DEFINITION
Preterm labouris defined as one where the labour
starts before the 37th
completed weeks counting from
the first day of the last menstrual period
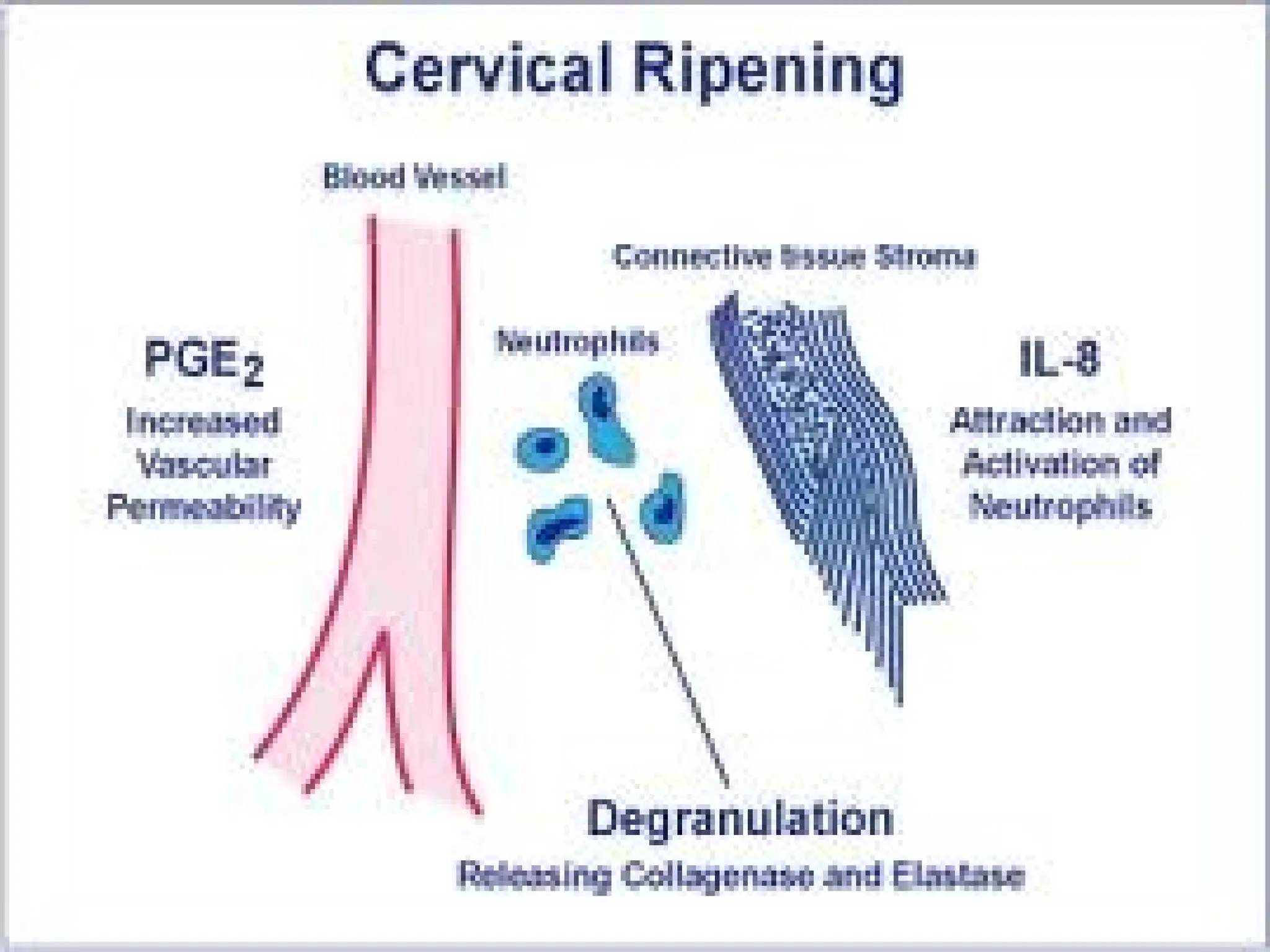
Etiopathogenesis
Decidual cells andmacrophages produce
cytokines
Increase synthesis of prostaglandins and
leukotrienes
Initiate pre term contraction
10.
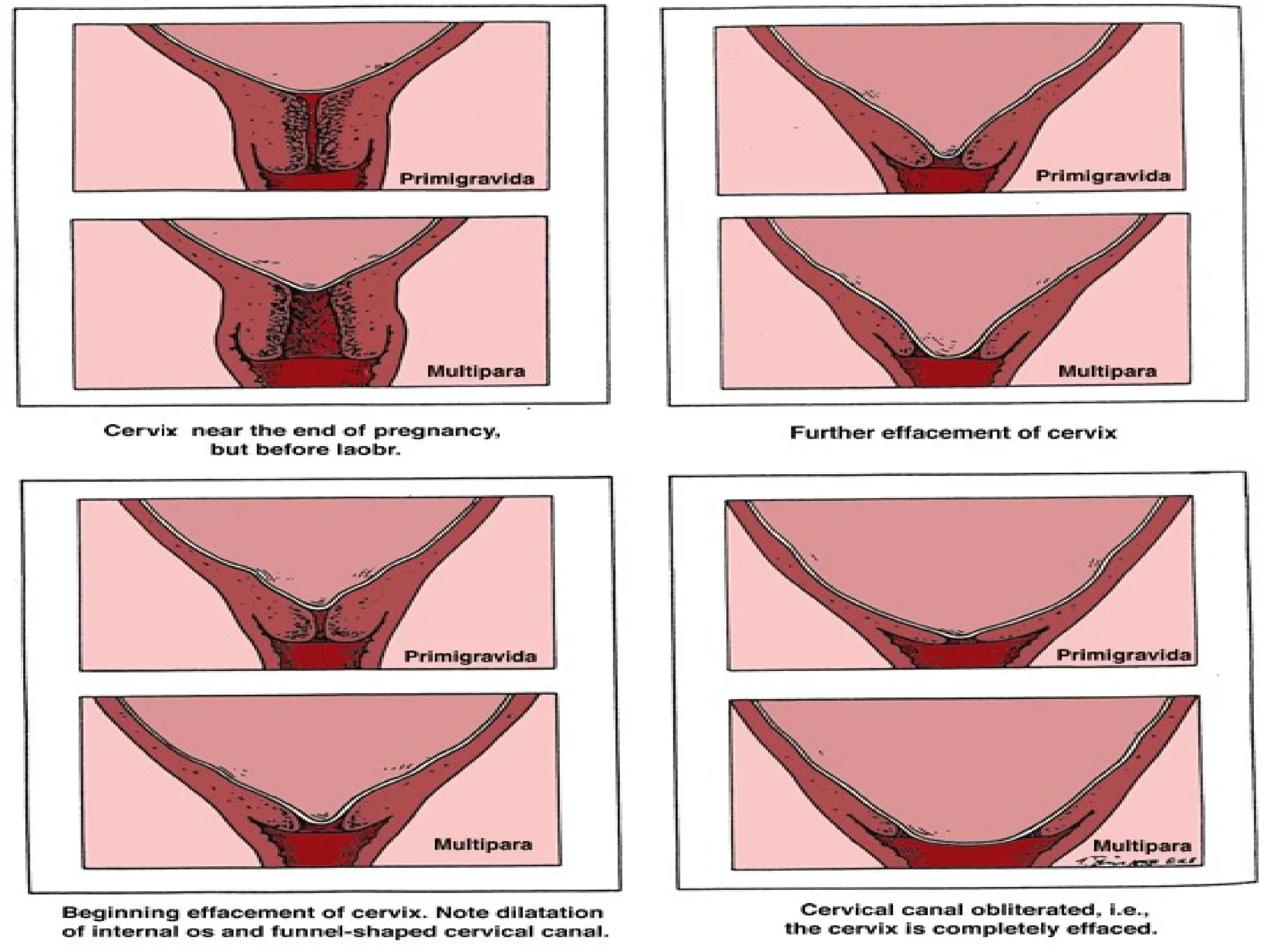
Diagnosis
Regular uterine contractionwith or without pain
( 1 in 10 minute)
Dialation (2cm)
Effacement ( 80%)
Pelvic pressure
Back ache
Vaginal discharge
11.
