O R I G I N A L P A P E R
Characteristics of Patients Referred to Psychiatric Emergency
Services by Crisis Intervention Team Police Officers
Beth Broussard • Joanne A. McGriff •
Berivan N. Demir Neubert • Barbara D’Orio •
Michael T. Compton
Received: 29 September 2009 / Accepted: 20 January 2010 / Published online: 7 February 2010
� Springer Science+Business Media, LLC 2010
Abstract The Crisis Intervention Team (CIT) program
trains police officers in crisis intervention skills and local
psychiatric resources. Because the safety and appropriate-
ness of any new intervention is a crucial consideration, it is
necessary to ensure that CIT training does not result in
excessive or inappropriate referrals to psychiatric emer-
gency services (PES). Yet, aside from one prior report by
Strauss et al. (2005) in Louisville, Kentucky, little is known
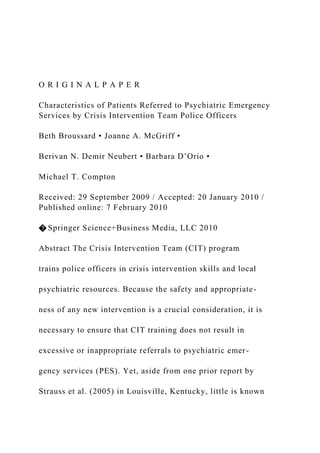
about the comparability of patients referred to PES by CIT-
trained officers in relation to other modes of referral. The
research questions driving this retrospective chart review
of patients referred to PES were: (1) What types of patients
do CIT-trained officers refer to PES?, and (2) Do mean-
ingful differences exist between patients referred by family
members, non-CIT officers, and CIT-trained officers?
Select sociodemographic and clinical variables were
abstracted from the medical records of 300 patients during
an eight-month period and compared by mode of referral.
Differences across the three groups were found regarding:
race, whether or not the patient was held on the locked
observation unit, severe agitation, recent substance abuse,
global functioning, and unkempt or bizarre appearance.
However, there were virtually no differences between
patients referred by CIT-trained and non-CIT officers.
Thus, while there were some expected differences between
patients referred by law enforcement and those referred by
family members, CIT-trained officers appear to refer
individuals appropriately to PES, as evidenced by such
patients differing little from those referred by traditional,
non-CIT police officers. Trained officers do not have a
narrower view of people in need of emergency services
(i.e., bringing in more severely ill individuals), and they do
not have a broader view (i.e., bringing in those not in need
of emergency services). Although CIT training does not
appear to affect the type of individuals referred to PES,
future research should examine the effect of CIT training
on the frequency of referrals or proportion of subjects
encountered that are referred, which may be expected to
differ between CIT-trained and non-CIT officers.
Keywords Crisis intervention team � Law enforcement �
Police officers � Psychiatric emergency services
Introduction
As first responders in crisis situations involving persons
with serious mental illnesses, law enforcement officers are
often the principal source of referral to psychiatric emer-
gency services (PES) and play an .
O R I G I N A L P A P E RCharacteristics of Patients Refer.docx
1. O R I G I N A L P A P E R
Characteristics of Patients Referred to Psychiatric Emergency
Services by Crisis Intervention Team Police Officers
Beth Broussard • Joanne A. McGriff •
Berivan N. Demir Neubert • Barbara D’Orio •
Michael T. Compton
Received: 29 September 2009 / Accepted: 20 January 2010 /
Published online: 7 February 2010
� Springer Science+Business Media, LLC 2010
Abstract The Crisis Intervention Team (CIT) program
trains police officers in crisis intervention skills and local
psychiatric resources. Because the safety and appropriate-
ness of any new intervention is a crucial consideration, it is
necessary to ensure that CIT training does not result in
excessive or inappropriate referrals to psychiatric emer-
gency services (PES). Yet, aside from one prior report by
Strauss et al. (2005) in Louisville, Kentucky, little is known
2. about the comparability of patients referred to PES by CIT-
trained officers in relation to other modes of referral. The
research questions driving this retrospective chart review
of patients referred to PES were: (1) What types of patients
do CIT-trained officers refer to PES?, and (2) Do mean-
ingful differences exist between patients referred by family
members, non-CIT officers, and CIT-trained officers?
Select sociodemographic and clinical variables were
abstracted from the medical records of 300 patients during
an eight-month period and compared by mode of referral.
Differences across the three groups were found regarding:
race, whether or not the patient was held on the locked
observation unit, severe agitation, recent substance abuse,
global functioning, and unkempt or bizarre appearance.
However, there were virtually no differences between
patients referred by CIT-trained and non-CIT officers.
Thus, while there were some expected differences between
patients referred by law enforcement and those referred by
3. family members, CIT-trained officers appear to refer
individuals appropriately to PES, as evidenced by such
patients differing little from those referred by traditional,
non-CIT police officers. Trained officers do not have a
narrower view of people in need of emergency services
(i.e., bringing in more severely ill individuals), and they do
not have a broader view (i.e., bringing in those not in need
of emergency services). Although CIT training does not
appear to affect the type of individuals referred to PES,
future research should examine the effect of CIT training
on the frequency of referrals or proportion of subjects
encountered that are referred, which may be expected to
differ between CIT-trained and non-CIT officers.
Keywords Crisis intervention team � Law enforcement �
Police officers � Psychiatric emergency services
Introduction
As first responders in crisis situations involving persons
with serious mental illnesses, law enforcement officers are
often the principal source of referral to psychiatric emer-
4. gency services (PES) and play an important role in the
initiation of mental health treatment. Violent behavior,
male gender, experiencing more severe psychosocial
stressors, and spending more time in the emergency setting
have been found to characterize those patients referred by
law enforcement officers to PES compared to other modes
of referral, such as referral by health care providers, self-
referral, and other referral sources (Redondo and Currier
B. Broussard � J. A. McGriff � B. D’Orio � M. T. Compton
(&)
Department of Psychiatry and Behavioral Sciences, Emory
University School of Medicine, 49 Jesse Hill Jr. Drive, S.E.,
Room #333, Atlanta, GA 30303, USA
e-mail: [email protected]; [email protected]
M. T. Compton
Department of Behavioral Sciences and Health Education,
Rollins School of Public Health of Emory University,
Atlanta, GA, USA
B. N. Demir Neubert
5. Department of Health Policy and Management, Rollins School
of Public Health of Emory University, Atlanta, GA, USA
123
Community Ment Health J (2010) 46:579–584
DOI 10.1007/s10597-010-9295-3
2003; Way et al. 1993). Furthermore, race/ethnicity and its
socioeconomic correlates may play a role in pathways to
care, as exemplified by research indicating high rates of
police involvement and police referral to psychiatric ser-
vices for ethnic minorities with psychotic disorders (Bhu-
gra et al. 2000; Burnett et al. 1999; Commander et al. 1999;
Compton et al. 2006a, Fisher et al. 2004; Garety and Rigg
2001; Jarvis et al. 2005; Morgan et al. 2004, 2005a, b). In
recognition of the role that police officers often assume in
psychiatric referral and mental health crisis situations, as
well as the widespread problem of criminalization of
people with mental illnesses, many law enforcement
6. agencies have implemented crisis intervention programs in
collaboration with community partners.
The Crisis Intervention Team (CIT) program trains
officers in crisis intervention skills to adequately handle
interactions with individuals with mental illnesses or
substance use disorders. Furthermore, in addition to the
training, the program was developed in an effort to pro-
mote partnerships among law enforcement, mental health
professionals, and advocates. The training component of
CIT provides police officers with 40 h of lectures and
role-playing activities based on the Memphis Model of
CIT (Bower and Pettit 2001; Dupont and Cochran 2000).
As described in detail elsewhere (Oliva and Compton
2008), implementation of CIT trainings in Georgia began
in 2005 and is supported by a multi-disciplinary collabo-
ration among numerous organizations (e.g., Georgia
Bureau of Investigation, Georgia Department of Behav-
ioral Health and Developmental Disabilities, Georgia
7. affiliate of the National Alliance on Mental Illness). The
Georgia CIT training curriculum is approved by Georgia
Peace Officer Standards and Training to assure quality and
consistency of training in localities throughout the state.
The week-long course is comprised of: (1) approximately
20 h of lectures on psychiatric disorders and related topics
(e.g., signs and symptoms of mental illnesses, schizo-
phrenia, suicide prevention, addictive disorders, cultural
sensitivity, mental health laws) delivered by local mental
health professionals, advocates, and attorneys; (2) roughly
6 h visiting local emergency facilities and inpatient psy-
chiatric units, in part to hear the experiences of patients;
and (3) about 10 h of performance-based de-escalation
training that relies partly on role playing. Each class
accommodates 15–25 officers.
Most evaluation studies of CIT have focused on officer-
level data. For instance, research has examined improve-
ments in officers’ knowledge of and attitude towards
8. specific mental illnesses, officers’ enhanced self-efficacy,
officers’ decreased desire for social distance, increased
referrals to psychiatric services, reductions in the use of
force, and reductions in officer injuries (Bahora et al. 2008;
Borum et al. 1998; Compton et al. 2006b, 2010; Dupont
and Cochran 2000). However, additional outcomes
research on CIT is seriously needed (Compton et al. 2008).
While positive findings at the officer level are beneficial
and encouraging, research must begin to examine the effect
of CIT at the consumer level to determine whether CIT is
accomplishing its overall goal of facilitating mental health
referral for individuals with mental illnesses—in lieu of
incarceration—when appropriate. One example is the work
of Strauss et al. (2005), who utilized a chart review design
involving 485 patients referred to the emergency psychi-
atric services in Louisville, Kentucky, to examine charac-
teristics of patients brought in by CIT-trained officers
compared to those brought in by other sources (mental
9. inquest warrant or self-referral). Data collected from charts
included demographics, disposition, and diagnosis (pre-
sumably categorized generally into schizophrenia-related
disorders, mood disorders, or other diagnoses). CIT-trained
officers were found to refer individuals appropriately; those
referred by CIT-trained officers were not significantly
different from those referred by other sources, except in
diagnosis. A higher proportion of people brought in by
CIT-trained officers had a diagnosis of schizophrenia
(Strauss et al. 2005).
The current study attempted to replicate these previous
findings by conducting an exploratory, retrospective chart
review that assessed the sociodemographic and clinical
characteristics of patients referred to PES of a large, urban,
public-sector, county hospital in the southeastern United
States. Patients were classified by mode of referral; having
been referred by family members, traditional non-CIT
officers, or CIT-trained officers. The two research ques-
10. tions driving this study were: (1) What types of patients are
CIT-trained officers referring to PES? and (2) Do mean-
ingful differences exist between patients referred by family
members, patients referred by non-CIT officers, and
patients referred by CIT-trained officers? Because the
safety of any new intervention designed to improve health
is an initial research priority (‘‘first, do no harm’’), it is
necessary to ensure that CIT training does not result in
excessive or inappropriate referrals to PES. Do trained
officers have a narrower view of people in need of emer-
gency services, bringing in only severely ill individuals; do
they have a broader view, bringing in those not in need of
emergency services; or do they make appropriate referrals,
as indexed by such individuals being comparable with
those referred through other means? This study did not
attempt to address whether or not CIT-trained officers
bring in more patients (i.e., a greater frequency of referrals)
or a greater proportion of individuals with whom they
11. interact. Those issues, which should be addressed in other
research, could not be examined through a retrospective
chart review design because the number of individual
officers’ referrals would need to be counted and the number
580 Community Ment Health J (2010) 46:579–584
123
of CIT-trained and non-CIT officers would need to be
known, or a denominator (the total number of interactions
the individual officers have) would be necessary.
