The ultimate clinicalobjective of root canal treatment is the three-dimensional
obturation of the endodontic spaces after being completely cleaned, shaped, and
disinfected.
The aim of obturation is to establish a fluid-tight barrier with the aim of protecting
the periradicular tissues from microorganisms that reside in the oral cavity. While a
perfect airtight or hermatic seal is unachievable in reality, every effort should be
made to reach this target.
The filling must, therefore, completely and durably fill the root canal space so that
no empty spaces should remain.
According to the American Association of Endodontists “Obturation is the
method used to fill and seal a cleaned and shaped root canal using a root
canal sealer and core filling material.”
INTRODUCTION
2
3.
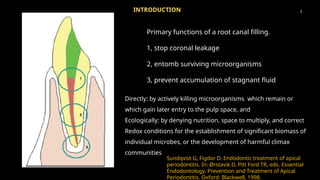
Primary functions ofa root canal filling.
1, stop coronal leakage
2, entomb surviving microorganisms
3, prevent accumulation of stagnant fluid
Sundqvist G, Figdor D. Endodontic treatment of apical
periodontitis. In: Ørstavik D, Pitt Ford TR, eds. Essential
Endodontology. Prevention and Treatment of Apical
Periodontitis. Oxford: Blackwell, 1998.
3
INTRODUCTION
Directly: by actively killing microorganisms which remain or
which gain later entry to the pulp space, and
Ecologically: by denying nutrition, space to multiply, and correct
Redox conditions for the establishment of significant biomass of
individual microbes, or the development of harmful climax
communities
4.
The achievement ofa “hermetic seal” is often cited as a major goal of
root canal treatment. According to accepted dictionary definitions, the
word hermetic means sealed against the escape or entry of air—or
made airtight by fusion or sealing.
HISTORICAL PERSPECTIVES
Endodontically speaking, the term hermetic is inappropriate; instead, terms
such as
fluid-tight, fluid-impervious, or bacteria-tight seals are more contemporary.
In 1924, Hatton indicated: “Perhaps there is no technical operation in dentistry or
surgery where so much depends on the conscientious adherence to high ideals as
that of pulp canal filling.”
4
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp, 11th edition
5.
5
Earlier rootcanals have been reported to be filled with Amalgam, Asbestos, Balsam, Bamboo, Cement,
Copper, Gold Foil, Iron, Lead, Oxychloride of Zinc, Paraffin, Pastes, Resin, Rubber, Silver Points, Tin
foils. Among all these materials tried none of them met the ideal requirements of an obturating
material.
The search for an suitable obturating material ended with the discovery of Gutta percha.
Gutta-percha is a name derived from two words
“GETAH”- meaning gum “PERTJA”- name of the tree in Malay language
Used in crude form by the natives of Malaysian archipelago for making knife handles, walking sticks
and for various other purposes.
R. Prakash, V. Gopikrishna, D.Kandaswamy, GUTTA-PERCHA – AN
UNTOLD STORY, ENDODONTOLOGY, 17 (2), 33-6
6.
The firstperson to discover this material was John Tradescant, who brought this material after his
travels from far-east in 1656, he named this material as “Mazer wood”.
The honour of introduction of this material goes to Dr. William Montogmerie, who was a medical
officer in Indian service.
In medicine, they were used as splints for holding fractured joints and manufacture of handles of
forceps, catheters etc.
It was earlier used to control hemorrhage in extracted socket wounds. They were also used for
skin diseases by the dermatologists, particularly against Small pox, Erysipelas, Psoriasis and
Eczema
R. Prakash, V. Gopikrishna, D.Kandaswamy, GUTTA-PERCHA – AN UNTOLD STORY,
ENDODONTOLOGY, 17 (2), 33-6
5
HISTORICAL PERSPECTIVES
7.
7
1800 s EdwinTruman introduced gutta percha as a temporary filling material in dentistry.
‟
1847 Hill developed the first gutta percha restorative material known as “Hill s Stopping” .
‟
1867 Bowman claimed to be the first to use gutta percha for a canal filling in an extracted molar .
1883 Perry claimed to use a pointed gold wire wrapped in gutta percha.
1887 S.S white company began to commercially manufacture gutta percha points.
1914 Callahan introduced softening and dissolution of gutta percha with use of rosins and used them for
obturation.
1959 Ingle and Levine proposed standardization of root canal instruments and filling materials and 1976
ISO was established.
1977 Thermoplasticized injectable gutta percha obturation was introduced to the profession.
R. Prakash, V. Gopikrishna, D.Kandaswamy, GUTTA-PERCHA – AN UNTOLD STORY,
ENDODONTOLOGY, 17 (2), 33-6
HISTORICAL PERSPECTIVES
8.
BIOLOGICAL CONSIDERATIONS FORROOT CANAL OBTURATION
In 1931, Rickert and Dixon proposed the “hollow tube” theory: an empty space within a
living organism tends to fill with tissue fluids within a short period of time.
This theory was based on the observation of an inflammatory reaction around the ends of
hollow steel and platinum anesthetic needle fragments implanted in experimental
animals. This reaction did not occur if the implant was made of a solid, non-porous
material.
Two years later, Coolidge arrived at the conclusion that, just as within unfilled or
underfilled root canals, fluids that accumulate within empty spaces are rapidly colonized
by microorganisms reaching these spaces by means of “anachoresis” and causing
inflammtory reaction.
Rickert UG, Dixon CM Jr. The controlling of root surgery. In: Transaction of
the eight International Dental Congress. Paris: Federation Dentaire
International; 1931:15–22.
8
9.
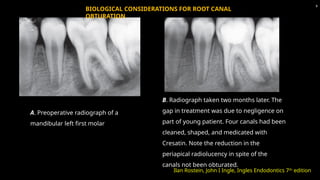
A. Preoperative radiographof a
mandibular left first molar
B. Radiograph taken two months later. The
gap in treatment was due to negligence on
part of young patient. Four canals had been
cleaned, shaped, and medicated with
Cresatin. Note the reduction in the
periapical radiolucency in spite of the
canals not been obturated.
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
9
BIOLOGICAL CONSIDERATIONS FOR ROOT CANAL
OBTURATION
10.
SELECTING THE CORRECTTIME FOR OBTURATION
The tooth is asymptomatic and the patient must feel perfectly
comfortable.
There is no exudate from the canal.
The canal can be properly dried.
There is no foul odor indicating the presence of microorganisms.
The temporary filling is intact if the root canal has been shaped in a
previous visit.
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
10
11.
Vital Pulp Tissue
At present, the consensus is that one-step treatment procedures are acceptable when the
patient exhibits a completely or partially vital pulp.
Obturation at the initial visit also precludes contamination as a result of leakage during the
period between patient visits.
Elective root canal treatment for restorative reasons can be completed in one visit provided
the pulp is vital, to some degree, and time permits.
When pain occurs as the result of irreversible pulpitis, obturation can occur at the initial visit
because removal of the vital tissue will generally resolve the patient’s pain.
11
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp,
11th edition
SELECTING THE CORRECT TIME FOR
OBTURATION
12.
Necrotic Pulp Tissue
Patients who present with pulp necrosis with or without asymptomatic periradicular
pathosis (asymptomatic apical periodontitis, chronic apical abscess, condensing osteitis)
may be treated in one visit, based on the best available information.
When patients present with acute symptoms caused by pulp necrosis and acute
periradicular abscess, obturation is generally delayed until the patient is asymptomatic.
However, more than 20 years ago, investigators demonstrated that cases with soft-tissue
swelling could be completed in one visit with appropriate endodontic treatment, incision
for drainage, and a regimen of antibiotics.
Management of these patients, however, may be more difficult should problems persist or
become
worse after the completion of treatment.
12
SELECTING THE CORRECT TIME FOR
OBTURATION
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp,
11th edition
13.
13
• One situationthat contraindicates single-visit care is the presence and persistence of exudation
in the canal during preparation. The potential for post-treatment exacerbation is increased if the
periapical lesion is productive and generates continual suppuration.
• If the canal is sealed, pressure and corresponding tissue destruction may proceed rapidly. In
these cases, canal preparation is completed, followed by calcium hydroxide placement.
• A dry cotton pellet is placed over the calcium hydroxide and the access is sealed with a
temporary restoration. Generally, exudation will be diminished and controllable at a subsequent
appointment; obturation may then be completed.
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION): Walton & Torabinejad
SELECTING THE CORRECT TIME FOR OBTURATION
In general,obturation can be performed after cleaning and shaping procedures
when the canal can be dried and the patient is not experiencing swelling.
An exception is the presence or persistence of exudation from the canal.
Obturation of a canal that cannot be dried is contraindicated.
Procedural concerns also dictate the time of obturation. Difficult cases may
require
more time for preparation and can be managed more uneventfully in multiple
appointments. Patients may require multiple short appointments because of
medical
conditions, their psychological state of mind, and fatigue.
15
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp, 11th
edition
16.
Apical limit ofroot canal instrumentation and obturation, part 1.
Literature review International Endodontic Journal (1998) 31, 384-
393
APICAL EXTENT OF OBTURATION
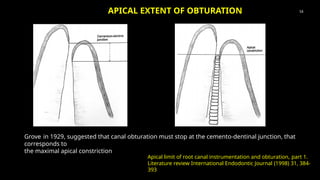
Grove in 1929, suggested that canal obturation must stop at the cemento-dentinal junction, that
corresponds to
the maximal apical constriction
16
17.
• Ricucci andLangeland suggested that the apical limit of canal
instrumentation and obturation should be the “apical constriction.”
• This anatomical location, however, cannot be determined clinically with
accuracy since it is “ever-changing”; it has been demonstrated as far as
3.8 mm from the anatomic apex.