Management
OBJECTIVES
1.To prevent preterm onset of labour
2.To arrest pre term labour
3.To minimise perinatal mortality and
morbidity
4.Appropriate management of labour
5.Effective neonatal care
12.
Prevention
Identification ofrisk factors
Rest
Nutritional supplement
Avoidance of smocking
Encerclage operation
Premature effacement with irritable uterus and early engagement
of head
Tocolytic agent
Bed rest
Be sure about the gestational age before induction
Selective continuation of complicated pregnancy
Rest
Appropriate therapy
Early hospitalisation
To arrest preterm labour
Adequate rest
Left lateral position
Adequate sedation
Diazepam 5mg
Phenobarbitone 30- 60 mg
Adequate hydration
Antibiotic if there is infection
Tocolytic agents ( short and long term therapy)
Contd…
Contraindications
1. Maternal
•Diabetes
• Thyrotoxicosis
• Hypertension
• Cardiac disease
• Haemorrhage
2. Fetal
• Fetal distress
• Fetal death
• Congenital malformation
• Pregnancy beyond 34 weeks
3. Others
• Rupture of membrane
• Cervical dialatation more than 4 cm
• Chorioamnionitis
17.
Long term therapy
Pregnancyprior to 34 weeks
Pregnancy can be continued for at least one week
Benificial when pregnancy beyond 48 hours but less than 7
days
Glucocorticoid therapy
Betamethasone 12mg IM every 12hrs - 2 doses
Dexametasone 8mg IM every 12 hrs - 3 doses
Contraindication
PROM
Pre eclampsia
Delivery time is outside 24hrs – 7 day interval
First stage
Patientis put to bed to prevent PROM
Ensure adequate oxygenation
Strong sedatives and acceleration should be avoided
Watch during labour
Delay - LSCS
20.
Second stage
Birthshould be gentle and slow
Liberal episiotomy
Tendency to delay curtailed by forceps
Cord is to be clamped immediately to prevent hypervolemia
and hyperbilirubinemia
Place baby in NICU
21.
LSCS
Before 34wks with breech
Lower segment or j shaped incision is preferred
22.
Nursing Diagnosis
1. Alteredcardiopulmonary tissue perfusion related to the
effects of tocolytic agents
2. Fear related to the uncertainity of outcome and effects of
preterm labour on fetus
3. Impaired gas exchange related to lung immaturity
4. Pain related to uterine contraction
5. Ineffective management of therapeutic regimen related to
the lack of knowledge and complexity of therapy
6. Diversional activity deficit related to the imposed bed rest
23.
Contd…
7. Constipation relatedto decreased gastrointestinal motility
from prolonged bed rest / adverse effect of tocolytic agent
8. Situational low self esteem related to the feeling of
inadequacy from pre term labour complications
9. Knowledge deficit related to the treatment of preterm labour
Definition
Spontaneous rupture ofthe membranes any time
beyond 28th
week of pregnancy but before the
onset of labour is called premature (pre labour)
rupture of membranes.
26.
TERM PROM
Whenthe rupture occurs beyond 37th
week but before the onset
of labour it is called term PROM
PRE TERM PROM
When the rupture occurs before the 37th
completed weeks it is
called preterm PROM
PROLONGED RUPTURE OF MEMBRANE
Rupture of membrane for 24 hours before delivery is called
prolonged rupture of membrane
Causes
Increased friabilityof the membranes
Decreased tensile strength of the membranes
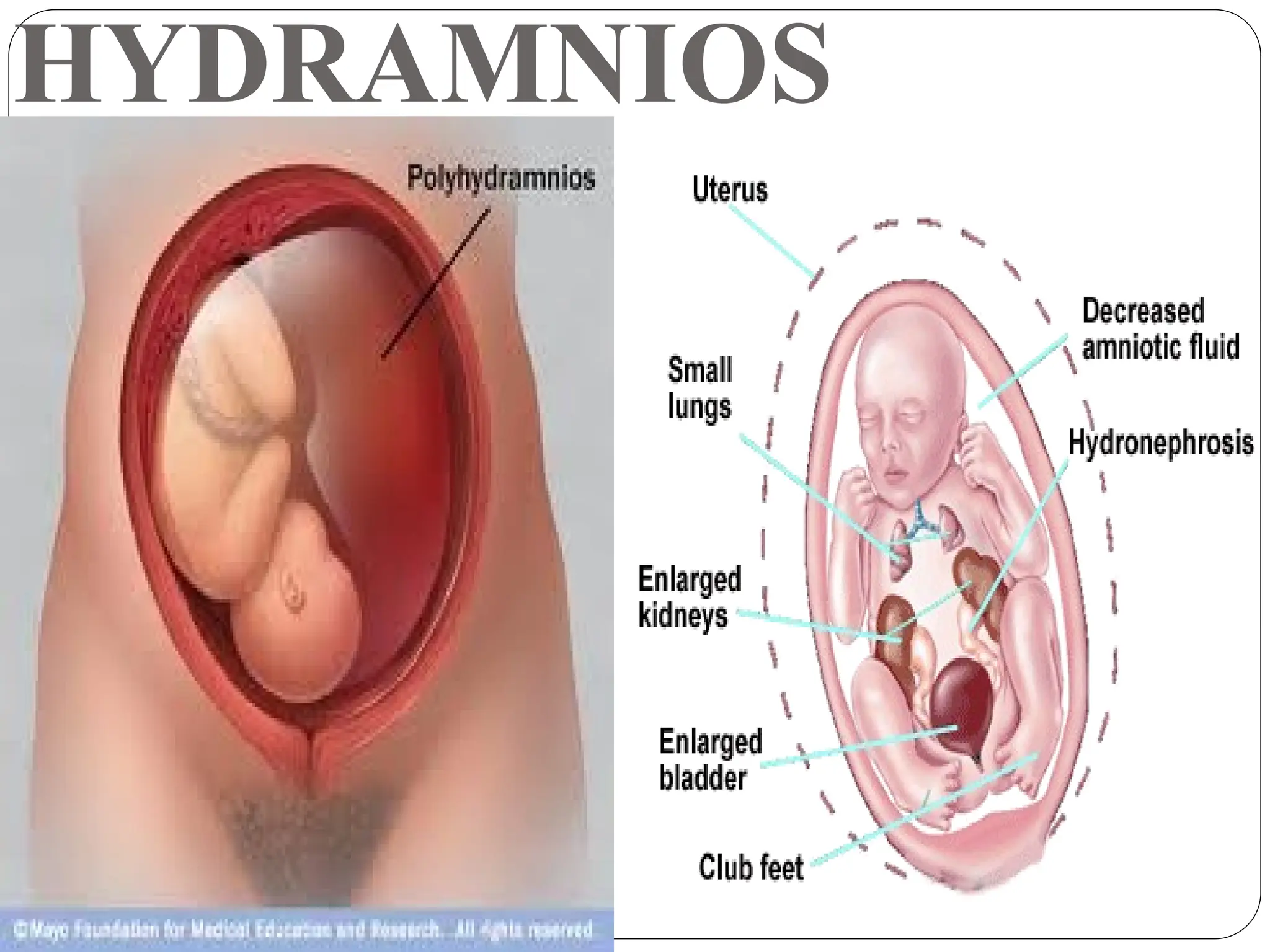
Polyhydramnios
Cervical incompetence
Multiple pregnancy
Infection – Chorio-amnionitis, UTI, lower genital tract
infections
29.
