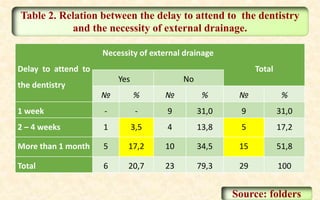
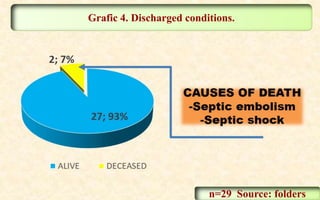
The study investigates the epidemiological and clinical characteristics of odontogenic facial cellulitis in patients at Farafenni General Hospital from October 2017 to May 2018, highlighting that odontogenic infections are life-threatening despite post-antibiotic improvements. Infections predominantly affect females and younger populations, particularly molars in the mandibular region, with a significant correlation between delays in seeking dental care and increased complications. Recommendations emphasize enhancing public awareness and preventive measures to promote timely dental visits.