Methods
For the chart review, 300 patients were identified by
reviewing medical records of individuals referred to PES
during the May 2008–December 2008 period. This repre-
sented a sample of charts, rather than a review of each and
every consecutive medical record. Inclusion criteria were
that patients were 18 years or older at the time of PES
evaluation, and that patients were referred to PES by
12. family members, non-CIT officers, or CIT-trained officers.
In an effort to include a diverse representation of patients
seen in PES, charts were reviewed from PES regardless of
the patients’ hospital course or final disposition (i.e., dis-
charge from PES versus admission to the inpatient psy-
chiatric unit or crisis stabilization unit). Patients from these
two units are referred from PES, and their PES charts
become part of their inpatient medical record.
Select sociodemographic, referral-related, and clinical
variables were abstracted from the medical records in a
standardized way. These variables included: age, gender,
race, diagnosis (schizophrenia or a related primary psy-
chotic disorder versus a primary affective disorder versus
another primary diagnosis), whether or not the patient was
held in the locked observation unit after triage, presence of
suicidal ideation, presence of homicidal ideation, severe
disorganization, severe agitation, recent substance abuse,
the Global Assessment of Functioning (GAF) scale score
13. (Endicott et al. 1976), and whether or not the patient was
discharged from PES (versus referral for hospitalization).
Only three broad diagnostic categories, rather than specific
diagnoses, were used due to limited sample sizes of
patients with individual diagnoses. In this PES setting,
diagnoses are made and recorded in the medical record by
the evaluating physician, based on the Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition
(American Psychiatric Association 2000a). Symptoms and
risks (e.g., presence of suicidal ideation) are assessed by a
nurse or social worker, and then reviewed by the evaluating
physician. Forms in the medical record allow these clini-
cians to tick boxes to record the presence of symptoms.
The GAF scale score is a widely used, reliable, and valid
100-point range that indicates overall current symptoms
and psychosocial functioning (American Psychiatric
Association 2000a, b; Goldman et al. 1992). The scale is
divided into 10 intervals with anchoring descriptions for
14. each (American Psychiatric Association 2000a). In addi-
tion to these variables, 10 mental status exam items were
assessed: appearance (e.g., neat versus unkempt or bizarre),
behavior, interaction, cooperativeness, speech, thought
content, affect, hallucinations, judgment, and insight.
The selection of variables was dependent on, and limited
by, information written in the medical record during rou-
tine clinical interactions in PES. Abstracted variables were
entered directly into a database in a password-protected
laptop computer. For the purpose of data collection,
patients were assigned a unique study number. No identi-
fying information was collected. The study protocol was
approved by the university’s institutional review board and
the hospital’s research oversight committee. The authors
have no known conflicts of interest pertaining to this study,
and all authors certify responsibility for the results and this
publication.
Data analysis was conducted using the SPSS version
15. 16.0 statistical software package. Basic descriptive statis-
tics depicted the overall sample in terms of sociodemo-
graphic and clinical variables. Bivariate analyses, including
chi-square tests of independence and analyses of variance,
were used to compare the three subgroups (patients refer-
red by family members, those brought in by non-CIT
officers, and patients referred by CIT-trained officers)
along these sociodemographic and clinical variables. To be
conservative, data imputation techniques were not
employed for missing data points.
Results
Between May 2008 and December 2008, 300 charts were
reviewed. Two hundred thirteen charts (71.0%) were in
PES, 11 (3.7%) were in the inpatient psychiatric unit, and 8
(2.7%) were in the crisis stabilization unit. Chart reviews in
the latter two settings involved the PES portion of the chart
rather than the inpatient record. As shown in Table 1, 127
patients (42.3%) were brought in by family members, 132
16. (44.0%) were brought in by non-CIT officers, and 41
Table 1 Sociodemographic characteristics of the 300 patients
Age, years (mean ± standard deviation) 38.4 ± 13.6
Gender
Female 128 (42.7%)
Male 172 (57.3%)
Race (n = 286)
African American 234 (81.8%)
European American 44 (15.4%)
Hispanic/Latino 8 (2.8%)
Mode of referral
Family 127 (42.3%)
Non-CIT Police Officers 132 (44.0%)
CIT-Trained Officers 41 (13.7%)
Community Ment Health J (2010) 46:579–584 581
123
(13.7%) were brought in by CIT-trained officers. The mean
17. age of patients was 38.4 ± 13.6 years (range = 18–78)
and 128 patients (42.7%) were female. The majority of the
sample (234, 81.8%) was African American.
As shown in Table 2, when associations between mode
of referral and the sociodemographic and clinical variables
of patients were examined, five variables were significantly
associated with mode of referral: (1) race (v2 = 7.90,
df = 2, P = 0.02), (2) whether or not the patient was held
on the locked observation unit (v2 = 146.10, df = 2, P
0.001), (3) severe agitation (v2 = 7.60, df = 2, P = 0.02),
(4) substance abuse (v2 = 15.42, df = 2, P .001), and
(5) GAF scale score (F = 3.68, df = 2, 260, P = 0.03).
Several post-hoc chi-square tests were conducted to clarify
where, among the three modes of referral, significant dif-
ferences occurred when it was not clear by examining the
proportions. With regard to race, an additional chi-square
test indicated that the proportions of African American
patients did not differ between non-CIT and CIT referrals
(P = 0.23), but that the proportions of African American
patients did differ by family members versus non-CIT
18. officer referrals (P = 0.006). For substance abuse, an
additional chi-square test similarly revealed that the pro-
portions with substance abuse did not differ between
non-CIT and CIT referrals (P = 0.10). In terms of GAF
scores, Tukey’s HSD post-hoc tests revealed that patients
brought in by family members had a higher GAF score
(40.7 ± 13.0) than those brought in by CIT-trained officers
(34.2 ± 10.6). Again, there was no difference between
patients brought in by non-CIT versus CIT-trained officers.
Regarding the mental status examination characteristics
of patients (data not shown), the proportion of patients with
unkempt or bizarre appearance noted on the mental status
examination differed significantly across the three modes
of referral. Specifically, both non-CIT and CIT-trained
officers brought in a higher percentage of patients with an
unkempt or bizarre appearance (63, 51.2% and 22, 61.1%)
compared to family members (28, 23.03%; v2 = 27.86,
df = 2, P 0.001). No other mental status examination
items differed across the three groups.
19. Discussion
Findings of the current study were remarkably similar to
those of the report by Strauss et al. (2005) in terms of
sample characteristics. For example, approximately 42% of
both samples were female (42.7% in the current study and
Table 2 Sociodemographic and clinical variables by mode of
referral
Variable (number included in the test
of association, if 300)
Family members
(n = 127)
Non-CIT officers
(n = 132)
CIT-Trained officers
(n = 41)
Test statistic, df, P
Age 38.5 ± 14.7 39.0 ± 12.9 36.1 ± 12.4 NS
Gender, male 70 (55.1%) 78 (59.1%) 24 (58.5%) NS
Race, African American (n = 286) 107 (88.4%) 95 (74.8%) 32
(84.2%) v2 = 7.90, df = 2,
P = 0.02
a
20. Diagnosis of schizophrenia or a related primary
psychotic disorder (n = 289)
76 (61.8%) 73 (57.9%) 29 (72.5%) NS
Diagnosis of a primary affective disorder (n = 289) 31 (25.2%)
23 (18.3%) 6 (15.0%) NS
Held on the locked observation unit (n = 274) 17 (16.2%) 115
(89.1%) 36 (90.0%) v2 = 146.10, df = 2,
P 0.001
Presenting problem noted on the triage form:
Suicidal ideation (n = 274) 14 (11.8%) 21 (17.5%) 8 (22.9%)
NS
Homicidal ideation (n = 269) 2 (1.7%) 8 (7.0%) 3 (8.6%) NS
Severe disorganization (n = 266) 24 (21.1%) 33 (28.0%) 10
(29.4%) NS
Severe agitation (n = 268) 12 (10.3%) 28 (23.9%) 7 (20.0%) v2
= 7.60, df = 2,
P = 0.02
Substance abuse (n = 251) 24 (22.6%) 52 (48.1%) 12 (32.4%)
v2 = 15.42, df = 2,
P .001a
GAF scale score (n = 263) 40.7 ± 13.0 38.8 ± 12.5 34.2 ± 10.6 F
= 3.68, df = 2, 260,
P = 0.03
b
21. Discharged from PES (n = 274) 28 (52.8%) 35 (50.7%) 16
(64.0%) NS
df degrees of freedom; NS non-significant; GAF Global
Assessment of Functioning
a
Post-hoc chi-square tests revealed a statistically significant
difference in race and substance abuse between patients brought
in by family
members and those brought in by non-CIT officers (but no
difference between those brought in by non-CIT vs. CIT-trained
officers)
b
Post-hoc tests revealed a statistically significant difference in
mean GAF scale scores between patients brought in by family
members and those
brought in by CIT-trained officers
582 Community Ment Health J (2010) 46:579–584
123
41.3% in the Strauss et al. sample) and roughly 15% of the
two samples were referred by CIT-trained officers (13.7%
in this study and 16.3% in the Strauss et al. study). In
addition, the mean age of participants in the current study
22. (38.4 years) was very similar to that of the Strauss et al.
sample (37.4 years). Thus, in many respects, such as
sample characteristics, the present study serves as a well-
matched replication of the Strauss et al. report.
Differences in characteristics of patients by mode of
referral were found in several domains: race, whether or not
they were held on the locked observation unit, severe agi-
tation, substance abuse, GAF score, and unkempt or bizarre
appearance. A number of explanations seem plausible.
First, non-CIT officers in this setting appear to be referring a
lesser proportion of African American patients than are
family members. The study was conducted in an urban,
public-sector hospital where approximately 90% of patients
are African American. Because this hospital serves as an
emergency receiving facility for all police officers to bring
in people from the city and surrounding areas (which
are characterized by a higher proportion of European
Americans, as well as lower saturation of the CIT training
23. program compared to the inner-city), the non-CIT police-
referred group had a lesser percentage of African Ameri-
cans. Second, the prominent difference in proportions of
patients that were located on the locked observation unit is
driven by hospital policy in this setting. That is, all patients
brought in by police officers on a peace officer’s report (a
temporary commitment that can be completed by officers)
are immediately taken to this locked unit. Third, the results
indicated that patients referred by law enforcement officers
(both CIT-trained and non-CIT) were more agitated, more
likely to have a history of abusing substances, and more
likely to be unkempt or bizarre in appearance than those
referred by family members. These findings may be con-
sistent with previous reports indicating that officer
involvement often occurs with potentially dangerous or
violent individuals (Redondo and Currier 2003). Fourth,
and related, patients referred by family members had sig-
nificantly higher GAF scores compared to those referred by
24. CIT-trained and non-CIT officers, indicating that family
members bring in patients with a milder severity of illness
and dysfunction than those brought in by officers. No sig-
nificant differences were found between patients brought in
by CIT-trained and non-CIT officers. The current findings
differ from those of Strauss et al. (2005) in that no differ-
ence was found across groups in terms of diagnosis.