Diagnosis
Subjective symptomis
Escape of watery discharge per vagina either as a gush or
slow leak.
Usually confused with
1. Hydrorrhoea gravidarum
2. Incontinence of urine
30.
Confirmation of Diagnosis
1.Speculum examination
2. Examination of the collected fluid from posterior fornix
for
Detection of pH ( 6 – 6.2)
Ferning pattern
3. 0.1% Nile blue sulphate test – orange blue colouration of
cells
4. USG
31.
Investigations
Complete bloodcount
Urine analysis and culture
High vaginal swab for culture
Vaginal pool to estimate phosphatidyl glycerol
USG
NST
32.
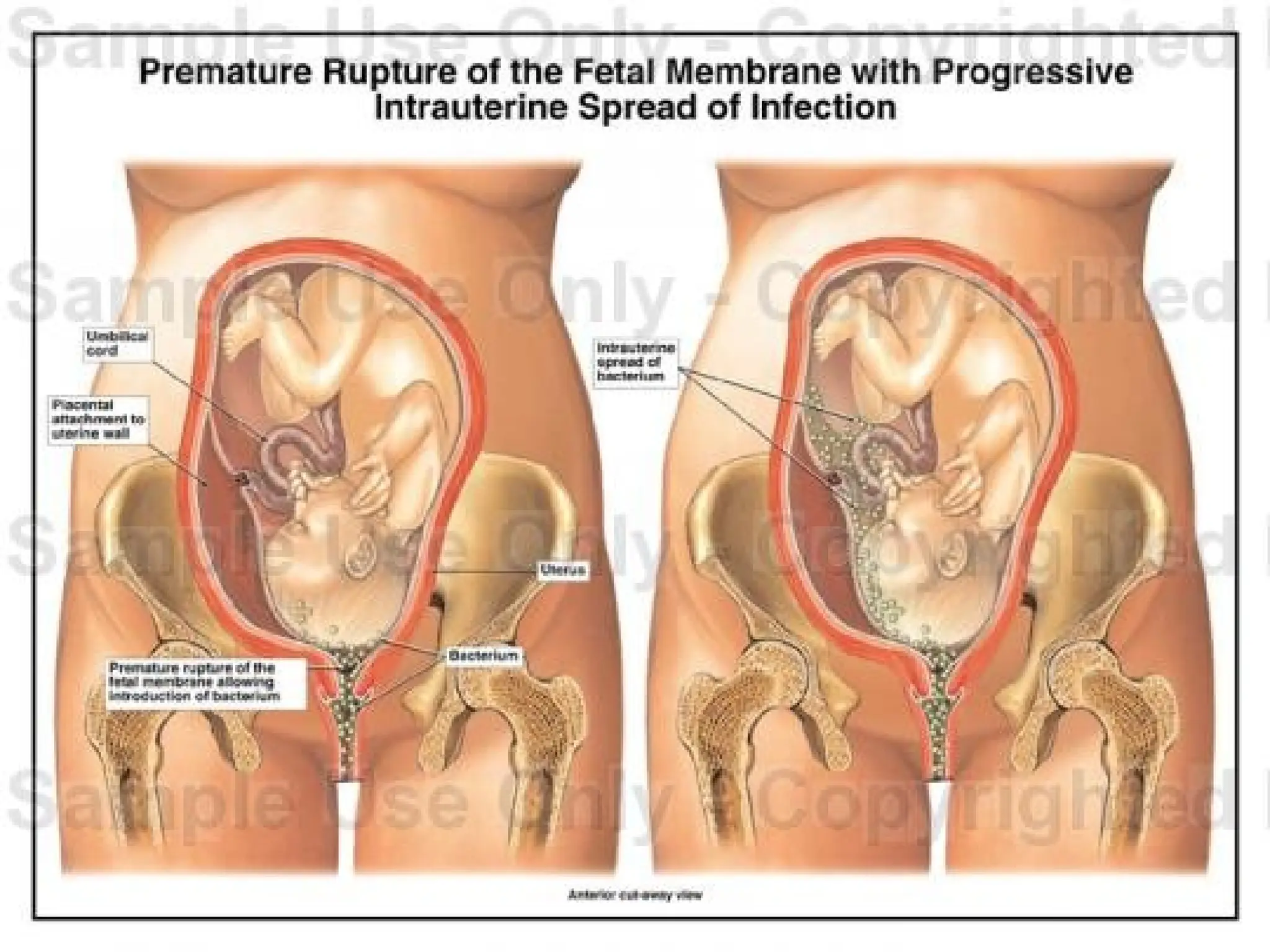
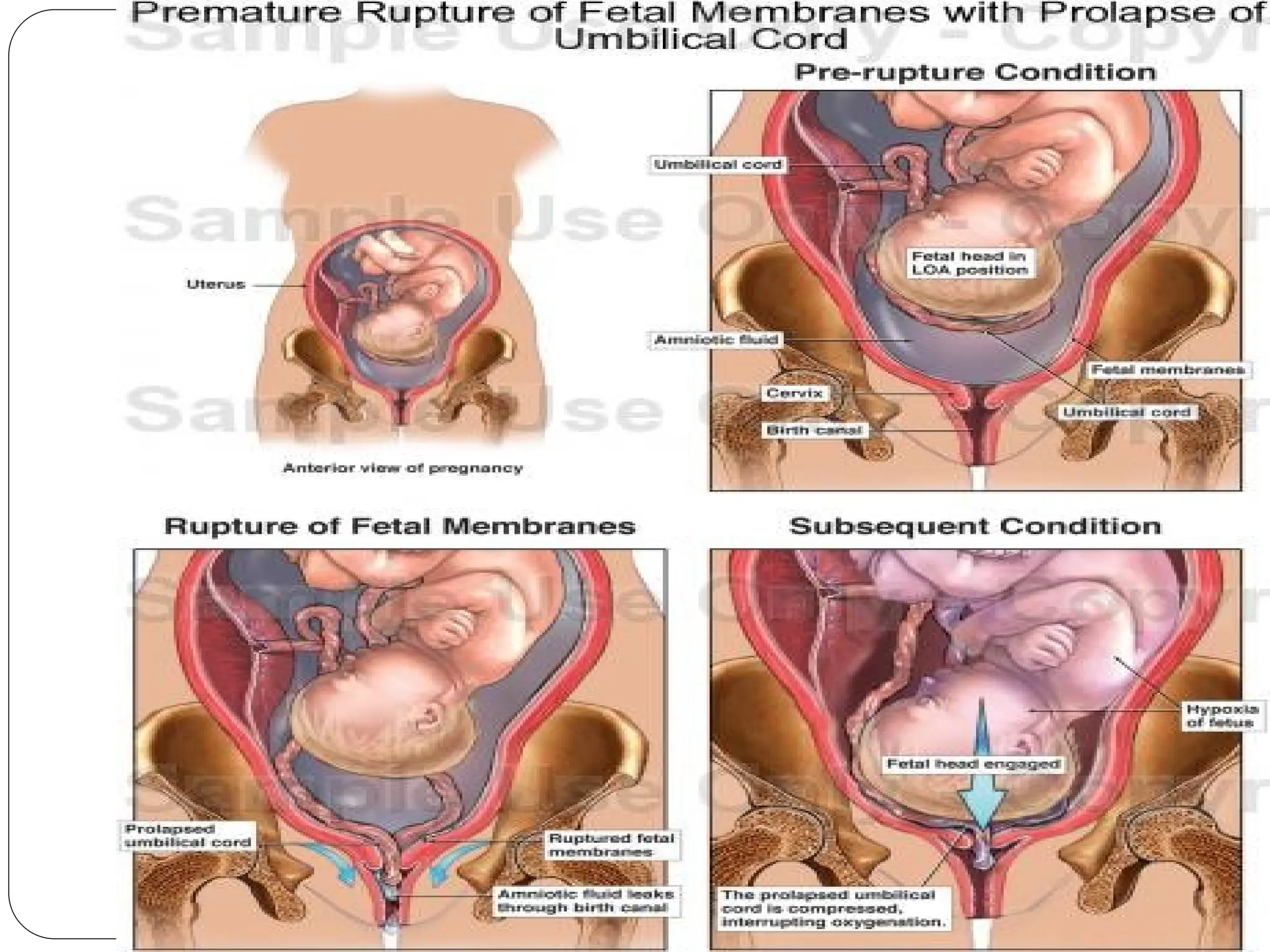
Dangers
Preterm labour andprematurity
Ascending infection
Cord prolapse
Dry labour
Fetal pulmonary hypoplasia
R.D.S
35.
