Download to read offline

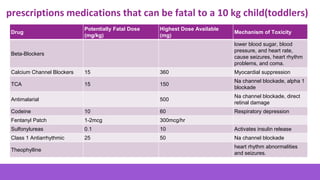
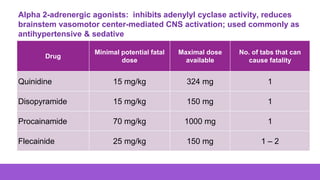
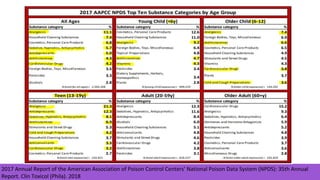

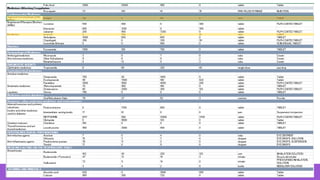
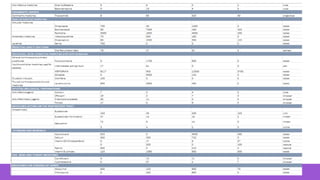




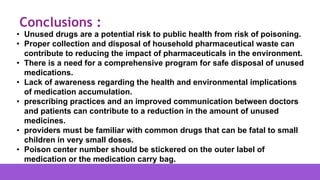


This document discusses medication safety and the dangers posed by common household medications to children. It notes that medicines are the leading cause of child poisoning, with nearly 52,000 children under age 6 seen in emergency rooms in 2017 for medicine poisoning. Several common medications are listed that can be fatal to a 10kg child in very small doses, such as a single pill. The document also discusses lethal drug interactions and the importance of safe medication disposal to prevent accidental poisoning. It concludes that awareness of potentially fatal medications and proper disposal are needed to protect public health.













































