Several methodological limitations should be considered
in the interpretation of the present findings. First, multiple
nurses and social workers conducted the initial assessment
in PES, and there are no measures of their inter-rater
reliability in the recording of data in patients’ charts. Thus,
discrepancies between ratings of symptoms and risks could
have been introduced, though there is no reason to believe
that this would have been a systematic bias. Second,
because of the retrospective design, missing data points
were relatively common, though more in some variables
than other. Only available data were used; to be conser-
25. vative, techniques for the imputation of data were not
employed. Third, some charts were missing the mode of
referral, excluding them from review which could have
biased the results. However, it is not expected that missing
referral modes would be concentrated in one referral type.
Results from this retrospective chart review reveal that
patients brought in by CIT-trained officers are similar to
those brought in by non-CIT officers. Furthermore, patients
brought in by police officers generally resemble those
brought in by family members in many respects. Thus,
CIT-trained officers are referring individuals appropriately
to emergency psychiatric services. Trained officers do not
have a more narrow view of people in need of emergency
services, bringing in more severely ill individuals; neither
do they have a broader view, bringing in those not in need
of emergency services. CIT training does not appear to
affect the type of individual referred to PES. Future
research should examine whether or not CIT-trained offi-
26. cers bring in more patients (i.e., a greater frequency of
referrals) or a greater proportion of individuals with whom
they interact, now that it has been established that CIT-
referred patients are appropriate referrals and differ little
from patients referred through other modes.
References
American Psychiatric Association. (2000a). Diagnostic and
statistical
manual of mental disorders, Fourth Edition, Text Revision.
Washington, DC: American Psychiatric Association.
American Psychiatric Association. (2000b). Handbook of
psychiatric
measures. Washington, DC: American Psychiatric Association.
Bahora, M., Hanafi, S., Chien, V. H., & Compton, M. T. (2008).
Preliminary evidence of effects of Crisis Intervention Team
training on self-efficacy and social distance. Administration and
Policy in Mental Health and Mental Health Services Research,
53, 159–167.
Bhugra, D., Hilwag, M., Mallett, R., Corridan, B., Leff, J.,
Neehall, J.,
et al. (2000). Factors in the onset of schizophrenia: A compar-
ison between London and Trinidad samples. Acta Psychiatrica
27. Scandinavica, 101, 135–141.
Borum, R., Deane, M., Steadman, H., & Morrissey, J. (1998).
Police
perspectives on responding to mentally ill people in crisis:
Perceptions of program effectiveness. Behavioral Sciences and
the Law, 16, 393–405.
Bower, D. L., & Pettit, W. G. (2001). The Albuquerque Police
Department’s Crisis Intervention Team: A report card. FBI Law
Enforcement Bulletin, 70, 1–6.
Burnett, R., Mallett, R., Bhugra, D., Hutchinson, G., Der, G., &
Leff,
J. (1999). The first contact of patients with schizophrenia with
psychiatric services: Social factors and pathways to care in a
multi-ethnic population. Psychological Medicine, 29, 475–483.
Community Ment Health J (2010) 46:579–584 583
123
Commander, M. J., Cochrane, R., Sashidharan, S. P., Akilu, F.,
&
Wildsmith, E. (1999). Mental health care for Asian, black and
white patients with non-affective psychoses: Pathways to the
28. psychiatric hospital, in-patient and after-care. Social Psychiatry
and Psychiatric Epidemiology, 34, 484–491.
Compton, M. T., Bahora, M., Watson, A. C., & Oliva, J. R.
(2008). A
comprehensive review of extant research on Crisis Intervention
Team (CIT) programs. Journal of the American Academy of
Psychiatry and the Law, 36, 47–55.
Compton, M. T., Demir-Neubert, B. N., Broussard, B., McGriff,
J. A.,
Morgan, R., & Oliva, J. R. (2010). Use of force preferences and
perceived effectiveness of actions among Crisis Intervention
Team (CIT) police officers and non-CIT officers in an
escalating
psychiatric crisis involving a subject with schizophrenia.
Schizophrenia Bulletin (in press).
Compton, M. T., Esterberg, M. L., Druss, B. G., Walker, E. F.,
&
Kaslow, N. J. (2006a). A descriptive study of pathways to care
among hospitalized urban African American first-episode
schizophrenia-spectrum patients. Social Psychiatry and Psychi-
atric Epidemiology, 41, 566–573.
Compton, M. T., Esterberg, M. L., McGee, R., Kotwicki, R. J.,
29. &
Oliva, J. R. (2006b). Crisis Intervention Team training: Changes
in knowledge, attitudes, and stigma related to schizophrenia.
Psychiatric Services, 57, 1199–1202.
Dupont, R., & Cochran, S. (2000). Police response to mental
health
emergencies—barriers to change. Journal of the American
Academy of Psychiatry and the Law, 28, 338–344.
Endicott, J., Spitzer, R. L., Fieiss, J. L., & Cohen, J. (1976).
The
global assessment scale: A procedure for measuring overall
severity of psychiatric disturbances. Archives of General
Psychiatry, 33, 766–771.
Fisher, H., Russell, M., Iacoponi, E., Craig, T., Garety, P.,
McGuire,
P., & Power, P. (2004). Pathways to care in first-episode
psychosis: A new measure of services contacted and received
before the commencement of treatment in first-episode
psychosis
(Abstract). Schizophrenia Research 70, Suppl, 77.
Garety, P. A., & Rigg, A. (2001). Early psychosis in the inner
city: A
30. survey to inform service planners. Social Psychiatry and
Psychiatric Epidemiology, 36, 537–544.
Goldman, H. H., Skodal, A. E., & Lave, T. R. (1992). Revising
axis V
for DSM-IV: A review of measures of social functioning.
American Journal of Psychiatry, 149, 1148–1156.
Jarvis, G. E., Kirmayer, L. J., Jarvis, G. K., & Whitley, R.
(2005). The
role of Afro-Canadian status in police or ambulance referral to
emergency psychiatric services. Psychiatric Services, 56, 705–
710.
Morgan, C., Mallett, R., Hutchinson, G., Bagalkote, H.,
Morgan, K.,
Fearon, P., et al. (2005a). Pathways to care and ethnicity. 1:
Sample characteristics and compulsory admission: Report from
the ÆSOP study. British Journal of Psychiatry, 186, 281–289.
Morgan, C., Mallett, R., Hutchinson, G., Bagalkote, H.,
Morgan, K.,
Fearon, P., et al. (2005b). Pathways to care and ethnicity. 2:
Source of referral and help-seeking: Report from the ÆSOP
study. British Journal of Psychiatry, 186, 290–296.
Morgan, C., Mallett, R., Hutchinson, G., & Leff, J. (2004).
Negative
31. pathways to psychiatric care and ethnicity: The bridge between
social science and psychiatry. Social Science and Medicine, 58,
739–752.
Oliva, J. R., & Compton, M. T. (2008). A statewide Crisis
Intervention Team (CIT) initiative: Evolution of the Georgia
CIT program. Journal of the American Academy of Psychiatry
and the Law, 36, 38–46.
Redondo, R. M., & Currier, G. W. (2003). Characteristics of
patients
referred by police to a psychiatric emergency service. Psychi-
atric Services, 54, 804–806.
Strauss, G., Glenn, M., Reddi, P., Afaq, I., Podolskaya, A., &
Rybakova, T. (2005). Psychiatric disposition of patients brought
in by Crisis Intervention Team police officers. Community
Mental Health Journal, 41, 223–228.
Way, B. B., Evans, M. E., & Banks, S. M. (1993). An analysis
of
police referrals to 10 psychiatric emergency rooms. Bulletin of
the American Academy of Psychiatry and the Law, 21, 380–397.
584 Community Ment Health J (2010) 46:579–584
123
32. Reproduced with permission of the copyright owner. Further
reproduction prohibited without permission.
c.10597_2010_Article_9295.pdfCharacteristics of Patients
Referred to Psychiatric Emergency Services by Crisis
Intervention Team Police
OfficersAbstractIntroductionMethodsResultsDiscussionReferenc
es
Coldiron et al. Conflict and Health 2013, 7:23
http://www.conflictandhealth.com/content/7/1/23
CASE STUDY Open Access
Brief mental health interventions in conflict and
emergency settings: an overview of four
Médecins Sans Frontières – France programs
Matthew E Coldiron1*, Augusto E Llosa1, Thomas Roederer1,
German Casas2,3 and Marie-Rose Moro2,4
Abstract
Introduction: Mental health problems, particularly anxiety and
mood disorders, are prevalent in the setting of
humanitarian emergencies, both natural and man-made disasters.
Evidence regarding best strategies for therapeutic
interventions is sparse. Médecins Sans Frontières has been
providing mental health services during emergencies for
over two decades, and here we compare data from four
programs.
Program Overview: In China, 564 patients were followed for an
average of 7 sessions after a major earthquake.
The most common diagnoses were PTSD and other anxiety
disorders. Between program entry and exit, the median
global assessment of functioning increased from 65 to 80. At
program entry, 58% were considered moderately,
33. markedly or severely ill; a proportion which fell to 14% at
program exit. In Colombia in the setting of chronic
violence, 2411 patients were followed for a median of two
sessions. Anxiety disorders and major depression were
the most common diagnoses, and 76% of patients were
moderately or severely ill at program entry. 91% had
symptomatic improvement at program exit. In Gaza, 1357
patients were followed for a median of 9 sessions; a
majority was under age 15. PTSD and other anxiety disorders
were the most common diagnoses, and 91% were
moderately or severely ill at entry. 89% had improved
symptoms at program exit. In the West Bank, the 1478
patients had similar characteristics to those enrolled in Gaza.
88% were moderately or severely ill at entry; 88% had
improved at exit.
Discussion and evaluation: It was feasible to implement brief
yet effective mental health interventions in a wide
variety of humanitarian contexts – post-natural disaster, during
acute violent conflict and during chronic violent
conflict. The most common diagnoses were PTSD, other anxiety
disorders and mood disorders. The use of local
specially-trained counselors who were focused on coping skills
and improving functionality over a brief time period,
likely contributed to the symptomatic improvement seen in a
large majority of patients across the four sites.
Conclusions: Mental health is an essential part of a health care
response to humanitarian emergencies. In a variety
of settings, we show the positive results of brief interventions.
Further research is needed to improve and evaluate
mental health interventions in crises.
Keywords: Disasters, Therapeutic consultations, PTSD,
Refugees, War, Violence, Natural disasters, Disaster medicine
* Correspondence: [email protected]
35. opinions [9-11]. Better evidence about the role of mental
health care in humanitarian settings is needed [12]. How-
ever, carrying out clinical research in these settings can be
challenging, partially because of weakened health systems
and structures. Likewise, specific, targeted interventions
may not be appropriate in all cultures and regions.
Since 1989, MSF France has provided psychological
care to persons affected by violence and lacking medical
support [13,14], implementing mental health care pro-
grams in response to emergencies in over 40 countries on
five continents worldwide. Principles of psychological first
aid are used. The psychotherapeutic work that is offered
through MSF programs is based on Winnicott’s thera-
peutic consultations model for children that we have
adapted for adults and for varied cultural contexts [15,16].