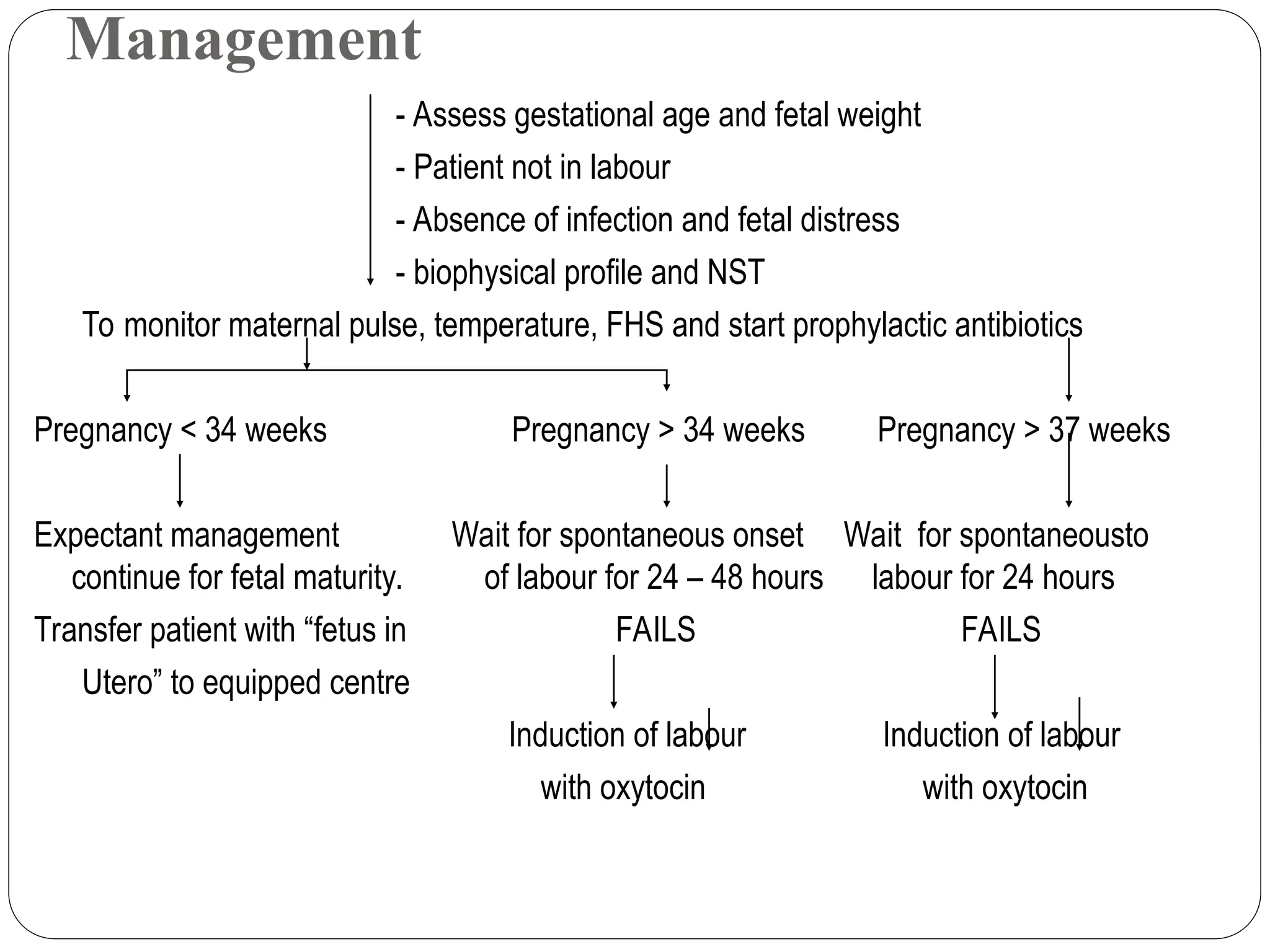
Management
- Assess gestationalage and fetal weight
- Patient not in labour
- Absence of infection and fetal distress
- biophysical profile and NST
To monitor maternal pulse, temperature, FHS and start prophylactic antibiotics
Pregnancy < 34 weeks Pregnancy > 34 weeks Pregnancy > 37 weeks
Expectant management Wait for spontaneous onset Wait for spontaneousto
continue for fetal maturity. of labour for 24 – 48 hours labour for 24 hours
Transfer patient with “fetus in FAILS FAILS
Utero” to equipped centre
Induction of labour Induction of labour
with oxytocin with oxytocin
39.