• Others suggest that the arbitrary rule that canal preparation should
terminate 1 mm short of the radiographic apex should not be accepted
in modern endodontic therapy.
• The “one millimeter” technique could result in instrumentation short of
the true canal terminus, possibly leaving necrotic and infected debris
behind, leading to treatment failure.
• According to Schilder, having three-dimensionally obturated root canal as
far as 0.5–1 mm from the radiographic terminus of the canal is in
practice equivalent to having filled it completely, leading to the success
of the therapy.
17
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
18.
Generally, root canalfilling materials are divided into
Pastes and Cements,
Solid materials
Semi-solid Materials.
Methods of filling root canals:principles and practices,
Endodontic Topics 2005, 12, 2–24
18
ROOT CANAL FILLING MATERIALS
19.
19
PASTES AND
CEMENTS
Sealers areself-hardening cements used in conjunction with solid or semi-solid
materials that serve as the core of the obturation.
Sometimes, clinicians use certain cements to fill the entire root canal without
another core obturation material.
Root canal sealers are used in conjunction with biologically acceptable semisolid or
solid obturating materials to establish an adequate seal of the root canal
system( Grossman )
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
20.
20
Seal thespace between the obturating core material and the internal root
surface
Fill the space between core and accessory filling materials in lateral
condensation
Seal the irregularities of the complex canal anatomy for example, lateral
canals and tubules
Lubricate and facilitate seating of the core and accessory filling material
Deliver antibacterial properties to the obturation system
Role of sealers
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
Sealers can bebroadly categorised into the following
groups:
o Zinc oxide eugenol-based
o Calcium hydroxide-based
o Glass ionomer-based
o Resin-based
o Calcium silicate-based
o Silicone-based
o Medicated sealers
R. M. E. Tomson, N. Polycarpou and P. L. Tomson Contemporary obturation of the root canal
system, BRITISH DENTAL JOURNAL VOLUME 216 NO. 6 MAR 21 2014
22
Types of sealers
23.
23
Zinc oxide eugenol-based
Grossman’sFormula of a Nonstaining
Sealer 1958
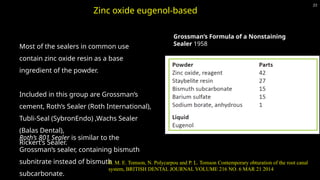
Most of the sealers in common use
contain zinc oxide resin as a base
ingredient of the powder.
Included in this group are Grossman’s
cement, Roth’s Sealer (Roth International),
Tubli-Seal (SybronEndo) ,Wachs Sealer
(Balas Dental),
Rickert’s Sealer.
Roth’s 801 Sealer is similar to the
Grossman’s sealer, containing bismuth
subnitrate instead of bismuth
subcarbonate.
R. M. E. Tomson, N. Polycarpou and P. L. Tomson Contemporary obturation of the root canal
system, BRITISH DENTAL JOURNAL VOLUME 216 NO. 6 MAR 21 2014
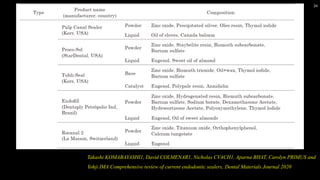
24.
24
Takashi KOMABAYASHI1, DavidCOLMENAR1, Nicholas CVACH1, Aparna BHAT, Carolyn PRIMUS and
Yohji IMA Comprehensive review of current endodontic sealers, Dental Materials Journal 2020
25.
25
Takashi KOMABAYASHI1, DavidCOLMENAR1, Nicholas CVACH1, Aparna BHAT, Carolyn PRIMUS and
Yohji IMA Comprehensive review of current endodontic sealers, Dental Materials Journal 2020
26.
26
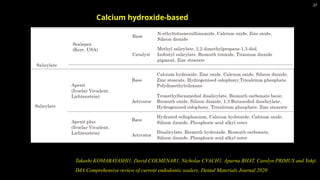
• Grossman’s cementhardens in approximately 2 hours at 37°C and 100% relative humidity.
• It begins to set in the root canal within 10–30 minutes because of the moisture present in
dentin.
• The setting time is also influenced by the quality of the zinc oxide and the pH of the resin
used, the care and technique in mixing the cement to its proper consistency, the amount of
humidity in the atmosphere, and the temperature and dryness of the mixing slab and
spatula.
• Tubli-Seal has been shown to have a setting time of approximately one hour.
• Setting time of Proco-Sol varies by an order of magnitude (40.5 min to 42 h).
Properties of zinc oxide eugenol based
sealers
Takashi KOMABAYASHI1, David COLMENAR1, Nicholas CVACH1, Aparna BHAT, Carolyn PRIMUS
and Yohji IMA Comprehensive review of current endodontic sealers, Dental Materials Journal 2020
27.
27
Takashi KOMABAYASHI1, DavidCOLMENAR1, Nicholas CVACH1, Aparna BHAT, Carolyn PRIMUS and Yohji
IMA Comprehensive review of current endodontic sealers, Dental Materials Journal 2020
Calcium hydroxide-based
28.
28
Takashi KOMABAYASHI1, DavidCOLMENAR1, Nicholas CVACH1, Aparna BHAT, Carolyn PRIMUS and Yohji
IMA Comprehensive review of current endodontic sealers, Dental Materials Journal 2020
Noneugenol
Sealers
Glass Ionomer Sealers
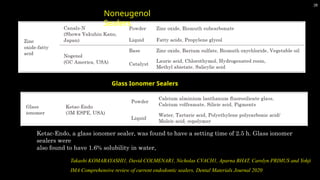
Ketac-Endo, a glass ionomer sealer, was found to have a setting time of 2.5 h. Glass ionomer
sealers were
also found to have 1.6% solubility in water,
29.
29
Takashi KOMABAYASHI1, DavidCOLMENAR1, Nicholas CVACH1, Aparna BHAT, Carolyn PRIMUS
and Yohji IMA Comprehensive review of current endodontic sealers, Dental Materials Journal 2020
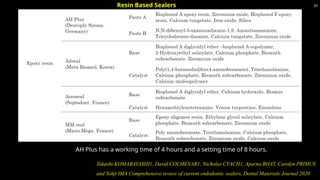
AH Plus has a working time of 4 hours and a setting time of 8 hours.
Resin Based Sealers
30.
30
Methacrylate Resin Sealers
Fourgenerations of methacrylate resin–based root canal sealers have been marketed for
commercial use
First generation:
The first generation of hydrophilic methacrylate resin–based material (Hydron; Hydron
Technologies, Inc., Boca Raton, Florida) was designed for en masse root filling and
appeared in the mid 1970s.
The major component of Hydron was poly[2-hydroxyethyl methacrylate] (poly[HEMA]),
which was injected into a root canal and polymerized in situ within the canal space
without the adjunctive use of a root-filling material.
Hydron became obsolete in the 1980s as subsequent clinical findings were unacceptable.
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp, 11th
edition
31.
31
• The secondgeneration of bondable sealer is non etching and hydrophilic in nature and
does not require the adjunctive use of a dentin adhesive.
• It is designed to flow into accessory canals and dentinal tubules to facilitate resin tag
formation for retention and seal after smear layer removal with NaOCl and EDTA.
• The sealer was found to seal best when applied to slightly moist intraradicular dentin.
• EndoREZ is recommended for use with either a conventional gutta-percha cone or with
specific EndoREZ points (resin-coated gutta-percha)
Second generation
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways
of the pulp, 11th edition
32.
32
Kenneth M. Hargreaves,Louis H. Berman, Cohen’s Pathways of the pulp, 11th edition
Third generation
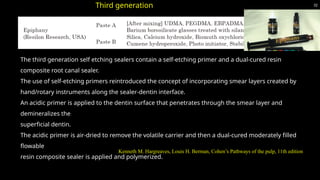
The third generation self etching sealers contain a self-etching primer and a dual-cured resin
composite root canal sealer.
The use of self-etching primers reintroduced the concept of incorporating smear layers created by
hand/rotary instruments along the sealer-dentin interface.
An acidic primer is applied to the dentin surface that penetrates through the smear layer and
demineralizes the
superficial dentin.
The acidic primer is air-dried to remove the volatile carrier and then a dual-cured moderately filled
flowable
resin composite sealer is applied and polymerized.
33.
33
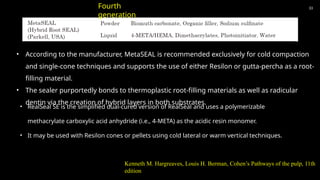
• According tothe manufacturer, MetaSEAL is recommended exclusively for cold compaction
and single-cone techniques and supports the use of either Resilon or gutta-percha as a root-
filling material.
• The sealer purportedly bonds to thermoplastic root-filling materials as well as radicular
dentin via the creation of hybrid layers in both substrates.
Fourth
generation
• RealSeal SE is the simplified dual-cured version of RealSeal and uses a polymerizable
methacrylate carboxylic acid anhydride (i.e., 4-META) as the acidic resin monomer.
• It may be used with Resilon cones or pellets using cold lateral or warm vertical techniques.
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp, 11th
edition
35
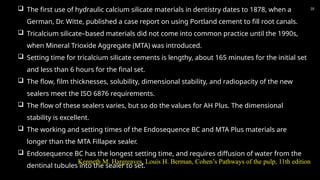
The firstuse of hydraulic calcium silicate materials in dentistry dates to 1878, when a
German, Dr. Witte, published a case report on using Portland cement to fill root canals.
Tricalcium silicate–based materials did not come into common practice until the 1990s,
when Mineral Trioxide Aggregate (MTA) was introduced.
Setting time for tricalcium silicate cements is lengthy, about 165 minutes for the initial set
and less than 6 hours for the final set.