We encourage individuals (adults, or where appropriate,
children) and families or dyads (mothers with their chil-
dren) to externalize their emotions and fears, to share
their traumas, depression and anxiety, and to cope with
their stresses [16]. We take into account different social
and cultural contexts, using local therapists or translators
[17-19], and we are guided by principles of psychodynamic
and interpersonal psychotherapy [18,20]. While the details
of the intervention may change slightly depending on the
context, the overall psychotherapeutic technique remains
the same. Patients with complex mental health problems
Table 1 Patient characteristics in four MSF mental health pro
China (N = 564) C
Sex*
F 388 (68.8%) 1
M 176 (31.2%) 7
36. Median age (IQR) 41 (14–58) 3
Median # of sessions (IQR) 7 (5–9) 2
Median length of therapy in weeks (IQR) 7 (5–10) 3
*Missing values for 7 patients in Colombia, 2 patients in Gaza,
and 2 patients in Nablu
and those not in the target population of the various
interventions are referred to existing local health
structures designed for longer-term psychological and
psychiatric care.
Given the paucity of published literature on the subject,
the cross-cultural aspect of MSF mental health program-
ming can provide important insights on responding to
emergencies. Here we describe patients enrolled in 4 men-
tal health programs in emergency contexts, their diagno-
ses and their clinical evolution. Some of the data have
been published individually [6,21,22]. In the context of this
synthesis, we aim to show the results of brief psychological
interventions in diverse emergency contexts, from areas
experiencing chronic and acute violence as well as major
natural disasters. Anonymized patient data were en-
tered into Epidata (Odense, Denmark) and analyzed
with STATA 10.1 (College Station, Texas, USA). The
program was authorized by local authorities and pa-
tients were informed about the use of data in research.
Privacy and confidentiality of patients were ensured
during the treatment and after the conduct of the analysis.
This analysis met the criteria for review of program
monitoring data and for exemption from the MSF Ethics
Review Board.
Program overview
37. Table 1 presents demographic data as well as information
about length of care for patients enrolled in programs in
all four sites described below.
China
On 12 May 2008, a strong earthquake (7.9 on Richter
scale) hit the Sichuan province of China, killing at least
100 000 people and leaving 5 million displaced. In the
first days after the earthquake, MSF established a stand-
ard response in support of local and national emergency
relief officials, including emergency mental health
services. From 12 November 2008 until 15 August 2009,
in conjunction with the Crisis Intervention Center of
the Chinese Academy of Sciences, MSF offered psycho-
logical care in Wudu and Beichuan, sites of temporary
housing for displaced persons, located approximately
100 km from the earthquake’s epicenter. Patients referred
grams
olombia (N = 2411) Gaza (N = 1357) Nablus (N = 1478)
624 (67.6%) 617 (45.5%) 868 (58.8%)
80 (32.4%) 738 (54.5%) 608 (41.2%)
3 (15–46) 13 (9–24) 15 (7–36)
(1–3) 9 (6–12) 7 (4–10)
(1–6) 12 (8–16) 12 (7–17)
s.
Coldiron et al. Conflict and Health 2013, 7:23 Page 3 of 6
38. http://www.conflictandhealth.com/content/7/1/23
from local health care providers, as well as those detected
in community screenings, were referred to psychological
care centers managed by MSF, the Chinese Academy of
Science and the Crisis Intervention Center in the tempor-
ary camps.
Ten local volunteer counselors provided psychological
consultations under the supervision of a single expatriate
clinical psychologist. The locally-trained volunteer coun-
selors also benefitted from additional crisis response train-
ing provided by MSF, as well as individual and team
meetings led by senior mental health staff and case review.
Brief psychological evaluations were made on self-referred
patients, as well as those who had been referred from
school and community workers and health care providers.
Patients diagnosed with a psychological condition for
which psychotherapy was considered beneficial were
enrolled in follow-up therapy.
Table 2 lists the most common primary diagnoses
among the 564 patients enrolled in follow-up programs.
A majority of patients were diagnosed with anxiety dis-
orders, including PTSD and generalized anxiety disorder.
Other common diagnoses included bereavement and ad-
justment disorder. Global assessment of functioning
(GAF) and CGI were recorded at each visit. At first con-
tact, median GAF was 65 (IQR 60–75) and 327 (58%) of
patients were described as moderately, markedly, or se-
verely ill on the CGI. At the time of last contact, median
GAF was 80 (IQR 75–85) and 78 (14%) patients were
described as moderately, markedly, or severely ill.
Colombia
Colombia has been affected by internal armed conflict
for the last 40 years. Since 2002, MSF has provided men-
39. tal health programming in the Department of Tolima,
long a center of activity for different armed groups. The
civilian population of this area has experienced multiple
displacements, kidnappings, extortion, and repeated acts
of armed violence. In this area, short-term psychological
care was provided at a fixed urban site and in mobile
clinics in rural areas where access to care was impeded
because of the conflict.
Table 2 Clinical diagnoses representing at least 5% of formal
China (N = 564) Colombia (n = 2323)
Condition Number (%) Condition Number (%)
PTSD 206 (36) Anxiety disorders† 750 (32)
Anxiety disorders† 146 (26) MDD 423 (18)
Bereavement 49 (9) ASD 230 (10)
Adjustment disorder 32 (6) Adjustment disorder 197 (9)
PTSD + MDD 27 (5) PTSD 196 (8)
MDD 26 (5)
*PTSD = Post-traumatic stress disorder; MDD = Major
depressive disorder; ASD = Acute s
†Excluding ASD and PTSD.
At first contact, screening for PTSD, anxiety disorder,
and depression was performed using a self-administered
checklist of signs, symptoms, and feelings. Severity of
symptoms was assessed for those admitted into follow-up
programs by considering the number and intensity of the
signs and symptoms of the disorder. Patients received ei-
ther individual or group psychotherapeutic interventions.
40. A full description of the methods used has been previously
published [21].
Here we summarize the outcomes of the 2411 patients
enrolled in individual or group psychotherapy between
February 2005 and February 2008. Overall, 2054 patients
(85.2%) received individual psychotherapy; the others re-
ceived either group or dyad therapy, such as mother-
and-child therapy for children under 3 years. Primary
diagnoses were available for 2323 of enrolled patients.
The most common clinical diagnoses were anxiety disor-
ders (excluding PTSD and acute stress disorder) and de-
pression. Acute stress disorder, adjustment disorder, and
PTSD were also frequently diagnosed (Table 2). At time of
enrollment, 1519 patients (64.2%) had moderate symp-
toms and 275 (11.6%) had severe symptoms. Patient de-
fault was common (1236, 51.7%). At the time of last
contact, information about improvement or aggravation of
symptom severity was available for 1685 patients (69.9%)
originally enrolled. Of those, 154 (9.1%) had unchanged or
worsened symptoms and 1531 (90.9%) had improved
symptoms.
Gaza
Densely-populated and impoverished, the Gaza Strip
has seen repeated waves of political tension and armed
conflict for much of the last decade. The use of rockets
and mortars has led to loss of property and deteriorat-
ing infrastructure, as well as many violent injuries and
deaths. Living in the midst of chronic conflict, with on-
going fears of exacerbation, its residents have experi-
enced large-scale trauma. MSF has provided medical
care in Gaza since 1989, and its mental health program
has aimed to provide support to civilian victims of con-
flict. Given concerns about the applicability of standard
diagnoses made in four MSF mental health programs*
41. Gaza (n = 1332) Nablus (N = 1478)
Condition Number (%) Condition Number (%)
PTSD 659 (50) Anxiety disorders† 333 (25)
Anxiety disorders† 247 (19) PTSD 226 (17)
MDD 175 (13) MDD 149 (11)
Enuresis 61 (5) ASD 147 (11)
Distress, no disorder 126 (9)
Enuresis 111 (8)
tress disorder.
Coldiron et al. Conflict and Health 2013, 7:23 Page 4 of 6
http://www.conflictandhealth.com/content/7/1/23
criteria and categories in this cross-cultural and post-
traumatic background, focus groups with local profes-
sionals were conducted at the beginning of the program in
Gaza and the West Bank to better understand the cultural
implications of presenting complaints and symptoms.
At first contact, semi-structured interviews with stan-
dardized questionnaires led to an eventual DSM-IV-TR
diagnosis, assigned by MSF psychologists and psychia-
trists. The severity of disorder (mild, moderate, severe)
was assessed at the initial visit and at the final visit. A
full description of the methods used has been previously
published [22].
42. Patients enrolled in Gaza were younger than those
treated in China and Colombia; over half were children
under 15 years. Among the 1357 patients whose mental
health care began in an MSF clinic between January 2007
and July 2011, a formal diagnosis was available for 1332
patients. A large majority of patients were diagnosed with
anxiety disorders; fully one-half were diagnosed with
PTSD (Table 2). Depression and enuresis were also com-
mon. Severity at first contact was judged as moderate in
754 patients (55.6%) and as severe in 474 (34.9%). In total,
only 133 patients (10.2%) defaulted on their treatment
program. An assessment of symptom severity at program
exit was available for 1256 patients: 141 (11.2%) had
unchanged or worsened symptoms and 1115 (88.8%)
had improved symptoms.
West Bank
The city of Nablus is one of the major urban centers of
the West Bank. This part of the Occupied Palestinian
Territories has also known political tension and violent
conflict over the past decade, but with a lower level of
acute violence than in Gaza. MSF has provided mental
health care in the West Bank since 1994, opening a
program in Nablus in 2004.
As in Gaza, referrals to the program were made from
local health care practitioners as well as through com-
munity outreach efforts. All referred patients were
screened and assigned a primary diagnosis. Those with
mental illness related to the political tension and vio-
lence were enrolled in follow-up with MSF; patients not
meeting these criteria were referred to appropriate
health care providers.
Here we describe results of 1478 patients enrolled in the
43. MSF mental health program between January 2007 and
December 2011. Just as in the Gaza program, over half of
all patients enrolled were children under 15. A formal
diagnosis was available for 1355 patients. Like in Gaza, a
variety of anxiety disorders and depression were the most
common diagnoses (Table 2). On the other hand, the diag-
nosis of PTSD was made less frequently than in Gaza. As
in Gaza, the diagnosis of enuresis was common, likely
reflecting the younger age of enrolled patients. Severity at
first contact was judged as moderate in 689 patients
(46.7%) and severe in 601 (40.7%). As in Gaza, patient de-
fault was low – 286 patients (21.0%). An assessment of
symptom severity at last contact was available for 1206 pa-
tients: 146 (10.8%) had unchanged or worsened symptoms
and 1060 (87.9%) had improved symptoms.
Discussion and evaluation
The strength of the current overview is that it shows a
straightforward model of care that has been adapted for
use in a wide variety of humanitarian settings – from
Latin America to the Middle East to China. Furthermore,
in these diverse settings – acute conflict, chronic conflict,
and post-natural disaster – the overall patient-level results
were extremely satisfactory, with marked improvement of
functionality and/or symptom intensity seen throughout.
On the most basic level, several lessons can be taken
away from this series of programs. Most importantly, it is
possible to provide high-quality mental health care in the
midst of humanitarian emergencies. While this is not ne-
cessarily a new observation, many previous reports of the
effectiveness of psychotherapeutic interventions have been
in the setting of clinical trials, under controlled settings,
and with a larger infrastructure. The data described here
are simply programmatic. On one hand, this is not ideal
for drawing conclusions, but on the other hand, given the
44. large number of patients across such different settings, the
strength of the results described here – under actual pro-
gram conditions – underscores the importance of includ-
ing this type of programming in a standard emergency
response.