Meaning
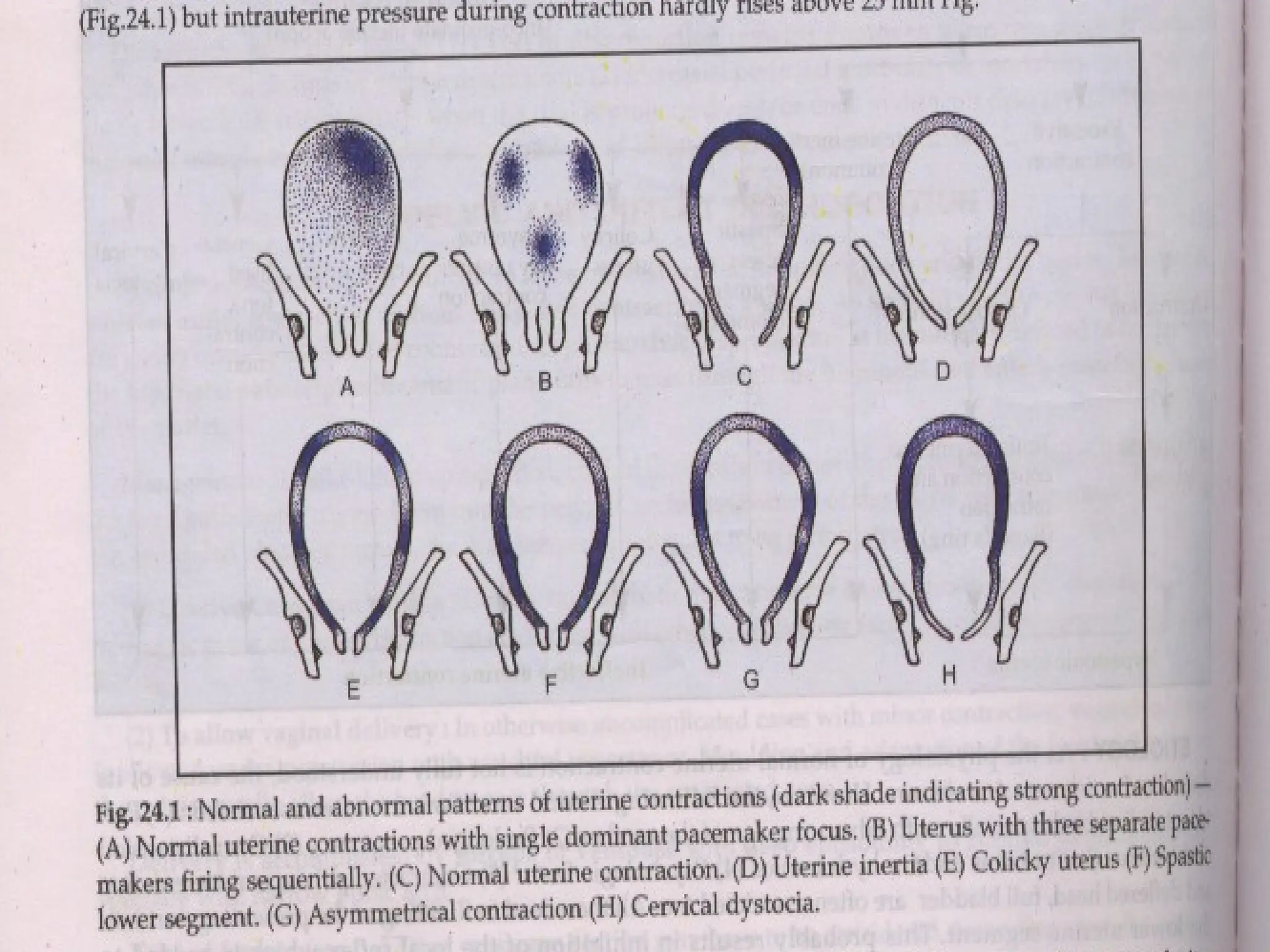
Any deviation ofthe normal pattern of
uterine contractions affecting the
course of labour is called abnormal
uterine action
40.
Etiology
Advancing age ofthe mother
Prolonged pregnancy
Over distention of the uterus due to twins
Psychological Factors
Contracted pelvis
Malpresentations
Full bladder
Precipitate Labour
Precipitate Labour
Definition:
Alabour lasting less than 3 hours
Etiology: More common in multipara when there are
strong uterine contractions
roomy pelvis
small sized pelvis
minimal soft tissue resistance
44.
Complications
Maternal:
Lacerations ofthe cervix, vagina
and perineum.
Shock.
Inversion of the uterus.
Postpartum haemorrhage:
no time for retraction,
lacerations.
Sepsis due to:
lacerations,
inappropriate surroundings.
Foetal:
Intracranial haemorrhage due to
sudden compression and
decompression of the head.
Foetal asphyxia due to:
strong frequent uterine
contractions reducing placental
perfusion,
lack of immediate resuscitation.
Avulsion of the umbilical cord.
Foetal injury due to falling down.
45.
Management
Before delivery
Patient whohad previous precipitate labour should be hospitalized
before expected date of delivery as she is more prone to repeated
precipitate labour.
During delivery
Inhalation anaesthesia: as nitrous oxide and oxygen is given to
slow the course of labour.
Tocolytic agents: as ritodrine (Yutopar) may be effective.
Episiotomy: to avoid perineal lacerations and intracranial
haemorrhage.
After delivery
Examine the mother and foetus for injuries.
46.
EXCESSIVE UTERINE CONTRACTIONAND
RETRACTION
Physiological Retraction Ring
It is a line of demarcation between the upper and lower uterine segment
present during normal labour and cannot usually be felt abdominally.
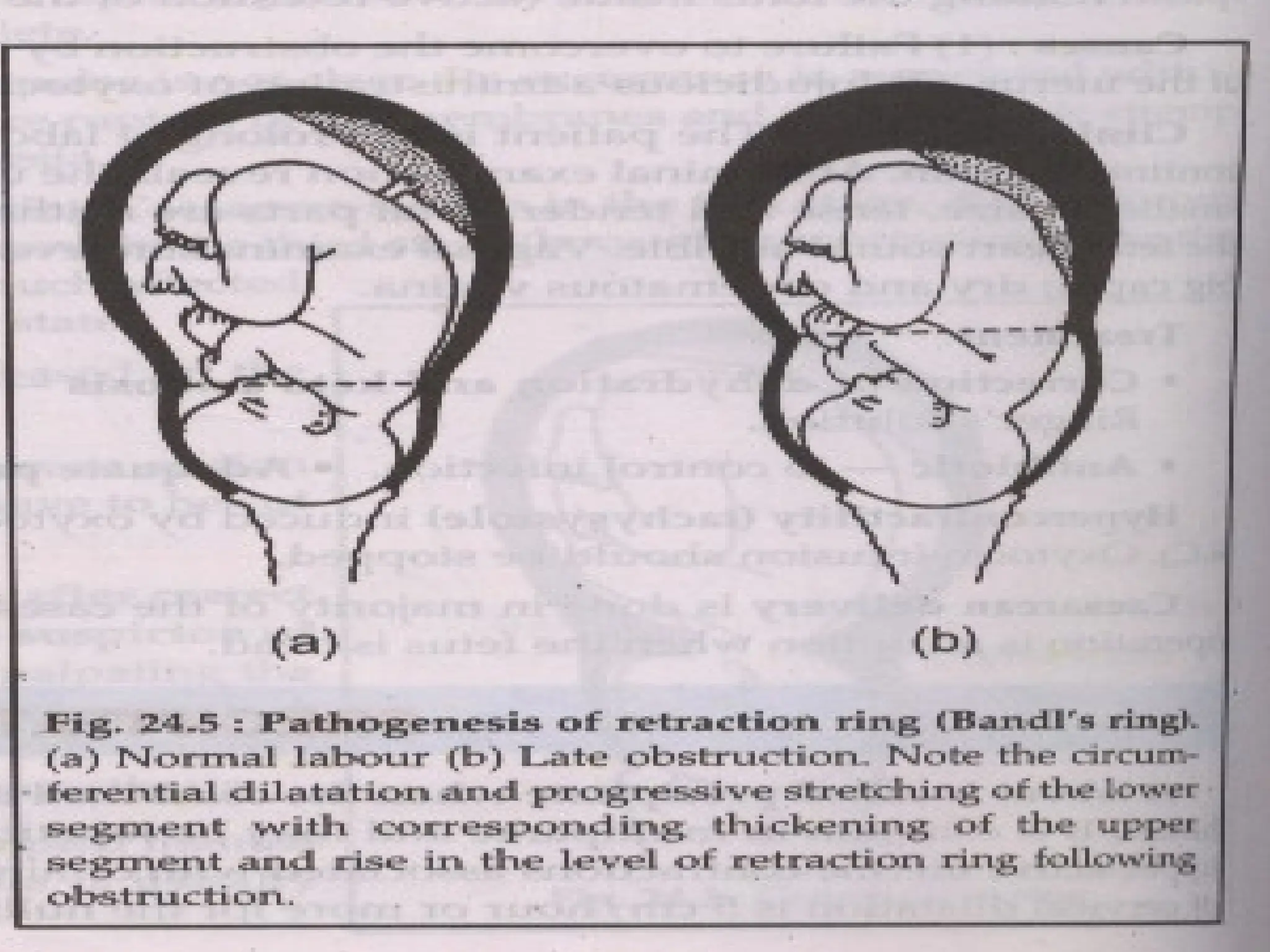
Pathological Retraction Ring (Bandl’s ring)
It is the rising up retraction ring during obstructed labour due to marked
retraction and thickening of the upper uterine segment while the relatively
passive lower segment is markedly stretched and thinned to accommodate
the foetus.