The flow, film thicknesses, solubility, dimensional stability, and radiopacity of the new
sealers meet the ISO 6876 requirements.
The flow of these sealers varies, but so do the values for AH Plus. The dimensional
stability is excellent.
The working and setting times of the Endosequence BC and MTA Plus materials are
longer than the MTA Fillapex sealer.
Endosequence BC has the longest setting time, and requires diffusion of water from the
dentinal tubules into the sealer to set.
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp, 11th edition
36.
36
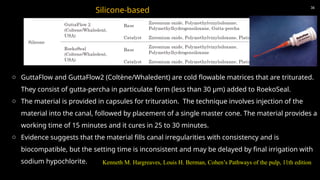
Silicone-based
o GuttaFlow andGuttaFlow2 (Coltène/Whaledent) are cold flowable matrices that are triturated.
They consist of gutta-percha in particulate form (less than 30 μm) added to RoekoSeal.
o The material is provided in capsules for trituration. The technique involves injection of the
material into the canal, followed by placement of a single master cone. The material provides a
working time of 15 minutes and it cures in 25 to 30 minutes.
o Evidence suggests that the material fills canal irregularities with consistency and is
biocompatible, but the setting time is inconsistent and may be delayed by final irrigation with
sodium hypochlorite. Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp, 11th edition
37.
37
Sealers containingparaformaldehyde are strongly contraindicated in endodontic
treatment. Although the lead and mercury components may have been removed from
these zinc oxide–eugenol formulations over time, the severely toxic paraformaldehyde
content has remained a constant.
These sealers are not approved by the U.S. Food and Drug Administration and are
unacceptable under any circumstances in clinical treatment because of the severe and
permanent toxic effects on periradicular tissues.
Sealers in this category include Endomethasone, SPAD, Reibler’s Paste.
Medicated Sealers
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp, 11th
edition
38.
38
Takashi KOMABAYASHI1, DavidCOLMENAR1, Nicholas CVACH1, Aparna BHAT, Carolyn PRIMUS and
Yohji IMA Comprehensive review of current endodontic sealers, Dental Materials Journal 2020
39.
Pulp diagnosisas vital or necrotic is important for selection of an endodontic sealer for
clinical use. In vital pulp (pulpitis) cases, the therapeutic effects of sealers are not
necessary under the asepsis technique non surgical root canal treatment.
In necrotic pulp cases, especially cases with large apical radiolucency, the therapeutic
effects of tricalcium silicate-based sealers are useful.
A medicated sealer to kill bacteria should increase the chances of long-term success.
Cases of large apical radiolucency diagnosed with questionable or unfavorable
prognoses are expected to benefit from sealer-driven therapeutic effects.
39
SEALER SELECTION
Takashi KOMABAYASHI1, David COLMENAR1, Nicholas CVACH1, Aparna BHAT, Carolyn PRIMUS
and Yohji IMA Comprehensive review of current endodontic sealers, Dental Materials Journal 2020
40.
40
While tricalcium silicatesealers show the least leakage, they have slow setting
times. Therefore, tricalcium silicate sealers are not a good choice if post/core/build-
up must occur on the same day together with endodontic obturation.
Salicylate-based (calcium-hydroxide-containing) are good choices if post/core/build-
up is performed immediately after completion of endodontic obturation.
SEALER SELECTION
Takashi KOMABAYASHI1, David COLMENAR1, Nicholas CVACH1, Aparna BHAT, Carolyn PRIMUS and Yohji IMA
Comprehensive review of current endodontic sealers, Dental Materials Journal 2020
41.
Various methods ofsealer placement have been advocated,
including the master cone, lentulo spirals, files and reamers, and
ultrasonics.
Investigators compared sealer placement using a file rotated
counterclockwise, the lentulo spiral, an ultrasonic file, and coating
the master gutta-percha cone.
Placement did not differ with the various techniques; however,
the investigators noted the most variation in sealer coating was in
the apical area.
Another study compared sealer placement with a K-type file, the
lentulo spiral, and using the master cone in curved canals. Results
demonstrated no significant differences in the techniques after
obturation.
41
SEALER PLACEMENT
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp, 11th edition
42.
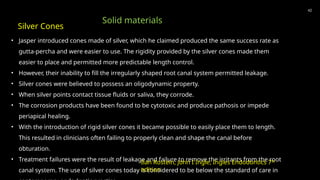
• Jasper introducedcones made of silver, which he claimed produced the same success rate as
gutta-percha and were easier to use. The rigidity provided by the silver cones made them
easier to place and permitted more predictable length control.
• However, their inability to fill the irregularly shaped root canal system permitted leakage.
• Silver cones were believed to possess an oligodynamic property.
• When silver points contact tissue fluids or saliva, they corrode.
• The corrosion products have been found to be cytotoxic and produce pathosis or impede
periapical healing.
• With the introduction of rigid silver cones it became possible to easily place them to length.
This resulted in clinicians often failing to properly clean and shape the canal before
obturation.
• Treatment failures were the result of leakage and failure to remove the irritants from the root
canal system. The use of silver cones today is considered to be below the standard of care in
42
Silver Cones
Solid materials
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
43.
1. They donot adapt well to the inner canal anatomy. The canal will, therefore, remain
inadequately obturated or mostly filled with sealer.
2. The canal often has an irregular shape; it is elliptical, eccentric, and the apical foramen
doesn’t have a round cross-section like the silver point. As a result, the silver point will only
touch the walls in two points, will not be able to seal an elliptical foramen, and consequently
filling mishaps may occur.
3. If the silver point is positioned at the apical foramen, or protruding beyond the apex, once
the surrounding sealer has been resorbed, metallic corrosion sets in as a result of oxidation.
This leads to the formation of cytotoxic byproducts containing sulfur and chloride.
43
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
DISADVANTAGES
44.
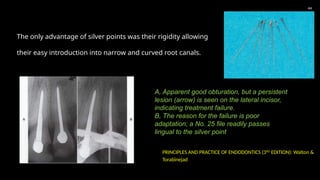
The only advantageof silver points was their rigidity allowing
their easy introduction into narrow and curved root canals.
44
A, Apparent good obturation, but a persistent
lesion (arrow) is seen on the lateral incisor,
indicating treatment failure.
B, The reason for the failure is poor
adaptation; a No. 25 file readily passes
lingual to the silver point
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION): Walton &
Torabinejad
45.
45
Files usedas core materials are an interesting concept.
Because preparation is accomplished with files, why not fill the canal with sealer, force or "screw" a file
into place at the correct working length, and then cut it at the canal orifice? This technique has not gained
popular acceptance, although there have been advocates.
A major disadvantage is that, because of their design and the complexity of root canals, files do not
provide a complete seal.
Their fluting precludes a close fit, and sealer will not occupy the rest of the space.
In addition, retrieval is difficult if retreatment or a post space is needed.
Files as a primary core material are contraindicated.
Files
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION): Walton & Torabinejad
46.
46
Why not developa paste or cement that can be mixed in a liquid or putty form, inject the material to length, fill the
entire canal, and then allow the material to set? This would be fast, the paste would fill the entire canal space, and
obturation would be much simpler.
In addition, this method would permit use of a material that would adhere to dentin and create an absolute seal.
PASTES (SEMISOLIDS)
It has been suggested that a resin based sealer such as AH 26 and Diaket be used as the sole
obturating material.
These sealers have the same disadvantages as pastes and, therefore, have not attained popular use.
Resins
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION):
Walton & Torabinejad
47.
47
Zinc oxideand eugenol may be mixed pure (no additives) to intermediate thickness.
Other formulations combine zinc oxide-eugenol (ZnOE) with various additives.
The types known as N2 (A paste containing 6.5% paraformaldehyde as well as lead and mercury was
advocated
for use by Sargenti) or RC2B are most common.
These are derivations of Sargenti's formula and contain opaquers, metallic oxides (lead) or chlorides
(mercuric), steroids (at times), plasticizers, paraformaldehyde, and various other ingredients.
Claims of antimicrobial properties, biologic therapeutic activity, and superiority are made for these paste
formulations; no proof exists that they contribute any beneficial aspects to obturation.
Zinc Oxide and Eugenol
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION):
Walton & Torabinejad
48.
48
MTA can beused as a canal obturation material because of its superior physiochemical and
bioactive properties.
Mineral trioxide aggregate (MTA)
Indications
According to Bogen et al., the following are the applications of MTA:
1. MTA obturation combined with root-end resection
2. Teeth with open apices
3. Retreatment with MTA obturation
4. Internal resorption
5. Dens in dente
Limitations
Difficulty in retreatment following MTA obturation,
especially in curved canals
Potential for discoloration, especially when used in the
anterior esthetic zone
49.
49
Techniques of Placement
Itis accomplished using a syringe-type device with a barrel and special needles. The paste is mixed and
placed in the barrel, a screw handle is inserted and twisted, and the paste is extruded through the special
needle-like tips.
The needles are placed deep in the canal, and the paste is expressed as the needles are slowly backed out
of the canal. Advocates claim that this method completely fills the canal from the apical portion to the canal
orifice.
Injection
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION): Walton &
Torabinejad
50.
50
It isdone with lentulo spiral drills.
The paste is mixed, the drill is coated, and then it is placed and spun deep in the canal.
As with the syringe device, the canal is supposedly filled with paste as the drill is slowly
withdrawn.
Instrument placement
The advantages are obvious: paste techniques are fast and relativity easy to use and involve the use
of a single material.
The equipment needed, at least with the lentulo spiral technique, is relatively simple, comprising only a limited
assortment of special drills.
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION): Walton & Torabinejad
Advantages of Pastes
51.