The clinical improvement of patients provides several
learning points. First, we believe that our model of care
provision is well-adapted for responding to humanitarian
emergencies. Non-professionals undergo intense, short-
term training on providing coping skills and brief
counseling sessions. One benefit of this model is that the
counselors begin their training with a high level of lan-
guage skills, and often cultural competency, relevant to
the populations for whom they are caring. On the other
hand, the use of non-professionals as counselors creates a
burden for the supervising mental health professionals,
both in terms of diagnostic accuracy as well as therapeutic
follow-up. It also limits the number of clinical diagnoses
that are able to be cared for in one program. Nonetheless,
given that a large majority of our patients suffered from a
limited number of mood and anxiety disorders, the train-
ing of counselors is made easier.
The measures of outcomes described here are rudi-
mentary – often measured as “improved”, “unchanged”,
or “worsened”, and did not always correlate to quantitative
measures. At the same time, given the diversity of the so-
cial and political contexts, in the absence of standardized
transcultural evaluation methods, this sort of simple
Coldiron et al. Conflict and Health 2013, 7:23 Page 5 of 6
http://www.conflictandhealth.com/content/7/1/23
measurement is actually quite powerful. Using standard
45. checklists of symptoms, mental health professionals with a
variety of backgrounds and non-professional counselors
were able to make judgments about patient outcomes.
In these humanitarian emergencies, the first goal of our
mental health programs was to improve functionality
and symptoms. This high rate of symptom-based and
functional improvement was seen in all of the projects
described here.
Despite efforts, given the wide variety of contexts re-
ported here, it is clear that clinical diagnoses were not
completely standardized, thus limiting specific analysis
of outcome by clinical diagnosis. This would be interest-
ing to consider, particularly for post-traumatic stress
disorder and other anxiety disorders, which were the
most common diagnoses encountered. While our re-
sults showed good levels of clinical improvement, it
would also be interesting to see if rates of response dif-
fered by age. Given the variety of different therapeutic
interventions used (individual, dyad, and group therapy),
and without a more structured and consistent method
of assessment across contexts, we are hesitant to draw
conclusions.
Lastly, it would also be interesting to consider the
costs of these different interventions. Given the overall
rapid improvement of patients enrolled in our programs,
quantifying the financial needs for program implementa-
tion, which we imagine to be comparatively small, might
provide additional impetus for the inclusion of similar
programs in other humanitarian emergencies.
Conclusions
Standardization of data collection and evaluation methods
would allow for greater comparability across different
contexts. While patient care is rightfully prioritized in
46. humanitarian settings, standardized monitoring of men-
tal health diagnoses and outcomes would facilitate pro-
gram evaluation. Additional rigorous assessments are
still needed, but there appears to be an overall benefit to
appropriately-targeted psychotherapy in war and other
humanitarian crises [6,12,22,23].
The interventions we describe here were short-term.
Implementation of longer-term psychological follow-up,
particularly in areas affected by chronic violence, remains
challenging. In our programs, patients needing ongoing
psychiatric care were referred to local health care struc-
tures and other partner organizations. While beyond the
scope of this overview, and indeed beyond the scope of
MSF mental health interventions, it would be interesting
to further assess the psychological needs of this group of
patients.
Few conclusive studies assessing the effectiveness of
mental health interventions in crises have been conducted.
As a result, there is an ongoing gap in the current
evidence base on individual components of mental health
packages as well as best therapeutic strategies for specific
diagnoses in low resource settings. One such study
showed positive results in the treatment of PTSD in survi-
vors of sexual violence and could be used as a model for
research [24]. Additional examples of studies which could
be conducted in crises should include outcome assess-
ments as well as quasi-experimental designs where there
is a built-in comparator and cross-culturally validated as-
sessment tool. It is important to note that ethical concerns
and the need to provide treatment may preclude the use
of individual randomization.
Providing mental health care services should be part
of the standard response to humanitarian emergencies.
47. Our experience in vastly different settings shows that it is
both feasible and beneficial for the patients. Our model,
using a variety of mental health care providers – profes-
sionals and specially-trained local counselors – allowed us
to care for a large number of patients in difficult contexts.
Abbreviations
CGI: Clinical global impressions scale; GAF: Global assessment
of functioning;
IQR: Inter-quartile range; MSF: Médecins Sans Frontières
(Doctors without
borders); PTSD: Post-traumatic stress disorder.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
MC drafted the manuscript. AL participated in study design and
in drafting
the manuscript. TR performed data analysis. GC and MM
participated in
study design, coordinated data collection and provided ongoing
programmatic support. All authors read and approved the final
manuscript.
Acknowledgements
We thank the many mental health professionals and volunteers
who have
contributed their time and expertise over many years in Wudu
and
Beichuan, Tolima, Nablus and Gaza. Their dedication to
providing quality
mental health services in the face of often difficult conditions
made this
article possible. We thank the public health authorities in
China, Colombia,
48. Gaza and Nablus for their support. We also recognize the
important
collaborations with our partner organizations, notably the
Chinese Academy
of Science and Crisis Intervention Center in Wudu and
Beichuan.
Author details
1Epicentre, 8 rue Saint-Sabin, 75011 Paris, France. 2Médecins
Sans Frontières,
8 rue Saint-Sabin, 75011 Paris, France. 3Los Andes University,
School of
Medicine, Cr 7 N. 117-15, Bogota, Colombia. 4Hôpital Cochin,
Maison des
adolescents, Université de Paris 5, 97 Boulevard de Port Royal,
75670 Paris
cedex 14, France.
Received: 10 July 2013 Accepted: 24 October 2013
Published: 1 November 2013
References
1. Mollica RF, Cardozo BL, Osofsky HJ, Raphael B, Ager A,
Salama P: Mental
health in complex emergencies. Lancet 2004, 364:2058–2067.
2. De Jong JTVM, Komproe IH, Van Ommeren M: Common
mental disorders
in post-conflict settings. Lancet 2003, 361:2128–2130.
3. Neria Y, Nandi A, Galea S: Post-traumatic stress disorder
following
disasters: a systematic review. Psychol Med 2008, 38:467–480.
4. Madianos MG, Sarhan AL, Koukia E: Major depression
across West Bank: a
49. crosssectional general population study. Int J Soc Psychiatry
2011,
58:315–322.
Coldiron et al. Conflict and Health 2013, 7:23 Page 6 of 6
http://www.conflictandhealth.com/content/7/1/23
5. Canetti D, Galea S, Hall BJ, Johnson RJ, Palmieri PA,
Hobfoll SE: Exposure to
prolonged socio-political conflict and the risk of PTSD and
depression
among Palestinians. Psychiatry 2010, 73:219–231.
6. Espié E, Gaboulaud V, Baubet T, Casas G, Mouchenik Y,
Yun O, Grais RF,
Moro MR: Trauma-related psychological disorders among
Palestinian
children and adults in Gaza and West bank, 2005–2008. Int J
Ment Health
Syst 2009, 3:21.
7. Jones L, Asare JB, El Masri M, Mohanraj A, Sherief H, van
Ommeren M:
Severe mental disorders in complex emergencies. Lancet 2009,
374:654–661.
8. The Sphere Project: Humanitarian charter and minimum
standards in disaster
response. Geneva: The Sphere Project; 2011.
9. Van Ommeren M, Saxena S, Saraceno B: Mental and social
health during
and after acute emergencies: emerging consensus? Bull World
Health
50. Organ 2005, 83:71–76.
10. Inter-Agency Standing Committee: IASC guidelines on
mental health and
psychosocial support in emergency settings. Geneva: IASC;
2007.
11. Jordans MJD, Tol WA, Komproe IH, de Jong JTVM:
Systematic review of
evidence and treatment approaches: psychosocial and mental
health
care for children in war. Child Adolesc Ment Health 2009,
14:2–14.
12. Tol WA, Barbui C, Galappatti A, Silove D, Betancourt TS,
Souza R, Golaz A,
van Ommeren M: Mental health and psychosocial support in
humanitarian settings: linking practice and research. Lancet
2011,
378:1581–1591.
13. Moro MR: Establishment of a pyschological care center. In
Children and
Violence. Volume 11: The child in the family. Edited by
Chiland C, Gerald
Young J. Northvale: Aronson; 1994:125–144. Northvale.
14. Moro MR: Psychiatric interventions in crisis situations. The
Signal 1994,
2:1–4.
15. Winnicott DW: Therapeutic consultations in child
psychiatry. New York:
Hogarth Press; 1971.
16. Gaboulaud V, Reynaud C, Moro MR, Roptin J, Lachal C,
51. Brown V, Baubet T:
Pyschological support for Palestinian children and adults
referred to an
MSF program for behavioral and emotional disorders between
November 2000 and January 2006. Intervention 2010, 8:131–
142.
17. Ghosh N, Mohit A, Murthy RS: Mental health promotion in
post-conflict
countries. J R Soc Promot Health 2004, 124:268–270.
18. Baubet T, Moro MR: Cultures et soins du trauma psychique
en situation
humanitaire. In Soigner malgré tout: traumas, cultures et soins.
Edited by
Baubet T, Le Roch K, Bitar D, Moro MR. Grenoble: La Pensée
Sauvage;
2003:69–93.
19. Rousseau C, Measham T, Moro MR: Working with
interpreters in child
mental health. Child Adolesc Ment Health 2012, 16:55–59.
20. Weissman MM, Markowitz JC, Klerman GL: Comprehensive
guide to
interpersonal psychotherapy. New York: Basic Books and
Perseus Book Group;
2000.
21. Sanchez-Padilla E, Casas G, Grais RF, Hustache S, Moro
MR: The Colombian
conflict: a description of a mental health program in the
Department of
Tolima. Confl Health 2009, 3:13.
22. Llosa AE, Casas G, Thomas H, Mairal A, Grais RF, Moro
52. MR: Short and
longer-term psychological consequences of Operation Cast
Lead:
documentation from a mental health program in the Gaza Strip.
Confl Health 2012, 6:8.
23. Thabet AA, Vostanis P: Impact of political violence and
trauma in Gaza on
children’s mental health and types of interventions: a review of
research
evidence in a historical context. Int J Peace Dev Stud 2012,
2:214–218.
24. Bass JK, Annan J, Murray SM, Kaysen D, Griffiths S,
Cetinoglu T, Wachter K,
Murray LK, Bolton PA: Controlled trial of psychotherapy for
Congolese
survivors of Sexual violence. N Engl J Med 2013, 368:2182–
2191.
doi:10.1186/1752-1505-7-23
Cite this article as: Coldiron et al.: Brief mental health
interventions in
conflict and emergency settings: an overview of four Médecins
Sans
Frontières – France programs. Conflict and Health 2013 7:23.
Submit your next manuscript to BioMed Central
and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
53. • Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at
www.biomedcentral.com/submit
Reproduced with permission of the copyright owner. Further
reproduction prohibited without
permission.
1752-1505-7-23.pdf
The Journal of Emergency Medicine, Vol. 43, No. 1, pp. 76–82,
2012
Published by Elsevier Inc.
