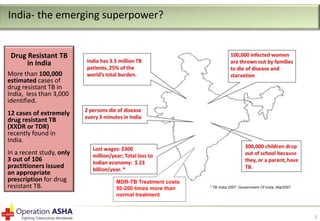
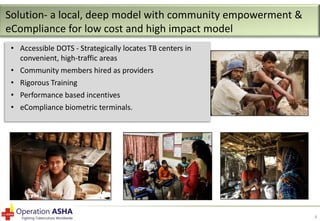
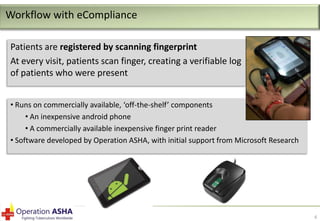
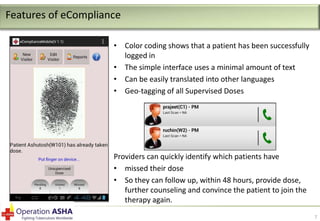
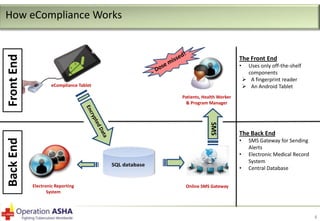
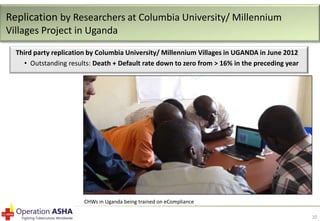
eCompliance is an electronic treatment monitoring system that uses biometric fingerprint scanning to ensure accuracy and adherence in tuberculosis (TB) treatment. It aims to curb the growth of multi-drug resistant TB (MDR-TB) by preventing missed and unsupervised doses. Field tests in India and Uganda found death and default rates reduced to zero compared to over 16% previously. eCompliance creates an indisputable record of each patient visit and drug dose taken by requiring fingerprint scans. This eliminates human errors in record keeping and gaps in treatment supervision that can lead to drug resistance. Initial results found it improved treatment motivation and outcomes while increasing health worker productivity by 30%.