51
PRINCIPLES AND PRACTICEOF ENDODONTICS (3RD
EDITION): Walton & Torabinejad
First, the universal problem with any nonsolid core material is length control. It is difficult to avoid
overfills or underfills.
Theoretically, radiographs should be made many times during obturation to assess length and density
as the material is being injected or placed.
Obviously, this is time consuming and subjects the patient to needless radiation.
Another major disadvantage is sealability. These techniques seal inconsistently: sometimes well,
other times poorly.
This unpredictability may be related to three factors: (1) large voids or discrepancies within the
material or adjacent to the walls; (2) shrinkage of ZnOE on setting, which leaves a space for
microleakage; and (3) solubility of pastes in tissue or oral fluids. In addition, injection devices are
difficult to clean and maintain.
Disadvantages
52.
Gutta-percha is themost popular core material used for obturation.
Gutta-percha is a dried coagulated extract of plants of Palaquium, Blanco genus of Sapotaceae family. These trees
are natural inhabitants of South East Asia, particularly Malaysian and Indonesian archipelago. Gutta percha is
white in color as squeezed from the trees. The Gutta-percha yielding trees are medium to tall trees, in which a
series of cuts (concentric or v- shaped cuts) are made to obtain the juice. The leaves of these trees also contribute
to a minimal extent in Gutta-percha production.
INDIGENOUS SOURCES
In India the species of this genus is very scanty. The species found are Palaquium obavatum, Palaquium
polyanthum, Palaquium ellipticum and palaquium gutta trees in Assam and Western ghats.
Palaquium gutta was recently introduced and planted in Botanical gardens, Bangalore.
52
Gutta-Percha
R. Prakash, V. Gopikrishna, D.Kandaswamy, GUTTA-PERCHA – AN
UNTOLD STORY, ENDODONTOLOGY, 17 (2), 33-6
53.
53
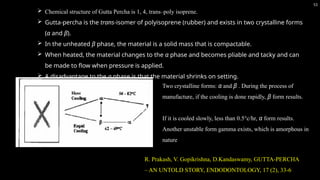
Chemical structureof Gutta Percha is 1, 4, trans–poly isoprene.
Gutta-percha is the trans-isomer of polyisoprene (rubber) and exists in two crystalline forms
(α and β).
In the unheated β phase, the material is a solid mass that is compactable.
When heated, the material changes to the α phase and becomes pliable and tacky and can
be made to flow when pressure is applied.
A disadvantage to the α phase is that the material shrinks on setting.
Two crystalline forms: α and β . During the process of
manufacture, if the cooling is done rapidly, β form results.
If it is cooled slowly, less than 0.5°c/hr, α form results.
Another unstable form gamma exists, which is amorphous in
nature
R. Prakash, V. Gopikrishna, D.Kandaswamy, GUTTA-PERCHA
– AN UNTOLD STORY, ENDODONTOLOGY, 17 (2), 33-6
54.
54
Gutta-percha conesconsist of approximately 20% guttapercha, 65% zinc oxide, 10%
radiopacifiers, and 5% plasticizers.
Attempts have been made to make gutta-percha more antimicrobial by the addition of
materials such as iodoform, calcium hydroxide, chlorhexidene, and tetracycline.
The clinical effectiveness of adding these materials has not been demonstrated. Moreover,
to exert an antimicrobial pharmacological effect, the active ingredient must leach out of
the gutta-percha, which could have a detrimental effect on longterm sealability.
55.
55
Active substancebeing ZnO from which zinc ions (Zn2+) are mobilized by hydrolysis.
No micro-organism capable of destroying trans 1,4- poly isoprene has been described till date .
Nocardia was the only organism capable of degrading gutta percha (Warneke et al 2007)
PROPERTIES OF GUTTA PERCHA
BACTERIAL DEGRADATION
BIOLOGICAL PROPERTIES
No systemic toxic reactions toward gutta-percha have been reported in the literature.
Several cell culture studies have demonstrated gutta-percha to have little or no cytotoxicity.
56.
56
Supplied by themanufacturer in a non-sterile form.
Storage in commonly used disinfectants should be avoided.
Gutta-percha cones should be stored in cool and dark conditions in order to prevent hardening and brittleness due to
further crystallization and/or oxidation.
Owing to its comparatively soft consistency, guttapercha can be removed mechanically by conventional hand file or by
rotary instruments.
Recently, gutta-percha cones that are “free of living germs” (declaration of the manufacturer) have been marketed.
HANDLING PROPERTIES
57.
57
1. It adaptsto the canal walls because of its compactability. In fact, gutta-percha is neither
molecularly condensable nor compressible. However, once softened by heat, it can be
compacted against the canal walls and collapse any voids present in the commercial product.
2. Once set, gutta-percha is stable in size. It shrinks only when chemically softened (e.g., with
chloroform) following evaporation of the solvent, or if it is physically softened (e.g., by heat),
during the cooling phase. For
these reasons, chemical softening of gutta-percha is to be avoided, since it may create voids.
Softening by physical means must be accompanied by compaction of the material to
compensate for the volumetric changes that occur during the cooling phase.
ADVANTAGES of gutta-percha points
58.
58
3. Although constitutedprimarily of zinc oxide, gutta-percha has a very low solubility rate.
Nonetheless, there
are some cases where gutta-percha, that had inadvertently been forced beyond the apex, was
partially resorbed over the course of several years.
4. It is well tolerated by tissues. Of all materials used in dentistry, gutta-percha is perhaps the
most inert.
5. It may have certain (weak) bacteriostatic activity, attributed to zinc oxide.
6. It is semi-solid when introduced in the canal. This allows easy manipulability. It becomes
malleable if
heated, so that it may assume any shape when compacted with appropriate instruments. This
allows a
59.
59
7. It isradiopaque because of its sulfate content (usually barium sulfate) and thus easily
recognizable
radiographically.
8. It can be easily disinfected. Immersion in 5%–6% sodium hypochlorite for 60 seconds is
sufficient to eliminate
both gram-positive and gram-negative microorganisms and even the most resistant Bacillus
subtilis spores.
9. If necessary, it can be easily removed from the root canal when endodontic retreatment is
indicated. Solvents such as chloroform, chlorothene, eucalyptus, and rectified white turpentine
have been used.
60.
60
10. Gutta-percha isa poor heat conductor. This implies optimal control of its plasticity in its most apical
portion,
when heated.
11. Once introduced into the root canal and heated, gutta-percha expands. This characteristic helps to
ensure a tighter seal.
Disadvantges of gutta-percha points are
1. Lack of sufficient rigidity especially in small sizes; it cannot always be pushed beyond a ledge that might be
present.
2. It adheres to the dentin walls without establishing any bonds. To rectify this shortcoming, one must always
use
a sealer.
3. Gutta-percha points should be stored in a cool location with low humidity, otherwise they become brittle
with time.
61.
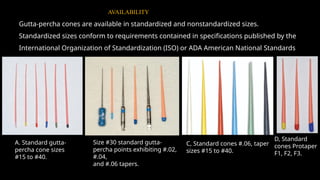
Gutta-percha cones areavailable in standardized and nonstandardized sizes.
Standardized sizes conform to requirements contained in specifications published by the
International Organization of Standardization (ISO) or ADA American National Standards
Institute (ADA ANSI).
A. Standard gutta-
percha cone sizes
#15 to #40.
C, Standard cones #.06, taper
sizes #15 to #40.
D, Standard
cones Protaper
F1, F2, F3.
AVAILABILITY
Size #30 standard gutta-
percha points exhibiting #.02,
#.04,
and #.06 tapers.
62.
62
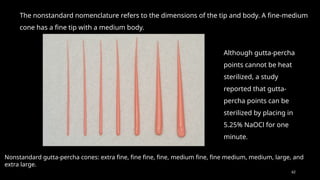
The nonstandard nomenclaturerefers to the dimensions of the tip and body. A fine-medium
cone has a fine tip with a medium body.
Nonstandard gutta-percha cones: extra fine, fine fine, fine, medium fine, fine medium, medium, large, and
extra large.
Although gutta-percha
points cannot be heat
sterilized, a study
reported that gutta-
percha points can be
sterilized by placing in
5.25% NaOCl for one
minute.
63.
63
TECHNIQUES FOR ROOTCANAL OBTURATION WITH GUTTA-
PERCHA
1. WARM VERTICAL COMPACTION
2. CONTINUOUS WAVE COMPACTION
3. THERMOMECHANICAL COMPACTION
4. COLD LATERAL COMPACTION
5. WARM LATERAL COMPACTION
6. THERMOPLASTIZIED INJECTION
7. CARRIER BASED GP
8. CHEMICAL SOFTENING
9. CUSTOM CONE
10. ACTIV GP
11. RESILON SYSTEM
64.
64
Ledge formation
Perforation
Unusual canalcurvatures
Internal resorptions
Large lateral canals
VERTICAL COMPACTION OF WARM GUTTA-PERCHA (Schilder
in 1967)
Indications (Weine)
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
65.
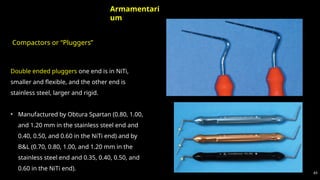
Compactors or “Pluggers”
65
Armamentari
um
Doubleended pluggers one end is in NiTi,
smaller and flexible, and the other end is
stainless steel, larger and rigid.
• Manufactured by Obtura Spartan (0.80, 1.00,
and 1.20 mm in the stainless steel end and
0.40, 0.50, and 0.60 in the NiTi end) and by
B&L (0.70, 0.80, 1.00, and 1.20 mm in the
stainless steel end and 0.35, 0.40, 0.50, and
0.60 in the NiTi end).