Printed in the USA
0736-4679/$ - see front matter
doi:10.1016/j.jemermed.2011.06.124
Prior Presentat
Society for Aca
Meeting – ‘‘Prev
lowing Hurricane
Mediterranean Em
2007; Southeast
Annual Meeting
University Medic
RECEIVED: 7 Jun
ACCEPTED: 1 Jun
54. Selected Topics:
Disaster Medicine
POST-TRAUMATIC STRESS DISORDER IN AN
EMERGENCY DEPARTMENT
POPULATION ONE YEAR AFTER HURRICANE KATRINA
Lisa D. Mills, MD,* Trevor J. Mills, MD, MPH,†‡ Marlow
Macht, MD,§ Rachel Levitan, MD,k Annelies De Wulf, MD,†‡
and Natasha S. Afonso, MD{
*Department of Emergency Medicine, University of California
Davis, Davis, California, †Section of Emergency Medicine,
Louisiana State
University Health Science Center, New Orleans, Louisiana,
‡Department of Veterans Affairs, New Orleans, Louisiana,
§Department of
Emergency Medicine, Denver Health Medical Center, Denver,
Colorado, kDepartment of Emergency Medicine, Maricopa
Medical Center,
Phoenix, Arizona, and {Department of Pediatrics, Weill Medical
College of Cornell University, New York, New York
Reprint Address: Trevor J. Mills, MD, MPH, Section of
Emergency Medicine, Louisiana State University Health Science
Center, 2021 Perdido
Street, New Orleans, LA 70115-3843
, Abstract—Background: Hurricane Katrina resulted in
a significant amount of injury, death, and destruction. Study
Objectives: To determine the prevalence of, and risk factors
for, symptoms of post-traumatic stress disorder (PTSD) in
an emergency department (ED) population, 1 year after
hurricane Katrina. Methods: Survey data including the
Primary Care PTSD (PC-PTSD) screening instrument, de-
mographic data, and questions regarding health care needs
and personal loss were collected and analyzed. Results:
55. Seven hundred forty-seven subjects completed the survey.
The PC-PTSD screen was positive in 38%. In the single
variate analysis, there was a correlation with a positive
PC-PTSD screen and the following: staying in New Orleans
during the storm (odds ratio [OR] 1.73, 95% confidence in-
terval [CI] 1.28–2.34), having material losses (OR 1.64, 95%
CI 1.03–2.60), experiencing the death of a loved one (OR
1.96, 95% CI 1.35–1.87), needing health care during the
storm (OR 2.01, 95% CI 1.48–2.73), and not having health
care needs met during the storm (OR 2.00, 95% CI 1.26–
3.18) or after returning to New Orleans (OR 2.29, 95% CI
ions: ‘‘Top Ten Most Newsworthy Abstracts’’
demic Emergency Medicine 2007 Annual
alence of Posttraumatic Stress Disorder Fol-
Katrina’’; also presented at the 4th Annual
ergency Medicine Congress, Sorrento, Italy
Society of Academic Emergency Medicine
2007; and the Eighteenth Annual Tulane
al School Research Day 2007.
e 2010; FINAL SUBMISSION RECEIVED: 2 February
e 2011
76
1.40–3.73). In the multivariate analysis, the death of a loved
one (OR 1.87, 95% CI 1.26–2.78), being in New Orleans dur-
ing the storm (OR 1.69, 95% CI 1.22–2.33), and seeking
health care during the storm (OR 1.69, 95% CI 1.22–2.35)
were associated with positive PC-PTSD screens. Conclu-
sions: There was a high prevalence of PTSD in this ED pop-
ulation surveyed 1 year after hurricane Katrina. By
targeting high-risk patients, disaster relief teams may
be able to reduce the impact of PTSD in similar popula-
tions. Published by Elsevier Inc.
, Keywords—post-traumatic stress disorder; public
56. health; disaster response; hurricane Katrina
INTRODUCTION
Hurricane Katrina made landfall on the Gulf Coast of
southeast Louisiana on the morning of Monday, August
29, 2005. The storm resulted in the most property damage
ever caused by a natural disaster, and the most deaths
caused by a natural disaster since 1928 (1). Over 1300
people were killed and $100 billion in assets were dam-
aged (1). An estimated 300,000 homes were completely
destroyed or made uninhabitable (2). In New Orleans,
80% of the metropolitan area flooded (3). Thousands
who remained in New Orleans during the storm and its
2011;
http://dx.doi.org/10.1016/j.jemermed.2011.06.124
PTSD in an ED Population after Katrina 77
aftermath experienced significant stressful events, includ-
ing exposure to extreme environmental conditions, hu-
man suffering, death, and violent behavior.
Hurricane evacuees also endured difficult circum-
stances. For those who evacuated from New Orleans, na-
tional television news coverage showed flooded property,
looting, and violence. These images may have affected
evacuees as they witnessed the destruction of their city.
Evacuees also directly dealt with lack of food and water,
heat, and unsafe living conditions. For those who returned
to post-Katrina New Orleans, there were continuing hard-
ships. Many were displaced from their homes, lived in
shelters or mobile homes, and experienced the lack of ba-
sic resources, such as electricity, water, telephone service,
and a reduced police force and health care system.
57. The diagnostic criteria for post-traumatic stress disor-
der (PTSD) stipulate the exposure to an inciting event that
involves actual or threatened death, or serious injury, to
oneself or others. Symptoms of PTSD include persis-
tently re-experiencing the traumatic event and consis-
tently avoiding stimuli associated with the trauma (4).
An estimated 7.8% of Americans will experience
PTSD at some point in their lives, corresponding with
an estimated 3.6% of adults aged 18–54 years who will
have PTSD in the course of a given year (5,6). Factors
associated with the development of PTSD symptoms
include psychiatric comorbidities and poor social
support (5). In prior studies of survivors of disasters, fac-
tors associated with the development of PTSD included
fear during the traumatic event, past traumatic experi-
ences, damage to the home, high levels of material loss,
loss of a loved one, continuing stressors, and continual re-
minders of the trauma (7–11). Female gender has been
associated with increased risk of development of PTSD
symptoms, however, this remains a subject of debate
(5,12). Furthermore, a person does not need to be
physically present at a traumatic event to develop PTSD
(13,14). People have been diagnosed with PTSD after
experiencing a traumatic event via the news, losing
a loved one, or hearing stories of a traumatic event.
Our hypothesis is that the stressors of the storm, both
during and immediately after hurricane Katrina, resulted
in a significant amount of PTSD in the population of New
Orleans. The purpose of this study was to determine the
prevalence of, and risk factors for, symptoms of PTSD
in an emergency department (ED) population, 1 year after
hurricane Katrina.
MATERIALS AND METHODS
58. Study Design
This cross-sectional study was conducted over 6 weeks in
July and August of 2006, 11–12 months after hurricane
Katrina struck the Gulf Coast. During each day of the
study period, in randomly selected 6-h blocks, research
personnel approached all people in the waiting room of
an interim public ED to assess eligibility and request con-
sent for an interview. The Louisiana State University
Health Science Center Institutional Review Board ap-
proved this study.
Study Setting and Population
Inclusion criteria were age $ 18 years at the time of the
study, those who were residents of the greater New
Orleans area at the time of the storm, and those who
gave verbal consent to answer the study questions. The
setting was the waiting room of the only operating public
ED within the city limits of New Orleans at the time.
Charity Hospital, one of the longest continually operating
public hospitals in the country, was closed 5 days after
Katrina’s landfall. In the year immediately after Katrina,
emergency care was delivered in a number of temporary
settings, including tents, the convention center, a Navy
ship, and a parking lot. At the time of the study, the Loui-
siana State University Interim Hospital had just opened
and the ED had a calculated volume of approximately
45,000 patient visits a year.
Study Protocol and Measurements
Trained research assistants conducted interviews using
a structured questionnaire that included demographics,
location of the person during the storm, material losses,
the experience of the death of a loved one, and health
59. care needs during and after Katrina. Material loss in-
cluded loss of an owned home, rented home, car, job,
pet, or personal property. The health care needs questions
were ‘‘yes/no’’ and included the questions ‘‘did you need
health care during or after the storm’’ and if yes, ‘‘was it
available?’’ The final items on the questionnaire were the
four questions of the Primary Care PTSD Screen (PC-
PTSD) (Table 1) (15). Although the questions are phrased
in the past tense, patients were instructed to relate their
symptoms at the time of the interview.
Participants with a positive screen were given written
information about local free mental health resources, and
encouraged to attend. There were no inpatient psychiatric
or psychiatric consultation services available at the time
of the study in the city of New Orleans.
Data Analysis
The primary dependent variable was a positive PC-PTSD
screen. A positive screen was defined as ‘‘yes’’ answers to
three of four items on the screen. This cutoff was selected
to maximize the specificity of the screen. In the study
Table 1. The Primary Care PTSD Screen (PC-PTSD)
In your life have you ever had any experience that was so
frightening, horrible, or upsetting that in the past month you:
1. Have had nightmares about it or thought about it when you
did not want to?
2. Tried hard not to think about it or went out of your way to
avoid situations that reminded you of it?
3. Were constantly on guard, watchful, or easily startled?
60. 4. Felt numb or detached from others, activities, or your
surroundings?
PTSD = post-traumatic stress disorder.
78 L. D. Mills et al.
validating this screen, a cutoff of three gives a sensitivity
of 0.78, with a specificity of 0.87, for an efficiency of 0.85
in a population of veterans with a PTSD prevalence of
24.5% (15).
The data were analyzed in Stata 9.2 (StataCorp, Col-
lege Station, TX). The data were first analyzed utilizing
univariate analysis, examining the relationship between
a positive PC-PTSD screen and gender, age (stratified
by decade), staying in New Orleans during the storm, ex-
periencing material losses, experiencing the death of
a loved one, needing health care either during the storm
or after returning to New Orleans, and whether or not
health care needs were met. For those who had material
losses, the specific material losses were also analyzed.
The categories of losses that were analyzed were owned
home, rented house, other personal property, car, pet,
and job. The responses to each of these questions were bi-
nary, except for deaths, where we included ‘‘unknown’’ as
a response for a missing but not confirmed dead relative.
All tests were two-tailed, with significance defined as
p < 0.05. The chi-squared test statistic was used except
where Fisher’s exact test was more appropriate.
To evaluate for interviewer bias, we tested for correla-
tion between each of the six interviewers and a positive
screen. There was no correlation between interviewer
and positive PTSD screens (Pearson chi-squared 6.4,
p = 0.265).
61. After completing the single variable analysis, vari-
ables were entered into a multivariable logistic regression
model, to allow adjustment for confounders. Due to the
expected colinearity, health care needs were included in
the multivariable model, but whether those health care
needs were met was not included. Model fit was assessed
with the Hosmer-Lemeshow goodness-of-fit test. The dis-
criminatory power of the model was investigated by gen-
erating a receiver operating characteristic curve for the
model and evaluating the area under the curve.
RESULTS
In the study period, 1181 people were approached, and
201 (17%) did not meet study criteria. Those who did
not meet criteria were under 18 years of age or were
not in New Orleans at the time of Katrina. Of the 908 el-
igible people, 783 (86%) consented and 747 (95%) peo-
ple completed the interview. The primary reason for
incomplete interviews was being called into the ED be-
fore completion of the interview. The prevalence of pos-
itive PC-PTSD screen in the population studied was 38%
(95% confidence interval [CI] 34.7–41.8%).
Demographics
Four hundred ten (55%) participants were women. The
mean age of participants was 42.2 years (SD 6 14.3
years). Thirty-nine percent of participants reported stay-
ing in New Orleans during the storm. Among the factors
analyzed, the most common was material loss, reported
by 87% (n = 648) of respondents. Of the material losses
reported, 459 (61% of total study participants) reported
the loss of a home, 209 reported loss of a home that
they owned, and 250 reported loss of a rented home.
Five hundred ninety-one (79%) reported loss of personal
62. property of value, 287 (38%) reported loss of a car, 89
(12%) reported loss of a pet, and 157 (21%) reported
loss of a job site.