The Bandl’s ring is seen and felt abdominally as a transverse groove that
may rise to or above the umbilicus.
Clinical picture: is that of obstructed labour with impending rupture
uterus.
Obstructed labour should be properly treated otherwise the thinned lower
uterine segment will rupture.
48.
HYPOTONIC UTERINE INERTIA
Definition:The uterine contractions are infrequent, weak and of
short duration
General factors:
Primigravida particularly elderly.
Anaemia
Nervous and emotional as anxiety
and fear.
Hormonal due to deficient
prostaglandins or oxytocin as in
induced labour.
Improper use of analgesics.
Local factors:
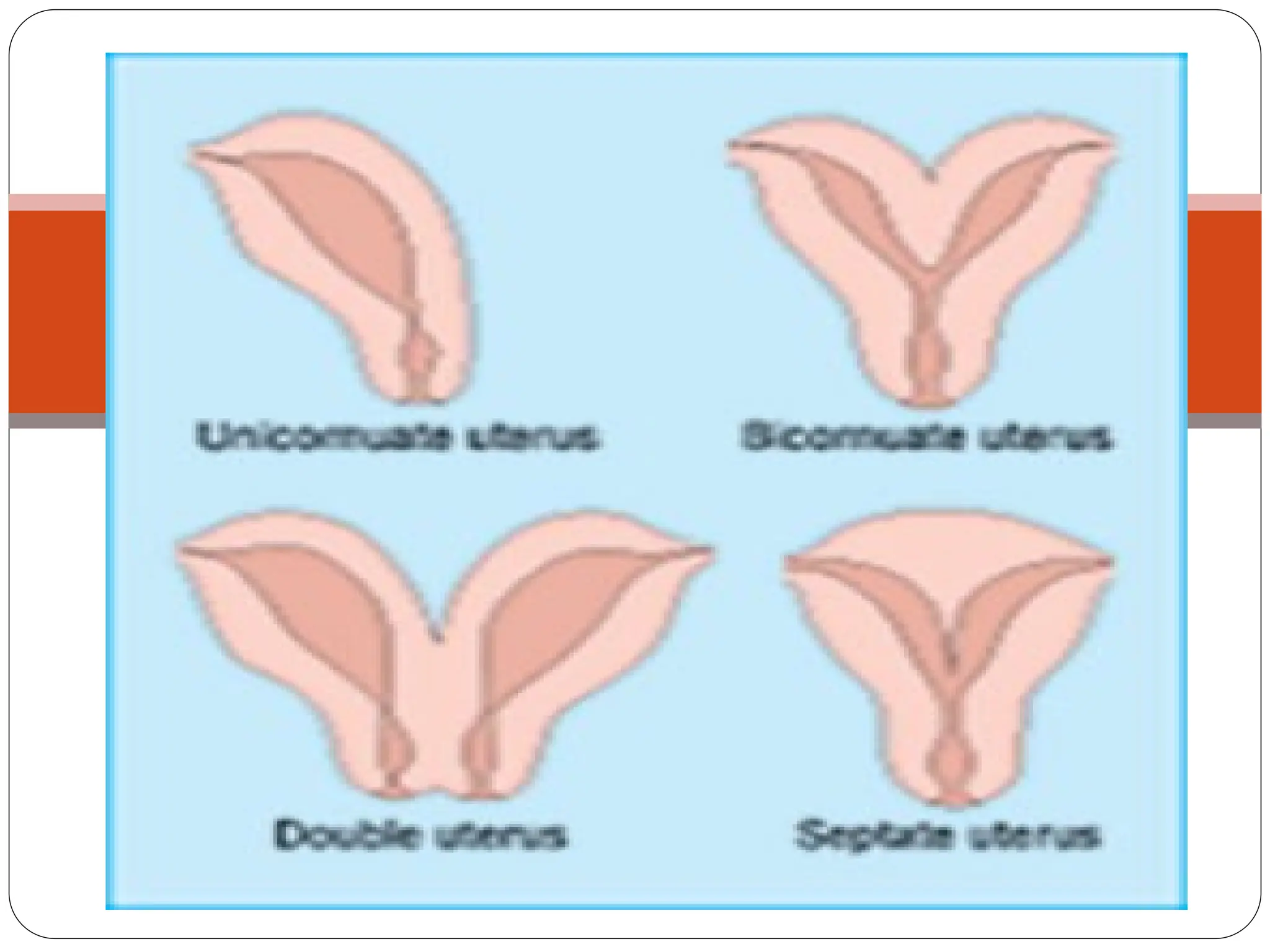
Overdistension of the uterus.
Developmental anomalies of the uterus
Myomas of the uterus interfering
mechanically with contractions.
Malpresentations, malpositions and
cephalopelvic disproportion. The
presenting part is not fitting in the
lower uterine segment leading to
absence of reflex uterine contractions.
Full bladder and rectum
49.
Types
Primary inertia: weakuterine contractions from the start.
Secondary inertia: inertia developed after a period of good uterine
contractions when it failed to overcome an obstruction so the uterus is
exhausted.
Clinical Picture
Labour is prolonged.
Uterine contractions are infrequent, weak and of short duration.
Slow cervical dilatation.
Membranes are usually intact.
The foetus and mother are usually not affected apart from maternal anxiety
due to prolonged labour.
More susceptibility for retained placenta and postpartum haemorrhage due to
persistent inertia.
Tocography: shows infrequent waves of contractions with low amplitude
HYPERTONIC UTERINE INERTIA
Types
Colickyuterus: incoordination of the different parts of the uterus in contractions.
Hyperactive lower uterine segment: so the dominance of the upper segment is lost.
Clinical Picture
The condition is more common in primigravidae and characterized by:
Labour is prolonged.
Uterine contractions are irregular and more painful.
High resting intrauterine pressure in between uterine contractions detected by
tocography (normal value is 5-10 mm of Hg).
Slow cervical dilatation.
Premature rupture of membranes.
Foetal and maternal distress.
52.
Management
General measures:as hypotonic inertia.
Medical measures:
€ Analgesic and antispasmodic as pethidine.
€ Epidural analgesia may be of good benefit.
Caesarean section is indicated in:
€ Failure of the previous methods.
€ Disproportion.
€ Foetal distress before full cervical dilatation
53.