66.
66
The “Touch ‘nHeat” carrier (SybronEndo). The “Alpha 2” heat carrier (B&L). The Elements Obturation Unit
(SybronEndo)
The Calamus (Dentsply/Tulsa Dental).
Heat carrier
67.
67
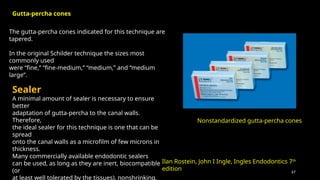
The gutta-percha conesindicated for this technique are
tapered.
In the original Schilder technique the sizes most
commonly used
were “fine,” “fine-medium,” “medium,” and “medium
large”.
Nonstandardized gutta-percha cones
Sealer
A minimal amount of sealer is necessary to ensure
better
adaptation of gutta-percha to the canal walls.
Therefore,
the ideal sealer for this technique is one that can be
spread
onto the canal walls as a microfilm of few microns in
thickness.
Many commercially available endodontic sealers
can be used, as long as they are inert, biocompatible
(or
at least well tolerated by the tissues), nonshrinking,
Gutta-percha cones
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
68.
68
Phases of obturation
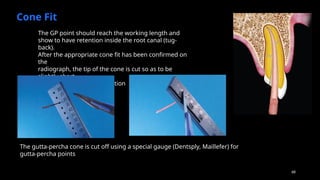
ConeFit
If feathered gutta-percha cones are used, they must be
slightly shortened (Figure 22-38) up to the size of the
apical
foramen, and a radiograph taken to check the cone fit.
The gutta-percha point should reach the working
length
The GP point should reach the working length and
show to have retention inside the root canal (tug-
back).
After the appropriate cone fit has been confirmed on
the
radiograph, the tip of the cone is cut so as to be
slightly short
with respect to the preparation
The gutta-percha cone is cut off using a special gauge (Dentsply, Maillefer) for
gutta-percha points
69.
69
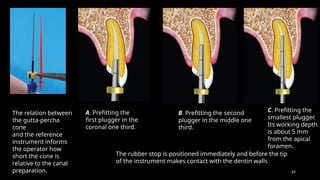
The relation between
thegutta-percha
cone
and the reference
instrument informs
the operator how
short the cone is
relative to the canal
preparation.
A. Prefitting the
first plugger in the
coronal one third.
The rubber stop is positioned immediately and before the tip
of the instrument makes contact with the dentin walls
B. Prefitting the second
plugger in the middle one
third.
C. Prefitting the
smallest plugger.
Its working depth
is about 5 mm
from the apical
foramen.
70.
70
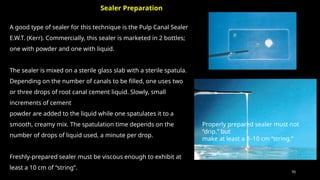
A good typeof sealer for this technique is the Pulp Canal Sealer
E.W.T. (Kerr). Commercially, this sealer is marketed in 2 bottles;
one with powder and one with liquid.
The sealer is mixed on a sterile glass slab with a sterile spatula.
Depending on the number of canals to be filled, one uses two
or three drops of root canal cement liquid. Slowly, small
increments of cement
powder are added to the liquid while one spatulates it to a
smooth, creamy mix. The spatulation time depends on the
number of drops of liquid used, a minute per drop.
Freshly-prepared sealer must be viscous enough to exhibit at
least a 10 cm of “string”.
Properly prepared sealer must not
“drip,” but
make at least a 8–10 cm “string.”
Sealer Preparation
71.
71
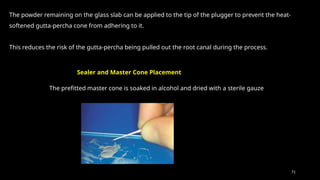
The powder remainingon the glass slab can be applied to the tip of the plugger to prevent the heat-
softened gutta-percha cone from adhering to it.
This reduces the risk of the gutta-percha being pulled out the root canal during the process.
Sealer and Master Cone Placement
The prefitted master cone is soaked in alcohol and dried with a sterile gauze
72.
72
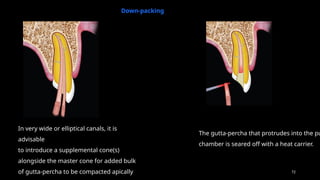
Down-packing
In very wideor elliptical canals, it is
advisable
to introduce a supplemental cone(s)
alongside the master cone for added bulk
of gutta-percha to be compacted apically
The gutta-percha that protrudes into the pu
chamber is seared off with a heat carrier.
73.
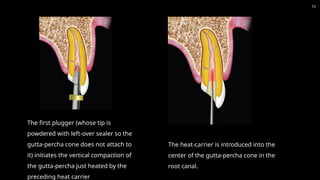
The first plugger(whose tip is
powdered with left-over sealer so the
gutta-percha cone does not attach to
it) initiates the vertical compaction of
the gutta-percha just heated by the
preceding heat carrier
The heat-carrier is introduced into the
center of the gutta-percha cone in the
root canal.
73
74.
74
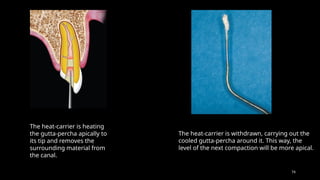
The heat-carrier isheating
the gutta-percha apically to
its tip and removes the
surrounding material from
the canal.
The heat-carrier is withdrawn, carrying out the
cooled gutta-percha around it. This way, the
level of the next compaction will be more apical.
75.
75
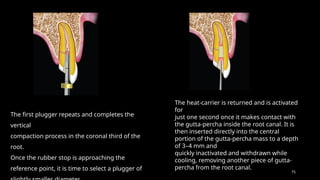
The first pluggerrepeats and completes the
vertical
compaction process in the coronal third of the
root.
Once the rubber stop is approaching the
reference point, it is time to select a plugger of
The heat-carrier is returned and is activated
for
just one second once it makes contact with
the gutta-percha inside the root canal. It is
then inserted directly into the central
portion of the gutta-percha mass to a depth
of 3–4 mm and
quickly inactivated and withdrawn while
cooling, removing another piece of gutta-
percha from the root canal.
76.
76
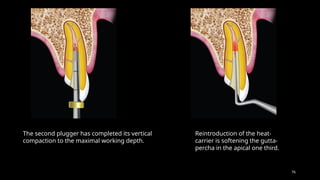
The second pluggerhas completed its vertical
compaction to the maximal working depth.
Reintroduction of the heat-
carrier is softening the gutta-
percha in the apical one third.
77.
77
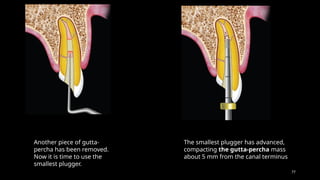
Another piece ofgutta-
percha has been removed.
Now it is time to use the
smallest plugger.
The smallest plugger has advanced,
compacting the gutta-percha mass
about 5 mm from the canal terminus
78.
78
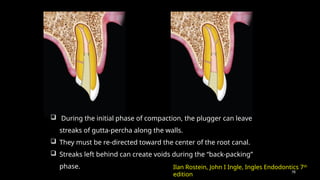
During theinitial phase of compaction, the plugger can leave
streaks of gutta-percha along the walls.
They must be re-directed toward the center of the root canal.
Streaks left behind can create voids during the “back-packing”
phase. Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
79.
79
Once thegutta-percha has been compacted to about 5–6 mm from the terminus of
the preparation, a radiograph is taken to verify that the gutta-percha is seated at the
desired location and that the obturation is well compacted.
The remainder of the canal (middle and coronal thirds) is filled in a backwards
fashion. It can be achieved via two different methods:
1. Introducing small pieces of gutta-percha into the root canal, and rhythmically
heating and compacting and them.
2. Using thermoplastic gutta-percha.
Reverse Filling (“back-packing”)
80.
80
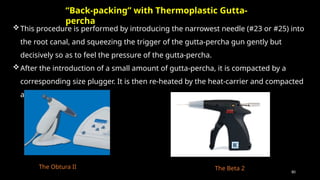
This procedure isperformed by introducing the narrowest needle (#23 or #25) into
the root canal, and squeezing the trigger of the gutta-percha gun gently but
decisively so as to feel the pressure of the gutta-percha.
After the introduction of a small amount of gutta-percha, it is compacted by a
corresponding size plugger. It is then re-heated by the heat-carrier and compacted
again.
“Back-packing” with Thermoplastic Gutta-
percha
The Obtura II The Beta 2
81.
81
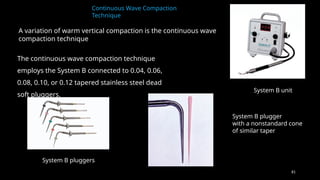
Continuous Wave Compaction
Technique
Avariation of warm vertical compaction is the continuous wave
compaction technique
System B unit
System B plugger
with a nonstandard cone
of similar taper
System B pluggers
The continuous wave compaction technique
employs the System B connected to 0.04, 0.06,
0.08, 0.10, or 0.12 tapered stainless steel dead
soft pluggers.
82.
82
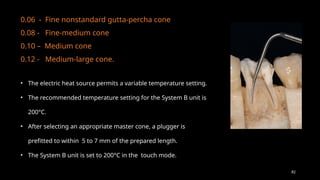
0.06 - Finenonstandard gutta-percha cone
0.08 - Fine-medium cone
0.10 – Medium cone
0.12 - Medium-large cone.
• The electric heat source permits a variable temperature setting.
• The recommended temperature setting for the System B unit is
200°C.
• After selecting an appropriate master cone, a plugger is
prefitted to within 5 to 7 mm of the prepared length.