Eighteen percent (n = 134) of participants experienced
the death of a loved one as a result of the storm. Over half
of the participants reported needing health care during the
storm (56%, n = 418) or after returning to New Orleans
(55%, n = 409). Of those who needed health care, 23%
(n = 95) reported that their needs were not met during
the storm. Twenty percent (n = 81) reported that their
health care needs were not met upon returning to the
city (Table 2).
Single-variable Analysis
There was no significant correlation between age (by de-
cade) and positive PC-PTSD screens (Pearson chi-
squared 14.1, p = 0.050). The data do show a significant
correlation with a positive PC-PTSD screen and staying
in New Orleans during the storm (OR 1.73, 95% CI
1.28–2.34), having material losses (OR 1.64, 95% CI
1.03–2.60), experiencing the death of a loved one (OR
1.96, 95% CI 1.35–1.87), needing health care during
the storm (OR 2.01, 95% CI 1.48–2.73), and not having
health care needs met either during the storm (OR 2.00,
95% CI 1.26–3.18) or after returning to New Orleans
(OR 2.29, 95% CI 1.40–3.73) (Table 3).
Table 2. Demographics of Study Participants (n = 747)
Number Percent
Positive PC-PTSD screen 285 38
63. Female gender 410 55
In New Orleans during Katrina 288 39
Experienced material loss 648 87
Home 459 61
Owned home 209 28
Rented home 250 34
Car 287 38
Other personal property of value 591 79
Job 157 21
Pet 89 12
Experienced death of a loved one 134 18
Needed health care during storm 418 56
Needed health care during storm but
not available (For this percentage,
n = 481)
95 23
Needed health care after storm 409 55
Needed health care after storm but not
available (For this percentage, n = 409)
81 20
PC-PTSD = primary care post-traumatic stress disorder.
PTSD in an ED Population after Katrina 79
Multi-variable Analysis
Female gender, being in New Orleans during the storm,
experiencing material losses, experiencing the death of
a loved one, and needing health care during the storm
or after returning were entered into the logistic regression
64. model. (Because there were only 27 participants over 65
years of age, age was not entered into the logistic regres-
sion model.) For this model, the Hosmer-Lemeshow
goodness-of-fit statistic was calculated at c
2(8) = 2.96,
p = 0.94. The area under a receiver operating characteris-
tic curve fitted to evaluate goodness of fit was 0.64, indi-
cating an adequate discriminatory power for the model.
In this model, experiencing the death of a loved one
carried the highest odds of a positive PC-PTSD screen
(OR 1.87, 95% CI 1.26–2.78). Being in New Orleans dur-
ing the storm (OR 1.69, 95% CI 1.22–2.33) and seeking
health care during the storm (OR 1.69, 95% CI 1.22–
2.35) were also associated with positive PC-PTSD
screens. There was no significant correlation with female
gender (OR 1.21, 95% CI 0.88–1.67), material losses (OR
Table 3. Single-variable Analysis of a Positive PC-PTSD
Screen and Risk Factors
OR Low High p Value
Female gender 1.21 0.90 1.64 0.1943
In New Orleans during Katrina 1.73 1.28 2.34 0.0003
Material losses 1.64 1.03 2.60 0.0352
Death of a loved one 1.96 1.35 2.87 0.0004
Needed health care during storm 2.01 1.48 2.73 0.0000
Health care not available during storm 2.00 1.26 3.18 0.0031
Needed health care after returning 1.14 0.85 1.53 0.3898
Health care not available after returning 2.29 1.40 3.73 0.0008
PC-PTSD = primary care post-traumatic stress disorder;
OR = odds ratio.
1.12, 95% CI 0.81–1.56), or seeking health care after re-
turning (OR 1.12, 95% CI 0.81–1.56) (Figure 1).
65. DISCUSSION
As hypothesized, we found a high prevalence (38.2%) of
PTSD in the population of New Orleans 1 year after hur-
ricane Katrina. This result is supported by other studies
conducted after the hurricane. A survey of the largest em-
ployer in the city 6 months after hurricane Katrina found
a PTSD rate of 19.2% (16). A separate study of police and
firefighters conducted by the Centers for Disease Control
and Prevention in the 2–3 months after the hurricane
showed a prevalence of PTSD rates of 19% and 22%, re-
spectively (17). Previous studies indicate that PTSD
symptoms may become chronic, with one- to two-thirds
of those suffering PTSD symptoms having incomplete
resolution years after the traumatic event (5,10,18,19).
Figure 1. Multivariable analysis of positive PC-PTSD (primary
care post-traumatic stress disorder) screen and risk factors.
NOLA = New Orleans, Louisiana; Material losses = exper-
ienced material losses during Katrina; HC = health care;
Needed HC during = needed health care during Katrina;
Needed HC after = needed health care after Katrina.
80 L. D. Mills et al.
Before the recent oil spill, unpublished data indicate that
levels of PTSD on the Gulf Coast continue to increase,
with PTSD prevalence up to 16–21% (20).
A number of variables were shown to be significantly
associated with the development of PTSD symptoms.
Nineteen percent of those interviewed reported the loss
of a loved one due to the hurricane. In both the univariate
and multivariate analysis, this was the most significant
risk factor for developing PTSD. In preparing for future
66. disasters, mental health services can potentially target
those who experience deaths in the family for early inter-
vention and services.
Having health care needs during the storm (56%) was
associated with PTSD. In addition, of those who needed
health care, those whose health care needs were not met
either during the hurricane (22%) or afterwards (20%)
were more likely to have a positive PTSD screen. Al-
though the causation is not clear, it is possible that those
individuals whose needs were not met were predisposed
to developing PTSD. Conversely, those with PTSD may
have been more likely to seek care or feel that their needs
were not met if their mental health conditions were not
addressed. The association between the need for health
care, those needs being unmet, and a positive PTSD
screen has important implications for disaster planning.
This study suggests that a robust response with attention
to health care needs, both for medical care and mental
health, may reduce the prevalence of PTSD and increase
well-being after a natural disaster.
Women made up roughly half of the interviewed pop-
ulation (55%). In this study, female gender was not asso-
ciated with a significantly increased likelihood of
developing PTSD symptoms. In previous disaster studies,
the increased prevalence of women with PTSD has been
linked to increased rates of trauma, such as rape and inti-
mate partner violence (12). Although there were multiple
media reports of sexual assault after the storm, a gender
difference in PTSD was not seen in our study.
Eighty-seven percent of those interviewed reported
material losses due to the storm. Unlike previous studies
that reported an increased risk of PTSD symptoms with
higher levels of material loss, no significant correlation
67. between positive PTSD screens and personal material
loss was found in this investigation (10). A possible ex-
planation is that material losses were present in the vast
majority of residents interviewed. Because material los-
ses were so prevalent in this cohort, this factor may
have less value as a predictor of a positive screen.
Because PTSD can have a detrimental effect on phys-
ical health, the prevalence of PTSD in New Orleans has
implications for the overall health of this community. A
study examining health problems in Vietnam War combat
veterans noted that those with a concurrent diagnosis of
PTSD were more likely to have physical health problems,
and that those with more severe PTSD symptoms also had
more physical problems (21). This evidence is particu-
larly concerning in the context of the health care crisis
in New Orleans. As of July 2007, only three of the seven
previously operating hospitals were open, two of which
were at partial capacity, dropping the total number of hos-
pital beds by two-thirds (22). Furthermore, the health care
workforce was drastically reduced. The Louisiana De-
partment of Health and Hospitals reported in April
2006 that there was less than one primary care physician
for every 3200 residents and less than one psychiatrist for
every 21,000 residents (23).
The high PTSD prevalence in New Orleans impacts
the safety of all members of the community. After the
hurricane, violent crime in the city increased dramatically
and has remained high. Violent crime is associated with
PTSD. According to a study of northern Ugandans ex-
posed to years of brutal conflict, those who exhibited
symptoms of PTSD or depression were more likely to
choose violent than non-violent means of conflict resolu-
tion and have a desire for retribution than those without
symptoms of PTSD (24). A separate study found that
68. Congolese and Ugandan child soldiers with symptoms
of PTSD were less open to reconciliation and had more
feelings of revenge (25). In pre-Katrina New Orleans, es-
timates of murder rates by population made it the deadli-
est city in the United States, with rates rising since 2004
(26). Although the exact homicide rate in 2006 is hard to
pin down, due to variable estimates of the remaining pop-
ulation, by even the most generous population estimates,
in the year after hurricane Katrina, New Orleans main-
tained the highest homicide rate in the country. It is pos-
sible that the high prevalence of PTSD in New Orleans
contributes to the violence seen in the city.
Despite the high level of PTSD in this study, as well as
mental health issues seen in several other studies, avail-
ability of mental health care 1 year after Katrina remained
limited in New Orleans (16,17). There were limited
mental health clinics as well as inpatient beds, and
patients often waited for days in the EDs for inpatient
placement.
When planning for immediate and long-term disaster
relief, it is clear that mental health needs must be ad-
dressed. With early identification and treatment of a pop-
ulation at risk for PTSD, symptoms may be reduced and
the overall health of the community could be improved.
Limitations
By virtue of being in an ED waiting room, participants
may have had a higher pre-test likelihood of illness and
injury. Because it was a public hospital, those interviewed
also may have been of a lower socioeconomic status, thus
having a higher likelihood of PTSD risk factors such as
69. PTSD in an ED Population after Katrina 81
concurrent stressors, lower baseline health status, and
previous trauma.
We did not examine concurrent psychiatric disorders.
Given the high prevalence of comorbidities in individuals
with PTSD, it is likely that high rates of other anxiety and
mood disorders also exist in this population.
We did not screen for sexual assault. Patients who expe-
rienced thistype of assault may have a higher rateof PTSD.
Another limitation is the voluntary nature of the inter-
view, which could not be avoided. Those who refused an
interview may have done so due to the emotional content
of the interview, concurrent stresses, fatigue, somatic
complaints, or other factors that may have altered
PTSD screen results.
Due to the setting, as well as time and resource limita-
tions for the interviews, we performed a screening test,
rather than using more complete PTSD inventories or
a complete psychiatric interview. Given the high specific-
ity of the screen, we felt that this screen effectively bal-
anced time and accuracy.
This study measured prevalence of PTSD symptoms 1
year after hurricane Katrina, not the incidence. Without
previous studies of PTSD prevalence in this population,
we cannot assume that the high prevalence of positive
PTSD screens is solely associated with experiencing the
hurricane. It is possible that the population studied in
this cohort had previously higher rates of PTSD than
the general population of the United States.
70. CONCLUSION
The response to national disasters continues to evolve,
and includes the leadership of emergency physicians. In
this study, there was a high prevalence of PTSD in post-
Katrina New Orleans. Staying in New Orleans, experi-
encing the death of a loved one, and needing health
care during the storm were associated with significantly
increased odds of having symptoms of PTSD. By target-
ing patients in the ED for referral and treatment, disaster
relief teams may be able to reduce the impact of PTSD in
similar populations.
Acknowledgments—The authors would like to thank Katie Hall
and Makalah Solway for their assistance in performing inter-
views. Additionally, we appreciate Dr. Jan Johnson’s input on
this manuscript. Finally, we would like to thank the participants
of this study, who told us their stories.
REFERENCES
1. Hurricane Katrina: lessons learned - Chapter One: Katrina in
per-
spective; 2007. Available at:
http://www.whitehouse.gov/reports/
katrina-lessons-learned/. Accessed September 9, 2008.
2. Chertoff M. Statement of Michael Chertoff, US Department
of
Homeland Security before the Senate Committee on Homeland
Security and Governmental Affairs. Homeland Security Digital
Library 2006;848:1.