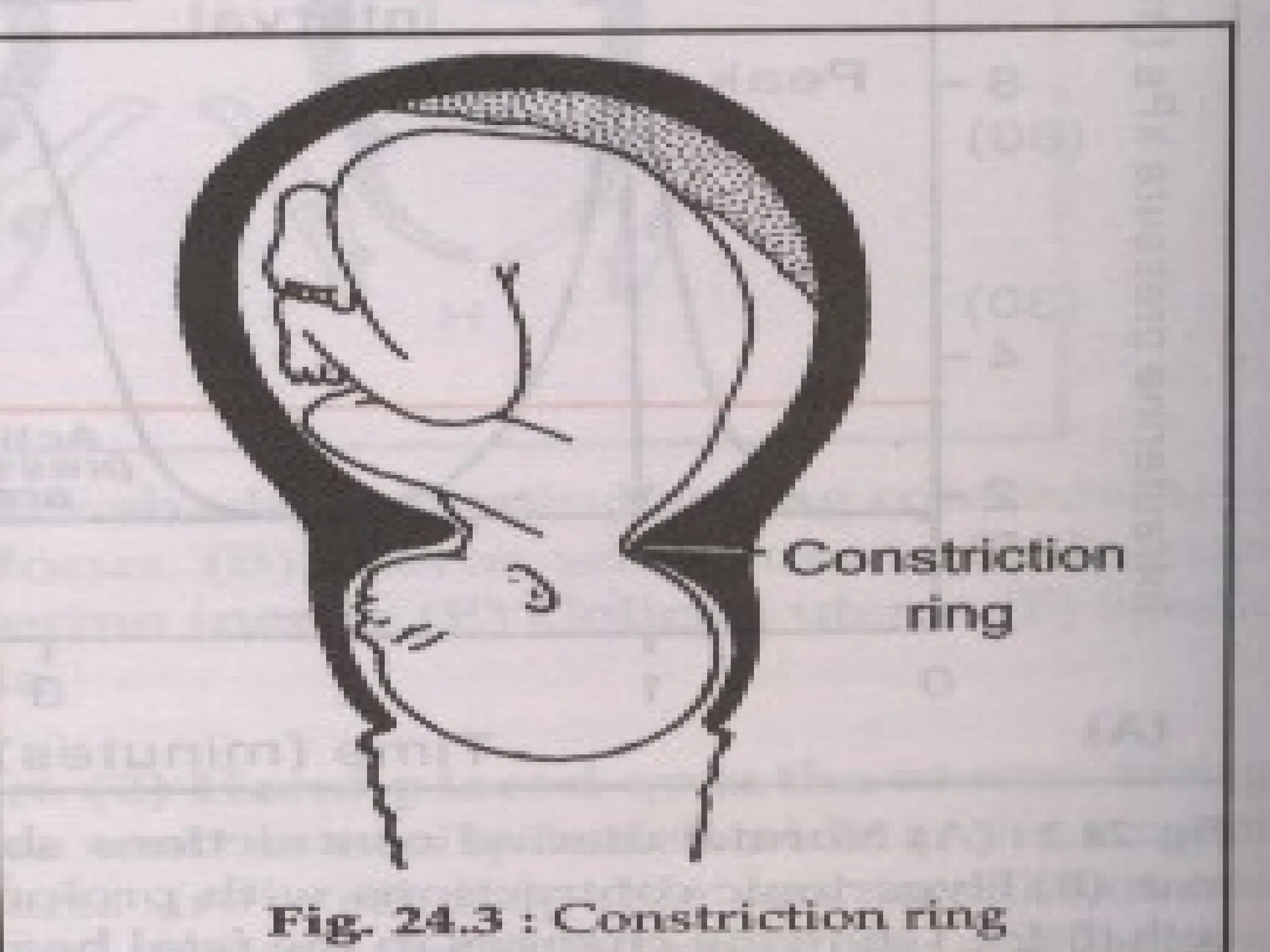
CONSTRICTION (CONTRACTION) RING
Definition
It is a persistent localised annular spasm of the circular uterine muscles.
It occurs at any part of the uterus but usually at junction of the upper and
lower uterine segments.
It can occur at the 1st, 2nd or 3rd stage of labour.
55.
Aetiology
Unknown but thepredisposing factors are:
Malpresentations and malpositions.
Clumsy intrauterine manipulations under light anaesthesia.
Improper use of oxytocin e.g.
use of oxytocin in hypertonic inertia.
IM injection of oxytocin.
Diagnosis
The condition is more common in primigravidae and frequently
preceded by colicky uterus.
The exact diagnosis is achieved only by feeling the ring with a
hand introduced into the uterine cavity.
56.
Management
Exclude malpresentations, malpositionand disproportion.
In the 1st stage: Pethidine may be of benefit.
In the 2nd stage: Deep general anaesthesia is given to relax the
constriction ring:
If the ring is relaxed, the foetus is delivered immediately by forceps.
If the ring does not relax, caesarean section is carried out with lower
segment vertical incision to divide the ring.
In the 3rd stage: Deep general anaesthesia is given followed by
manual removal of the placenta
57.
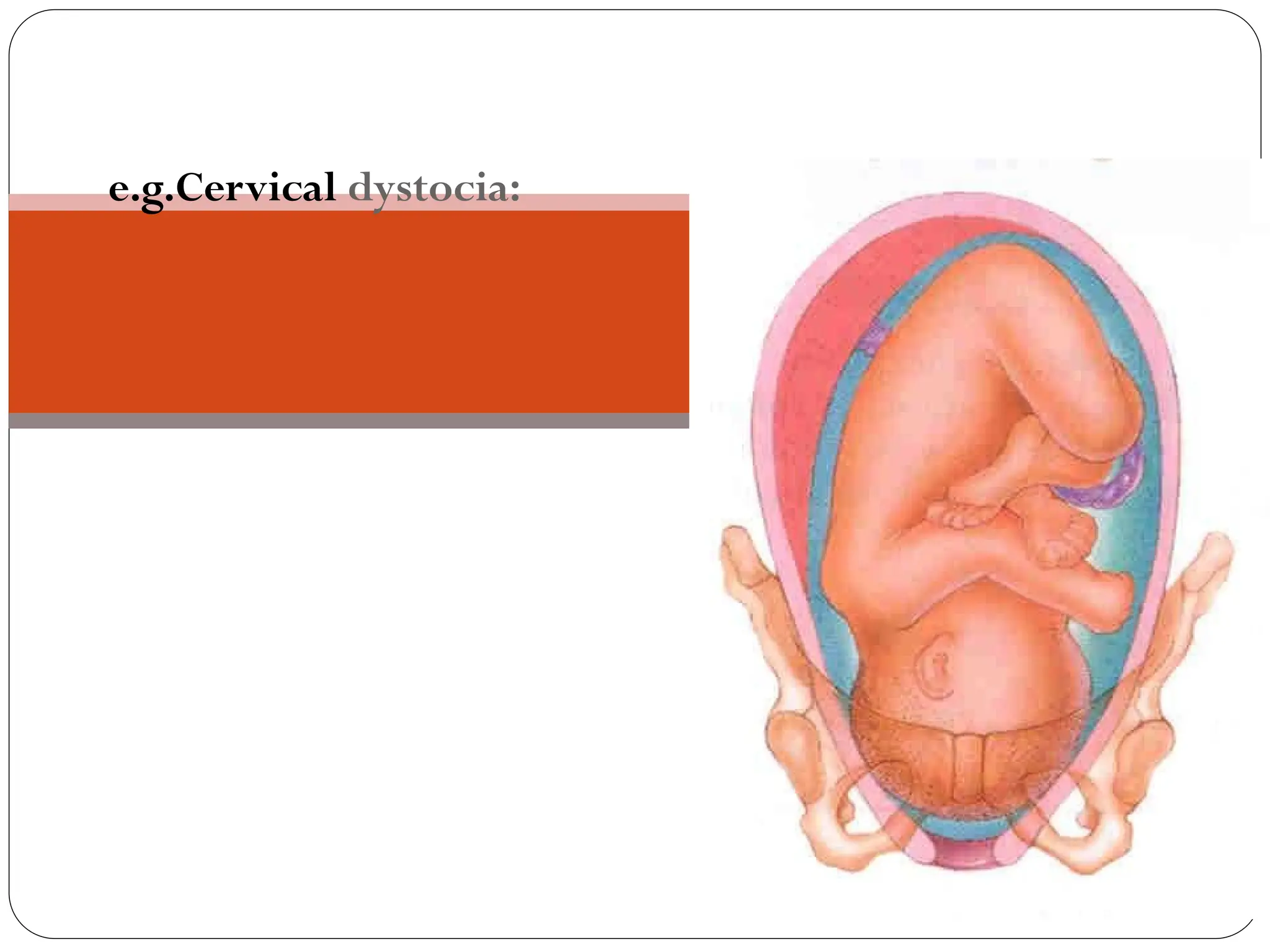
CERVICAL DYSTOCIA
Definition
Failure ofthe cervix to dilate within a reasonable time in spite of good
regular uterine contractions.