• The System B unit is set to 200°C in the touch mode.
83.
83
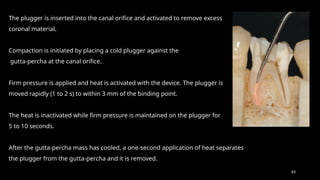
The plugger isinserted into the canal orifice and activated to remove excess
coronal material.
Compaction is initiated by placing a cold plugger against the
gutta-percha at the canal orifice.
Firm pressure is applied and heat is activated with the device. The plugger is
moved rapidly (1 to 2 s) to within 3 mm of the binding point.
The heat is inactivated while firm pressure is maintained on the plugger for
5 to 10 seconds.
After the gutta-percha mass has cooled, a one-second application of heat separates
the plugger from the gutta-percha and it is removed.
84.
84
In ovoidcanals, where the canal configuration may prevent the generation of
hydraulic forces, an accessory cone can be placed alongside the master cone
before compaction.
Filling the space left by the plugger may be accomplished by a thermoplastic
injection technique (Obtura or Ultrafil 3D [Coltène/Whaledent], Calamus
[DENTSPLY Tulsa Dental Specialties], Elements [SybronEndo], or HotShot
[Discus Dental, Los Angeles, California]).
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways
of the pulp, 11th edition
85.
85
This technique wasfirst introduced by McSpadden about 40 years ago. In this
technique a new instrument was used to condense the gutta-percha—the McSpadden
compactor.
The compactor, mounted on a contra-angled handpiece, was inserted in the canal next
to a gutta-percha cone and rotated at up to 20,000 rpm. Heat generated by friction
softened the gutta-percha and the blades pushed the material apically. This allowed the
THERMOMECHANICAL COMPACTION
86.
86
Using thestep-back method, the canal should be enlarged to at least the size of
a No. 45 instrument.
Gutta-percha cones are inserted in the prepared canal short of the root apex,
and a compactor blade, selected according to the width and length of the
prepared canal, is inserted between the gutta-percha and the canal wall.
With a stop on the compactor blade, the rotating tip of the blade is guided to
within 1.5 mm of the root apex.
Restriction of the blade within the canal prevents the forcing of
thermoplasticized gutta-percha through the root apex.
The plastic gutta-percha moves laterally and apically because the reversed flutes
on the compactor blade push the softened gutta-percha forward and sideways
even when one is withdrawing the rotating blade from the canal.
87.
87
Later, McSpaddendeveloped a new technique,
combining the principle of the thermomechanical
compaction with new materials.
The previous compactor was replaced with Nickel
Titanium Condensers, of different diameters and tapers,
and with “alpha phase” gutta-percha. This gutta-percha
was preplasticized in a MicroSeal heater and then
introduced into the canal with a rotating instrument, at
lower speeds (1,000 rpm to 4,000 rpm) than the original
McSpadden Compactor. This system uses MicroSeal
gutta-percha master cones and a specially formulated
Alpha Phase gutta-percha (low-fusing or ultra-low-
Kenneth M. Hargreaves, Louis H. Berman,
Cohen’s Pathways of the pulp, 11th edition
88.
88
• Lower pointof fusion of the gutta-percha
• Longer working time
• Less shrinkage during cooling
• High fluidity of the gutta-percha allowing for a good adaptation of the
material to the canal complexities.
The NiTi condenser is coated with heated gutta-percha and inserted into the canal next
to the master cone. The rotating instrument generates heat from the friction that, in
turn, thermally softens the master cone.
It also flows laterally, by centrifugal force, into all areas of the canal. The material is
therefore pushed both apically and laterally, providing a three-dimensional obturation of
the root canal system.
The most important characteristics of this
technique
91
LATERAL CONDENSATION OFGUTTA-PERCHA
Schematic illustration of the prepared root canal Fitting of the master cone. The cone is binding only
in the
apical portion of the prepared root canal.
92.
92
Spreader fit within2 mm of
the prepared canal without
binding. Note the space
available adjacent to the
spreader
The spreader is
introduced
alongside the
master cone to the
proper apical
depth.
After careful removal of the
spreader, an accessory cone,
lightly coated with sealer, is
introduced to the apical depth
created by the spreader.
93.
93
The spreader isreinserted
to make room for an
additional accessory cone.
The obturation process is continued until there is
no more room for additional insertions of the
spreader or further condensation of accessory
cones. At this point, the obturation is completed
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
94.
94
The auxiliarycones are selected based on the size of the spreader, the size of the canal, and
the position of the space created inside the canal. Prior to their insertion, the auxiliary cones
are lightly coated with sealer and are introduced to the same depth that the spreader has last
reached.
When the spreader can only penetrate 2 or 3 mm into the canal orifice, the obtutation is
completed.
The pressure exerted during lateral condensation should be very light because gutta-percha
is not compressible, and since as little as 1.5 kg of pressure is capable of fracturing the root.
Finally, the excess of gutta-percha protruding in the pulp chamber is seared off with a heat
carrier and is vertically compacted with prefitted pluggers.
The pulp chamber is cleaned with cotton pellets soaked in alcohol to remove any residual
particles of gutta-percha or sealer.
95.
95
A variationis lateral condensation with ultrasonic activation of the spreader.
With this technique the spreader is placed next to the master cone and activated without a water
coolant. Apical pressure is exerted, and the spreader is inserted to a predetermined length.
Advantages are that the ultrasonic action may spread the sealer, the friction of the spreader may
thermoplasticize the gutta-percha, and the force required to place the spreader may be less.
Ultrasonic Condensation
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION):
Walton & Torabinejad
96.
96
Occasionally, voidsor length problems will be apparent on the radiograph taken during or after obturation.
These should be corrected, before the sealer sets.
For voids, gutta-percha is removed with hot pluggers until the spreader can be reinserted just beyond the void
or discrepancy.
Then, a fresh mix of sealer is prepared. Lateral condensation is performed as described previously; sealer is
added back to the canal by coating each accessory cone.
An advantage of making an obturation verification radiograph before the excess gutta-percha is seared off is
that the entire mass can usually be removed by grasping the cones with the fingers.
Fitting a new master cone and re obturation is then possible.
Correcting Obturation Problems
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION):
Walton & Torabinejad
97.
97
If theexcess gutta-percha has been seared off, an overfill can sometimes be corrected before the sealer sets
by removing all gutta-percha with files or broaches.
When extruded beyond the apex, the overfilled gutta-percha is difficult to recover through the canal,
particularly after the sealer sets.
Extruded sealer can only be retrieved surgically.
Obturating materials extruded beyond the apex are irritants and affect healing, but generally they do not
completely prevent resolution unless there is gross overfill of core material.
ZnOE-based sealers often resorb from periapical tissues over time.
These situations should not be treated surgically unless failure to heal is evident on recall examination.
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION):
Walton & Torabinejad
98.
98
Lateral condensationis relatively uncomplicated, requires a simple armamentarium, and seals and
obturates as well as any other technique in conventional Situations.
Major advantage it has over most other techniques is length control.
With an apical stop and with careful use of the spreader, the length of the gutta-percha filling is
managed well.
Additional advantages include ease of retreatment, adaptation to the canal walls, positive dimensional
stability, and the ability to prepare post space.
Advantages
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION):
Walton & Torabinejad
99.
99
1. Being a“cold” technique, the gutta-percha cones don’t form a homogeneous, compact mass.
The final filling will comprise of a number of gutta-percha cones separated by a greater or
lesser amount of sealer, depending
on the clinician’s proficiency with the technique.
2. Filling of lateral portals of exit occurs less frequently than when vertical compaction is
performed and is always constituted of sealer, not gutta-percha.
3. The spreader should be placed within 1 mm to 2 mm of the working length. If not carefully
done, it may exert excessive lateral forces, increasing the risk of root fracture.
4. When considering that heat is not used, the most apical portion of the master cone does not
undergo significant modification. The seal in this area is, therefore, mainly entrusted to the
sealer.
DRAWBACKS
PRINCIPLES AND PRACTICE OF ENDODONTICS (3RD
EDITION):
Walton & Torabinejad
100.
100
This techniquewas introduced by Martin in 1987. It uses a special spreader whose tip is
electrically heated transmitting heat to the gutta-percha while laterally condensing.
While the lateral condensation technique is based on pressure that only causes a stratification of
the gutta-percha cones, the Endotec system permits the coalescense and fusion of the various
cones into a dense, homogeneous mass of guttapercha, with less stress on the dentinal walls.
This is a significantly simpler technique to execute.
TECHNIQUE OF WARM LATERAL CONDENSATION: THE
ENDOTEC
101.
101
Recently, anew device has been developed for both warm lateral and vertical
condensation, the EndoTwinn (MDCL N.V. Corporation, Amsterdam, The Netherlands).
This device combines application of heat and vibration.
Like the Endotec, the EndoTwinn is a hand-held, self-contained, heat-carrying
instrument with spreader or plugger tips.
Sonic vibrations are also incorporated to augment the compaction and obturation
effectiveness of EndoTwinn’s heated tips.
THE ENDOTWINN
Ilan Rostein, John I Ingle, Ingles Endodontics 7th
edition
102.
102
• In early2007, efforts to improve and refine the EndoTwinn led to the introduction of the
DownPak (Hu-Friedy, Chicago, Illinois).
• The DownPak system enables the clinician to employ variable temperature settings and to turn
the vibration feature on or off.
• The variable temperature settings are useful when different obturation materials are used. The
DownPak is cordless and light weight, with an ergonomically balanced hand-held grasp; all of
the switches and adjustments are easily accessible on the handle.
The EndoTwinn
system
103.
