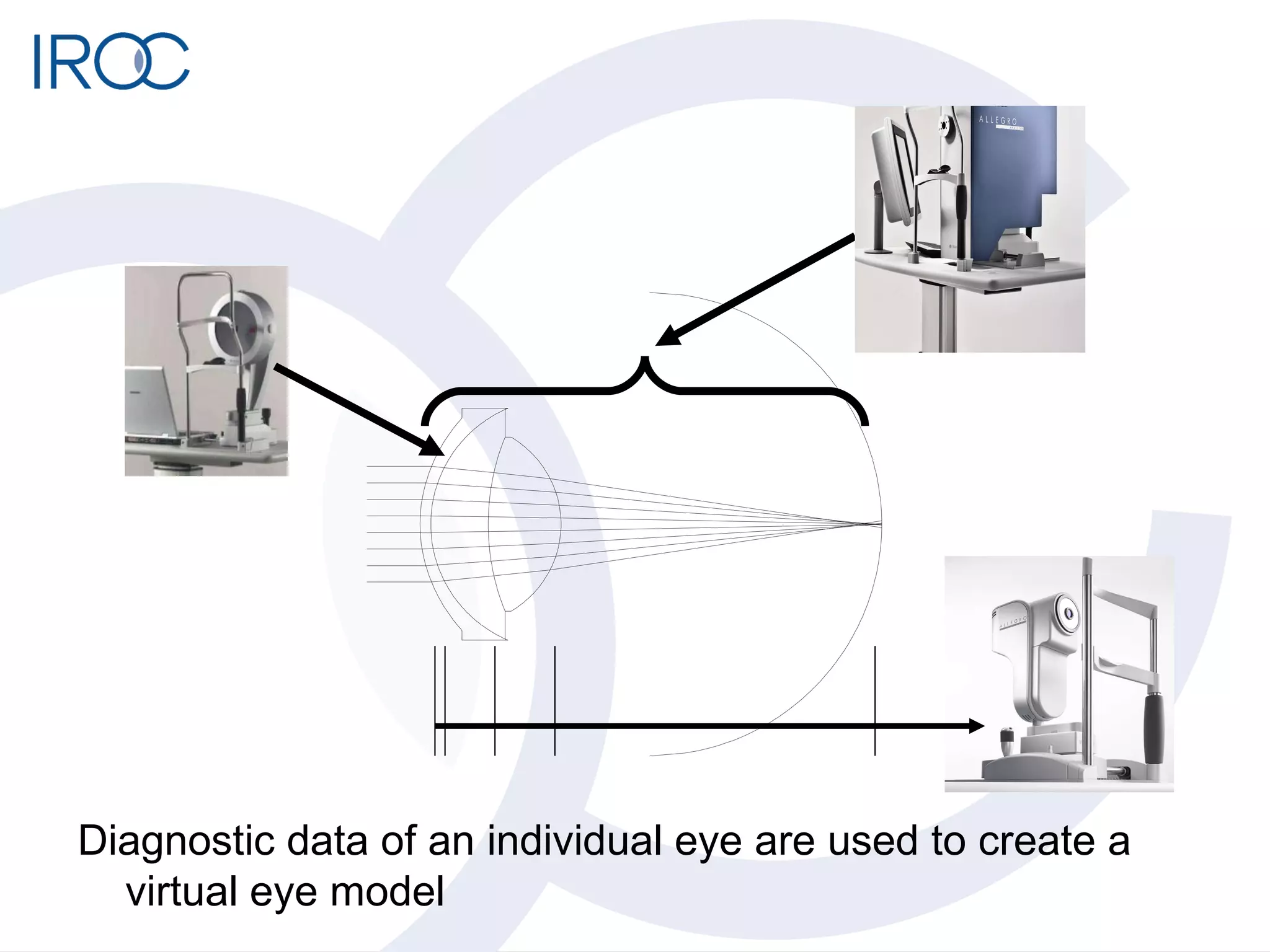
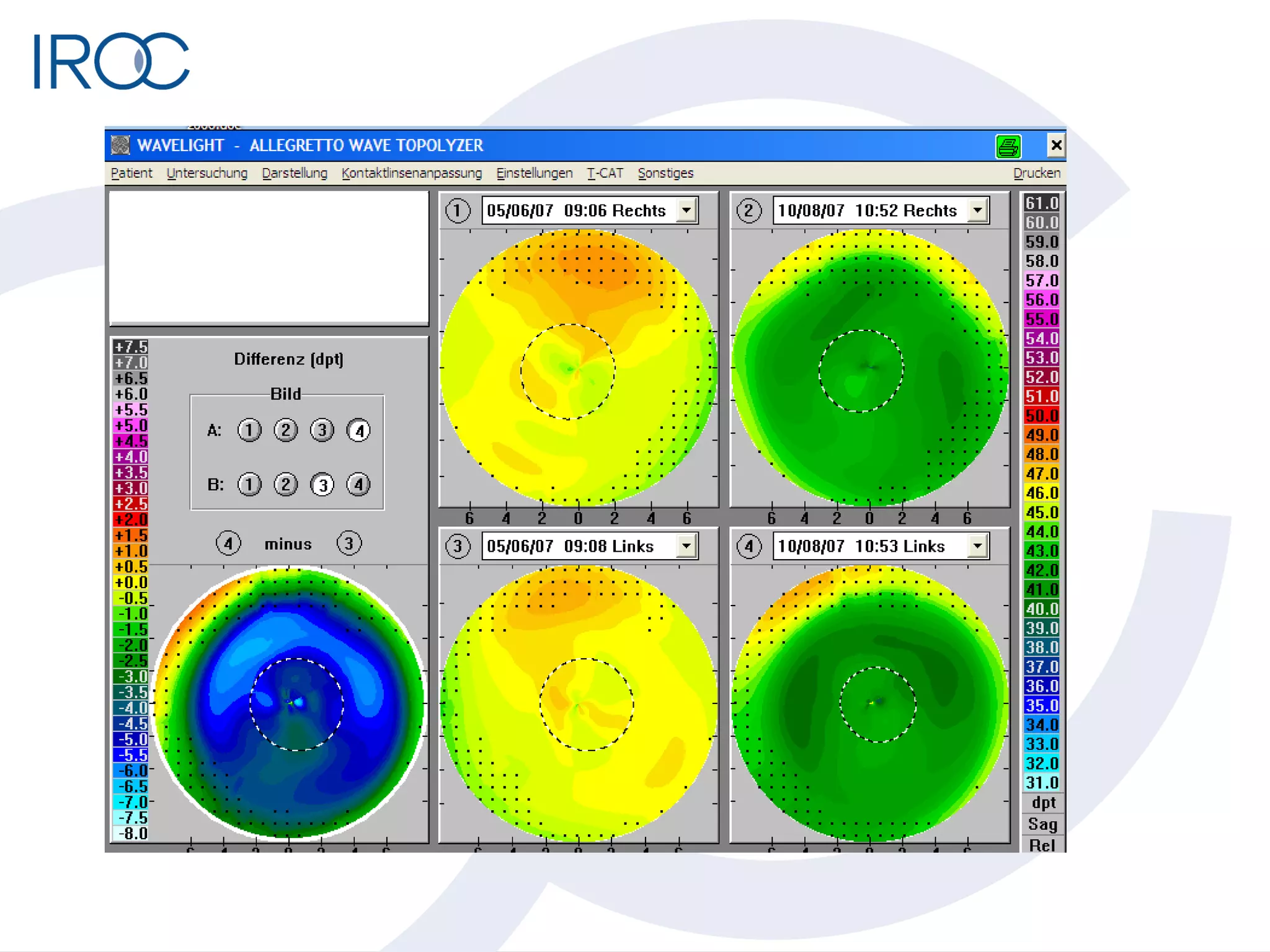

The document discusses optical modeling profiles used in refractive surgery planning. It describes how traditional profiles like WFO, F-CAT, and T-CAT do not consider individual eye optics and rely on averaged data. A new virtual eye model is presented that uses diagnostic data from tools like oculyzer, wavefront analyzer, and biometry to create a personalized eye model for each patient. Ray tracing is used to simulate refractive corrections and optimize ablation profiles. A clinical study showed the individualized ray tracing approach provided better refractive predictability compared to wavefront optimized treatments.