3. Knabb RD, Rhome JR, Brown DP. Tropical cyclone report:
Hurri-
cane Katrina, August 23–30, 2005. National Hurricane Center.
Available at: http://www.disastersrus.org/katrina/TCR-
71. AL122005_
Katrina.pdf. Accessed December 12, 2005.
4. American Psychiatric Association. Diagnostic and statistical
man-
ual of mental disorders: DSM-IV-TR. Washington, DC:
American
Psychiatric Association; 2000.
5. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB.
Post-
traumatic stress disorder in the National Comorbidity Survey.
Arch Gen Psychiatry 1995;52:1048–60.
6. Executive summaryof mental health: a report from the
SurgeonGen-
eral; 2007 (Chapter 2). Available at:
http://www.surgeongeneral.
gov/library/mentalhealth/home.html. Accessed December 12,
2007.
7. Galea S, Ahern J, Resnick H, et al. Psychological sequelae of
the
September 11 terrorist attacks in New York City. N Engl J Med
2002;346:982–7.
8. North CS, Nixon SJ, Shariat S, et al. Psychiatric disorders
among survivors of the Oklahoma City bombing. JAMA 1999;
282:755–62.
9. Basoglu M, Kilic C, Salcioglu E, Livanou M. Prevalence of
post-
traumatic stress disorder and comorbid depression in earthquake
survivors in Turkey: an epidemiological study. J Trauma Stress
2004;17:133–41.
72. 10. Armenian HK, Morikawa M, Melkonian AK, et al. Loss as a
deter-
minant of PTSD in a cohort of adult survivors of the 1988 earth-
quake in Armenia: implications for policy. Acta Psychiatr Scand
2000;102:58–64.
11. Goenjian AK, Steinberg AM, Najarian LM, Fairbanks LA,
Tashjian M, Pynoos RS. Prospective study of posttraumatic
stress,
anxiety, and depressive reactions after earthquake and political
vio-
lence. Am J Psychiatry 2000;157:911–6.
12. Yehuda R. Post-traumatic stress disorder. N Engl J Med
2002;346:
108–14.
13. Dixon P, Rehling G, Shiwach R. Peripheral victims of the
Herald of
Free Enterprise disaster. Br J Med Psychol 1993;66:193–202.
14. Schuster MA, Stein BD, Jaycox L, et al. A national survey
of stress
reactions after the September 11, 2001, terrorist attacks. N Engl
J
Med 2001;345:1507–12.
15. Prins A, Ouimette P, Kimerling R, et al. The primary care
PTSD
screen (PC-PTSD): development and operating characteristics.
Prim Care Psychiatr 2004;9:9–14.
16. DeSalvo KB, Hyre AD, Ompad DC, Menke A, Tynes LL,
Muntner P. Symptoms of posttraumatic stress disorder in a New
Or-
leans workforce following Hurricane Katrina. J Urban Health
73. 2007;
84:142–52.
17. Centers for Disease Control and Prevention (CDC). Health
hazard
evaluation of police officers and firefighters after Hurricane
Katrina: New Orleans, Louisiana, October 17–28 and November
30–December 5, 2005. MMWR Morb Mortal Wkly Rep 2006;55:
456–8.
18. Norris FH, Murphy AD, Baker CK, Perilla JL. Postdisaster
PTSD
over four waves of a panel study of Mexico’s 1999 flood. J
Trauma
Stress 2004;17:283–92.
19. North CS, Kawasaki AMSW, Spitznagel EL, Hong BA. The
course
of PTSD, major depression, substance abuse, and somatization
after
a natural disaster. J Nerv Ment Dis 2004;192:823–9.
20. Mental health on the decline in the Gulf Coast - Mental
Health.
MSNBC.com. August 21, 2007. Available at:
http://www.msnbc.
msn.com/id/20381086. Accessed December 2007.
21. Beckham JC, Moore SD, Feldman ME, Hertzberg MA,
Kirby AC, Fairbank JA. Health status, somatization, and
severity
of posttraumatic stress disorder in Vietnam combat veterans
with posttraumatic stress disorder. Am J Psychiatry 1998;155:
1565–9.
22. Eaton L. New Orleans recovery is slowed by closed
74. hospitals. The
New York Times July 24, 2007.
http://www.whitehouse.gov/reports/katrina-lessons-learned/
http://www.whitehouse.gov/reports/katrina-lessons-learned/
http://www.disastersrus.org/katrina/TCR-AL122005_Katrina.pdf
http://www.disastersrus.org/katrina/TCR-AL122005_Katrina.pdf
http://www.surgeongeneral.gov/library/mentalhealth/home.html
http://www.surgeongeneral.gov/library/mentalhealth/home.html
http://www.msnbc.msn.com/id/20381086
http://www.msnbc.msn.com/id/20381086
82 L. D. Mills et al.
23. Department of Health and Hospitals, State of Louisiana.
Primary care
and rural health; 2007. Available at:
http://www.dhh.louisiana.gov/
offices/news.asp?ID=88&Detail=857. Accessed September 9,
2008.
24. Vinck P, Pham PN, Stover E, Weinstein HM. Exposure to
war
crimes and implications for peace building in northern Uganda.
JAMA 2007;298:543–54.
25. Bayer C, Klasen F, Adam H. Association of trauma and
PTSD
symptoms with openness to reconciliation and feelings of
revenge
among former Ugandan and Congolese child soldiers. JAMA
2007;298:555–9.
26. VanLandingham MJ. Murder rates in New Orleans, La,
2004–2006.
Am J Public Health 2007;97:1614–6.
ARTICLE SUMMARY
75. 1. Why is this topic important?
Emergency physicians continue to be on the forefront
of disaster response. The disaster response team should
consider the immediate and delayed mental health needs
of affected populations to be part of overall health.
2. What does this study attempt to show?
This study shows the mental health impact of a major
natural disaster.
3. What are the key findings?
Key findings include the fact that a significant number
of individuals had symptoms of post-traumatic stress dis-
order 1 year after hurricane Katrina.
4. How is patient care impacted?
Health care, including mental health, is an integral part
of disaster relief and rebuilding. This response requires
prolonged individual, local, state, and national resources.
This study reveals the impact of a natural disaster on the
mental health of a population hurt by a storm and ham-
pered by a slow recovery.
http://www.dhh.louisiana.gov/offices/news.asp?ID=88%26Detai
l=857
http://www.dhh.louisiana.gov/offices/news.asp?ID=88%26Detai
l=857Post-traumatic Stress Disorder in an Emergency
Department Population One Year after Hurricane
KatrinaIntroductionMaterials and MethodsStudy DesignStudy
Setting and PopulationStudy Protocol and MeasurementsData
AnalysisResultsDemographicsSingle-variable AnalysisMulti-
variable AnalysisDiscussionLimitationsConclusionReferences
76. BRIEF REPORT
Emergency Department Predictors of Posttraumatic Stress
Reduction for
Trauma-Exposed Individuals With and Without an Early
Intervention
Matthew Price
University of Vermont
Megan Kearns
Centers for Disease Control and Prevention and
Emory University School of Medicine
Debra Houry and Barbara O. Rothbaum
Emory University School of Medicine
Objective: Recent data have supported the use of an early
exposure intervention to promote a reduction
in acute stress and posttraumatic stress disorder (PTSD)
symptoms after trauma exposure. The present
study explored a comprehensive predictive model that included
history of trauma exposure, dissociation
at the time of the trauma and early intervention, and
physiological responses (cortisol and heart rate) to
determine which variables were most indicative of reduced
PTSD symptoms for an early intervention or
treatment as usual. Method: Participants (n � 137) were
randomly assigned to the early intervention
condition (n � 68) or assessment-only condition (n � 69) while
receiving care at the emergency
department of a Level 1 trauma center. Follow-up assessments
occurred at 4 and 12 weeks posttrauma.
Results: Findings suggested that dissociation at the time of the
77. 1st treatment session was associated with
reduced response to the early intervention. No other predictors
were associated with treatment response.
For treatment as usual, cortisol levels at the time of acute care
and dissociation at the time of the traumatic
event were positively associated with PTSD symptoms.
Conclusions: Dissociation at the time at which
treatment starts may indicate poorer response to early
intervention for PTSD. Similarly, dissociation at
the time of the event was positively related to PTSD symptoms
in those who received treatment as usual.
Recent work has suggested exposure therapy administered
shortly after a trauma can reduce subsequent posttraumatic
stress
disorder (PTSD) symptoms (Rothbaum et al., 2012). The
variabil-
ity in outcomes, however, highlights a need to identify
predictors
of response in order to target treatment to those at greatest risk
and
those most likely to benefit (Kearns, Ressler, Zatzick, & Roth-
baum, 2012). The present study evaluated several variables
theo-
rized to predict response to an early intervention due to their
enhancement of fear acquisition after a trauma (Craske et al.,
2008). These variables include childhood trauma exposure,
heart
rate, cortisol levels, and dissociation.
Childhood trauma exposure is hypothesized to influence re-
sponse to an adulthood trauma. Childhood exposure may
establish
fear pathways that are strengthened after exposure to
subsequent
78. stressful events (Clemmons, Walsh, DiLillo, & Messman-
Moore,
2007). Indeed, childhood traumas are associated with more
severe
PTSD symptoms after an adulthood trauma (Nishith, Mechanic,
&
Resick, 2000). Those with such histories may be less likely to
benefit from early intervention after an adulthood trauma as a
result. Prior work is inconclusive on the influence of childhood
trauma on treatment outcome in chronic PTSD samples,
however.
Hembree, Street, Riggs, and Foa (2004) reported childhood
trauma
exposure was associated with reduced PTSD symptoms for pro-
longed exposure (PE), whereas Resick, Nishith, and Griffin
(2003)
did not find this association using PE or cognitive processing
therapy (CPT).
The initial physiological response to trauma may also enhance
fear acquisition. An elevated heart rate (HR) 1 week post-
trauma
was indicative of increased PTSD symptoms 4 months (Shalev
et
al., 1998), 6 months (Bryant, Harvey, Guthrie, & Moulds,
2000),
and 2 years later (Bryant & Harvey, 2002). Similarly,
posttrauma
cortisol has been negatively related to increased PTSD
symptoms
(for a review see DiGangi et al., 2013). Three studies suggested
baseline cortisol was not predictive of symptom reduction
during
treatment (Gerardi, Rothbaum, Astin, & Kelley, 2010; Olff, de
This article was published Online First February 3, 2014.
79. Matthew Price, Department of Psychology, University of
Vermont;
Megan Kearns, Centers for Disease Control and Prevention, and
Depart-
ment of Psychiatry and Behavioral Sciences, Emory University
School of
Medicine; Debra Houry, Department of Emergency Medicine,
Emory
University School of Medicine; Barbara O. Rothbaum,
Department of
Psychiatry and Behavioral Sciences, Emory University School
of Medi-
cine.
This work was supported by National Institute of Mental Health
Grant
R34MH083078 (principal investigator: Barbara O. Rothbaum)
and Emory
Center for Injury Control, Centers for Disease Control and
Prevention
Grant 5R49CE001494 (principal investigator: Debra Houry).
The study
was registered with clinicaltrials.gov (NCT00895518).
Correspondence concerning this article should be addressed to
Matthew
Price, Department of Psychology, University of Vermont,
Burlington, VT
05405. E-mail: [email protected]
T
hi
s
do