103
Thermoplastic Injection Techniques(Yee et al., Torabinejad et al.,
Marlin et al.,)
Heating of gutta-percha outside the tooth and injecting the material into the canal is an additional
variation of the thermoplastic technique.
The Obtura III, Calamus, Elements, HotShot, and
Ultrafil 3D
Available Devices
The Obtura system heats the gutta-percha to 160°C, whereas the Ultrafil 3D system employs a
low-temperature gutta-percha that is heated to 90 degree C.
104.
104
The Obtura IIIsystem (Obtura Spartan) consists of a hand-held
“gun” that contains a chamber surrounded by a heating element
into which pellets of gutta-percha are loaded. Silver needles
(varying gauges of 20, 23, and 25) are attached to deliver the
thermoplasticized material to the canal. The control unit allows
the operator to adjust the temperature and thus the viscosity of
the gutta-percha. The apical terminus should be as small as
possible to prevent extrusion of gutta-percha. The technique
requires the use of sealer, and once the canal is dried, the canal
walls are coated with sealer. Gutta-percha is preheated in the
gun, and the needle is positioned in the canal so that it reaches
within 3 to 5 mm of the apical preparation. Gutta-percha is then
gradually, passively injected by squeezing the trigger of the
“gun.”
Obtura III
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways
of the pulp, 11th edition
105.
105
The needle backsout of the canal as the apical portion is filled. Pluggers dipped in alcohol are
used to compact the gutta-percha. A segmental technique may also be used, in which 3- to 4-
mm segments of gutta-percha are sequentially injected and compacted.
o The difficulties with this system include lack of length control. Both overextension and
underextension are common results.
o To overcome this drawback, a hybrid technique may be used, in which the clinician
begins filling the canal by the lateral compaction technique.
o When the master cone and several accessory cones have been placed so that the mass
is firmly lodged in the apical portion of the canal, a hot plugger is introduced, searing
the points off approximately 4 to 5 mm from the apex.
o Light vertical compaction is applied to restore the integrity of the apical plug of gutta-
percha. The remainder of the canal is then filled with thermoplasticized gutta-percha
injected.
106.
106
Ultrafil 3D (Coltène/Whaledent)is a thermoplastic gutta-percha
injection technique involving gutta-percha cannulas, a heating
unit, and an injection syringe.
The system employs three types of gutta-percha cannulas. The
Regular Set is a low-viscosity material that requires 30 minutes to
set.
The Firm Set is also a low-viscosity material but differs in that it
sets in 4 minutes.
Endoset has a higher viscosity and does not flow as well. It is
recommended for techniques employing compaction and sets in
2 minutes. The heater is preset at 90°C and does not require
adjustment.
Ultrafil 3D
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways
of the pulp, 11th edition
107.
107
The Calamus flowobturation delivery system
(DENTSPLY
Tulsa Dental Specialties) is a thermoplastic device
equipped
with a cartridge system with 20- and 23-gauge
needles. The unit permits control of temperature and
also the flow rate. Pluggers are also available for use
with the system.
Calamus
108.
108
Obturation unit (SybronEndo)consists of a System B heat
source and plugger as well as a handpiece extruder for
delivering thermoplastic gutta-percha or RealSeal from a
disposable cartridge. The cartridges come with 20-, 23-, and
25-gauge needles for gutta-percha and 20- and 23-gauges
for RealSeal.
Elements
HotShot
The HotShot delivery system (Discus Dental [now part of
Philips Oral Healthcare]) is a cordless thermoplastic device
that has a heating range from 150°C to 230°C.
The unit is cordless and can be used with either gutta-percha
or Resilon. Needles are available in 20, 23, and 25 gauges.
109.
109
Thermafil, ProfileGT Obturators, GT Series X Obturators, and ProTaper Universal Obturators
Thermafil (DENTSPLY Tulsa Dental Specialties) was introduced as a gutta-percha obturation
material with a solid core.
Originally manufactured with a metal core and a coating of gutta-percha, the carrier was
heated over an open flame.
The technique was popular because the central core provided a rigid mechanism to
facilitate the placement of the gutta-percha.
Advantages included ease of placement and the pliable properties of the gutta-percha.
Disadvantages were metallic core made placement of a post challenging and retreatment
procedures were difficult.
Carrier-Based Gutta-Percha
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways
of the pulp, 11th edition
111
Changes inthe carrier systems include the development of a plastic core coated with α-phase
gutta-percha and a heating device that controls the temperature.
The Thermafil oven with carrier in
place
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the
pulp, 11th edition
112.
112
Removal ofthe smear layer is strongly recommended and has been shown to enhance the seal
with Thermafil.
After drying the canal a light coat of sealer is applied and a carrier is marked, set to the
predetermined length.
This is accomplished by using the millimeter calibration markings on the carrier shaft. Markings
are made at 18, 19, 20, 22, 24, 27, and 29 mm.
Gutta-percha on the shaft that may be obscuring the calibration rings can be removed with a
surgical blade or knife.
The carrier is disinfected with 5.25% NaOCl for 1 minute and rinsed in 70% alcohol.
The carrier is then placed in the heating device.
When the carrier is heated to the appropriate temperature the clinician has approximately 10
seconds to retrieve it and insert it into the canal
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways
of the pulp, 11th edition
113.
113
This isaccomplished without rotation or twisting.
The position of the carrier is verified radiographically.
The gutta-percha is allowed 2 to 4 minutes to cool before resecting the coronal portion
of the carrier, which can be several millimeters above the canal orifice.
This is accomplished by applying stabilizing pressure to the carrier and cutting the
device with an inverted cone, round bur, or a specially designed Prepi bur (DENTSPLY
Tulsa Dental Specialties).
Heated instruments are not recommended for this process because this may result in
displacement
114.
114
o Vertical compactionof the coronal gutta-percha can then be accomplished. When
necessary, gutta-percha can be added, heat softened, and compacted.
o An advantage to this technique is the potential for movement of gutta-percha into lateral
and accessory canals; however, extrusion of material beyond the apical extent of the
preparation is a disadvantage
o Pro-Post drills (DENTSPLY Tulsa Dental Specialties) are recommended if post space is
required for restoration of the tooth.
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways
of the pulp, 11th edition
115.
115
This techniquewas described by Callahan and Johnston at the beginning of the last century. It
used chloroform to chemically soften gutta-percha.
The technique is still practiced today with various types of chloroform sealers.
Guttapercha particles are added to chloroform to produce a sealer (chloropercha), that has the
same color as gutta-percha.
The mixture can then be used as a sealer with gutta-percha cones for obturation of the canal.
There is more shrinkage with the chloroform solvent techniques and this often translates into
leakage, with the material pulling away from the canal walls as it shrinks thereby creating voids.
CHEMICAL SOFTENING OF GUTTA-PERCHA
116.
116
1. Whenthe chloroform evaporates, the material undergoes a significant shrinkage,
compromising the longterm apical seal.
If the root canal is filled with chloropercha alone, two thirds of the material will be lost
once evaporation of the chloroform has occurred.
The operator must be very careful to avoid overfilling, because of the reported tissue
toxicity of chloroform
DRAWBACKS
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways
of the pulp, 11th edition
117.
117
When theapical foramen is excessively large or the
prepared root canal system is large, a custom cone may
need to be fabricated. This permits the adaptation of the
cone to the canal walls, reduces the potential for
extrusion of the corematerial, and may improve the
resultant seal.
The technique involves selection of a master cone and
fitting that cone 2 to 4 mm short of the prepared length
with frictional resistance.
Custom Cones
118.
118
The coneis grasped with locking cotton pliers or a hemostat so that it
can be placed into the canal in the same spatial relationship each time.
The cone is removed and the tip is softened in chloroform, eucalyptol,
or halothane for 1 or 2 seconds, depending on the clinical
requirements. Only the outer superficial portion of the cone is
softened. The central core of the cone should remain semi-rigid.
The cone is then placed into the canal to the working length. The
process can be repeated until an adequate impression of the canal is
obtained at the prepared length.
119.
119
A radiographis exposed to verify proper fit and position. An alternative to solvents
is softening with heat.
Large root canal systems may necessitate custom fabrication of a large master
cone before canal adaptation.
This may be accomplished by heating two, or more, large gutta-percha cones and
rolling the mass between two glass slabs until an appropriate size is obtained. A
spatula may also be used to shape the cone.
The posttreatment
radiograph with post space
prepared
A 1-year follow-up
radiograph demonstrating
osseous regeneration.
120.
120
Activ GP(Brasseler USA) consists of gutta-
percha cones impregnated on the external
surface with glass ionomer.
Single cones are used with a glass ionomer
sealer. Available in 0.04 and 0.06 taper
cones, the sizes are laser verified to help
ensure a more precise fit.
The single cone technique is designed to
provide a bond between the dentinal canal
wall and the master cone.
Activ GP
R. M. E. Tomson, N. Polycarpou and P. L. Tomson Contemporary obturation of the root canal system,
BRITISH DENTAL JOURNAL VOLUME 216 NO. 6 MAR 21 2014
121.
121
Epiphany system withthe primer, thinning
resin, sealant, and standard Resilon points.
The resin-based obturation systems RealSeal
(SybronEndo), and Resinate (Obtura Spartan,
Algonquin, Illinois) have been introduced as
alternatives to gutta-percha. Resilon is a high-
performance industrial polyester that has been
adapted for dental use.
The resin sealer bonds to a Resilon core, and
attaches to the etched root surface.
The manufacturer claims that this forms a
“monoblock”. With traditional obturation
techniques, there is a gutta-percha–sealer interface
and a toothsealer interface.
With Resilon the resin sealer bonds to both the
Resilon
122.
122
The systemresembles gutta-percha and can be placed by
lateral compaction, warm lateral or vertical compaction,
thermoplastic injection, or with a core-carrier technique.
It consists of a resin core material (Resilon) composed of
polyester, difunctional methacrylate resin, bioactive glass,
radiopaque fillers, and a resin sealer.
Because NaOCl may affect the bond strength of the primer,
EDTA should be the last irrigant used before rinsing the canal
with sterile water, saline, or chlorhexidine.
Resilon #.02, #.04, and
#.06 tapered points and a
thermoplastic plug for
use in the Obtura system.
R. M. E. Tomson, N. Polycarpou and P. L. Tomson Contemporary obturation of the root
canal system, BRITISH DENTAL JOURNAL VOLUME 216 NO. 6 MAR 21 2014
123.
123
After dryingthe canal, a self-etch primer (sulfonic acid– terminated functional monomer,
2-hydroxyethyl methacrylate [HEMA], water, and polymerization initiator) is used to
condition the canal walls and prepare them for bonding to the resin sealant (resin matrix
of bisphenol A-glycidyl methacrylate [Bis-GMA], ethoxylated Bis-GMA, urethane
dimethacrylate [UDMA], and hydrophilic difunctional methacrylates and fillers [70%] of
calcium hydroxide, barium sulfate, barium glass, bismuth oxychloride, and silica).
Two or three drops are placed in the canal with a pipette, a syringe, or a paper point that
wicks the material to the working length.
R. M. E. Tomson, N. Polycarpou and P. L. Tomson Contemporary obturation of the root
canal system, BRITISH DENTAL JOURNAL VOLUME 216 NO. 6 MAR 21 2014
124.
124
The excessprimer is removed, the resin sealer is dispensed onto a mixing slab, and the
viscosity is adjusted with the thinning resin.
The sealer is applied with a paper point, Resilon point, or lentulo spiral.
The canal is then obturated by lateral compaction, warm vertical compaction, or
thermoplastic injection.
The sealer takes approximately 25 minutes to set, so it is recommended that the coronal
surface of the material be light cured for 40 seconds.
R. M. E. Tomson, N. Polycarpou and P. L. Tomson Contemporary obturation of the root
canal system, BRITISH DENTAL JOURNAL VOLUME 216 NO. 6 MAR 21 2014


![30
Methacrylate Resin Sealers
Four generations of methacrylate resin–based root canal sealers have been marketed for
commercial use
First generation:
The first generation of hydrophilic methacrylate resin–based material (Hydron; Hydron
Technologies, Inc., Boca Raton, Florida) was designed for en masse root filling and
appeared in the mid 1970s.
The major component of Hydron was poly[2-hydroxyethyl methacrylate] (poly[HEMA]),
which was injected into a root canal and polymerized in situ within the canal space
without the adjunctive use of a root-filling material.
Hydron became obsolete in the 1980s as subsequent clinical findings were unacceptable.
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways of the pulp, 11th
edition](https://image.slidesharecdn.com/obturationall-250421005926-2fee84f8/85/obturation-all-important-for-dental-students-30-320.jpg)


![84
In ovoid canals, where the canal configuration may prevent the generation of
hydraulic forces, an accessory cone can be placed alongside the master cone
before compaction.
Filling the space left by the plugger may be accomplished by a thermoplastic
injection technique (Obtura or Ultrafil 3D [Coltène/Whaledent], Calamus
[DENTSPLY Tulsa Dental Specialties], Elements [SybronEndo], or HotShot
[Discus Dental, Los Angeles, California]).
Kenneth M. Hargreaves, Louis H. Berman, Cohen’s Pathways
of the pulp, 11th edition](https://image.slidesharecdn.com/obturationall-250421005926-2fee84f8/85/obturation-all-important-for-dental-students-84-320.jpg)
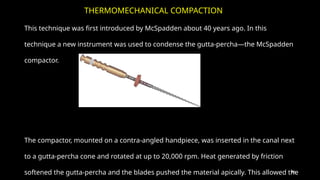
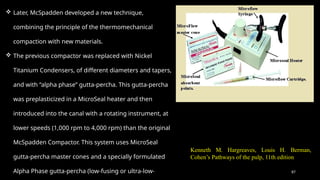
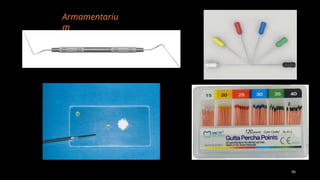
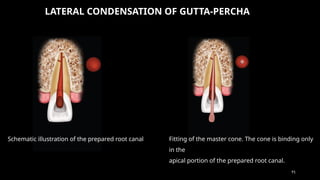
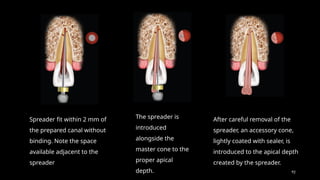

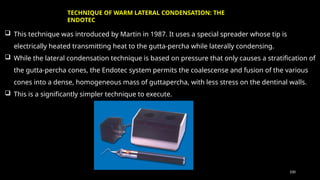
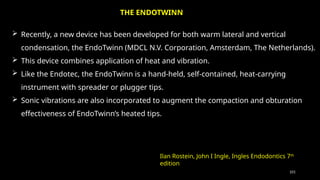
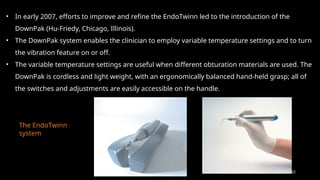
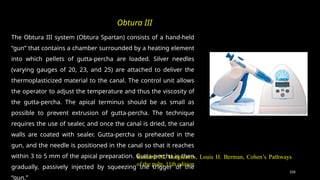
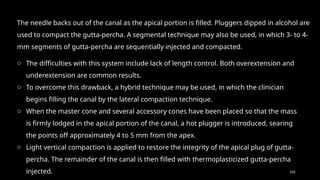
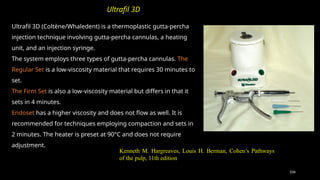
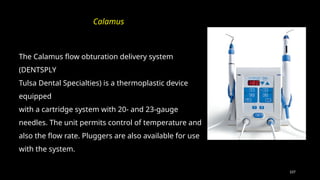
![108
Obturation unit (SybronEndo) consists of a System B heat
source and plugger as well as a handpiece extruder for
delivering thermoplastic gutta-percha or RealSeal from a
disposable cartridge. The cartridges come with 20-, 23-, and
25-gauge needles for gutta-percha and 20- and 23-gauges
for RealSeal.
Elements
HotShot
The HotShot delivery system (Discus Dental [now part of
Philips Oral Healthcare]) is a cordless thermoplastic device
that has a heating range from 150°C to 230°C.
The unit is cordless and can be used with either gutta-percha
or Resilon. Needles are available in 20, 23, and 25 gauges.](https://image.slidesharecdn.com/obturationall-250421005926-2fee84f8/85/obturation-all-important-for-dental-students-108-320.jpg)

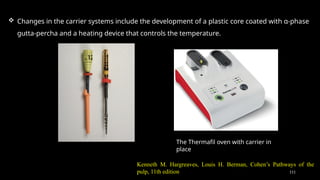
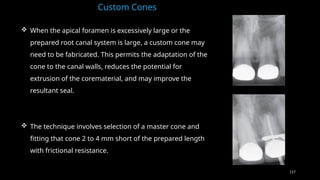
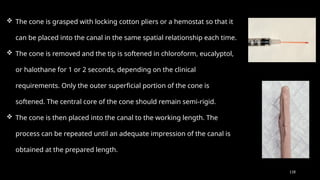
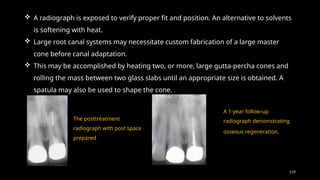
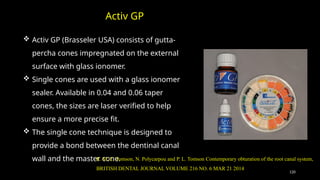
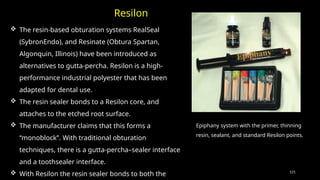
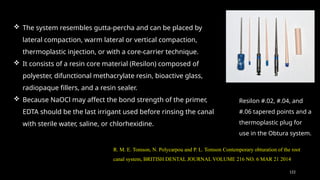
![123
After drying the canal, a self-etch primer (sulfonic acid– terminated functional monomer,
2-hydroxyethyl methacrylate [HEMA], water, and polymerization initiator) is used to
condition the canal walls and prepare them for bonding to the resin sealant (resin matrix
of bisphenol A-glycidyl methacrylate [Bis-GMA], ethoxylated Bis-GMA, urethane
dimethacrylate [UDMA], and hydrophilic difunctional methacrylates and fillers [70%] of
calcium hydroxide, barium sulfate, barium glass, bismuth oxychloride, and silica).
Two or three drops are placed in the canal with a pipette, a syringe, or a paper point that
wicks the material to the working length.
R. M. E. Tomson, N. Polycarpou and P. L. Tomson Contemporary obturation of the root
canal system, BRITISH DENTAL JOURNAL VOLUME 216 NO. 6 MAR 21 2014](https://image.slidesharecdn.com/obturationall-250421005926-2fee84f8/85/obturation-all-important-for-dental-students-123-320.jpg)


















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