Varieties
Organic (secondary) due to
Cervical stances as a sequel to previous amputation, cone biopsy, extensive
cauterisation or obstetric trauma.
Organic lesions as cervical myoma or carcinoma.
Functional (primary):
In spite of the absence of any organic lesion and the well effacement of the
cervix, the external os fails to dilate.
This may be due to lack of softening of the cervix during pregnancy or
cervical spasm resulted from overactive sympathetic tone.
58.
Complications
Annular detachment ofthe cervix: the bleeding from the cervix is
minimal because of fibrosis and avascular pressure necrosis leading
to thrombosis of the vessels before detachment.
Rupture uterus.
Postpartum haemorrhage: particularly if cervical laceration extends
upwards tearing the main uterine vessels.
Management
Organic dystocia:
♣ Caesarean section is the management of choice.
Functional dystocia:
♣ Pethidine and antispasmodics: may be effective.
♣ Caesarean section: if
♣ medical treatment fails or
♣ foetal distress developed.
Definition
The labour isprolonged when the combined duration of the
first and second stage is more than the arbitrary time limit
of 18 hours.
[ D.C.Dutta]
Prolonged labour is defined when the first and second
stage of labour last more than 24 hours, currently duration
is taken as more than 18 hours. Duration of labour is
calculated from mother’s subjective estimate of labour
onset
[Dawn]
63.
Prolongation due to
Protracted cervical dilatation in the first stage
Inadequate descent of the presenting part during the first or
in the second stage
Labour considered prolonged when the cervical dilatation
rate is < 1 cm/hr and the descent of the presenting part is <
1 cm/hr for a period of minimum 4 hours observation.
64.
Types of prolongedlabour
Hypotonic uterine dysfunction: due to low intensity
uterine contractions.
general factors local factors
Elderly primi gravida over distention of uterus
Anemia developmental anomalies
Nervousness, anxiety myomas of uterus
and fear
Hormonal mal presentations, CPD
Improper use of malpositions
analgesics full bladder and rectum
65.
Cont…
Hypertonic uterinedysfunction: it can be
a. Incordinate uterine action
b. colicky uterus
c. Asymmetrical uterine dysfunction
d. Hyperactive lower segment
e. Constriction ring dystocia
Cervical dystocia: cervix becomes thin and fails to dilate
within a reasonable time inspite of good uterine
contractions.
Risk factors ofprolonged labour
age and parity: commonly primigravidae, more in elderly
one
CPD and fetal malposition
Uterine distention- twins, hydramnios
Uterine defect- fibroid, malformation
Nervousness, fear and emotion
injudicious use of analgesia in labour
injudicious induction of labour by ARM and oxytocin
drip.
unknown cause.
69.
Causes of prolongedlabour
Faults in power [commonest cause]
*inefficient uterine dysfunction
*constriction ring
*cervical dystocia
*over dose of sedative and analgesics
* epidural analgesia
*improper use of oxytocics
70.
Cont…
Faults in passage:
PROM
Contracted pelvis
CPD
Cervical stenosis
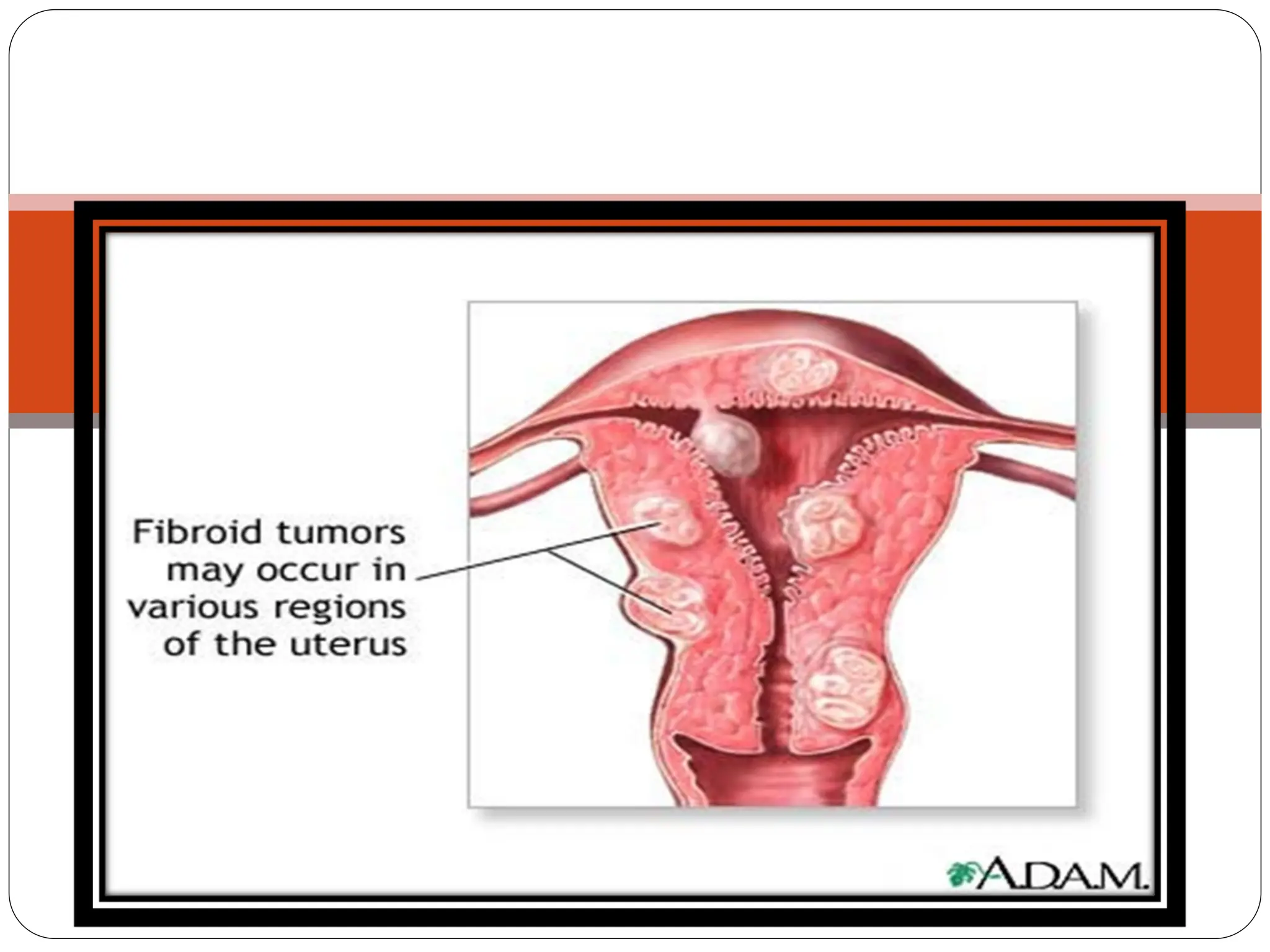
Fibroid or carcinoma
Ovarian tumor
Uterine fibroid 20%
71.
Engagement & descentof the
foetal head -
presence of cephalopelvic
disproportion
72.
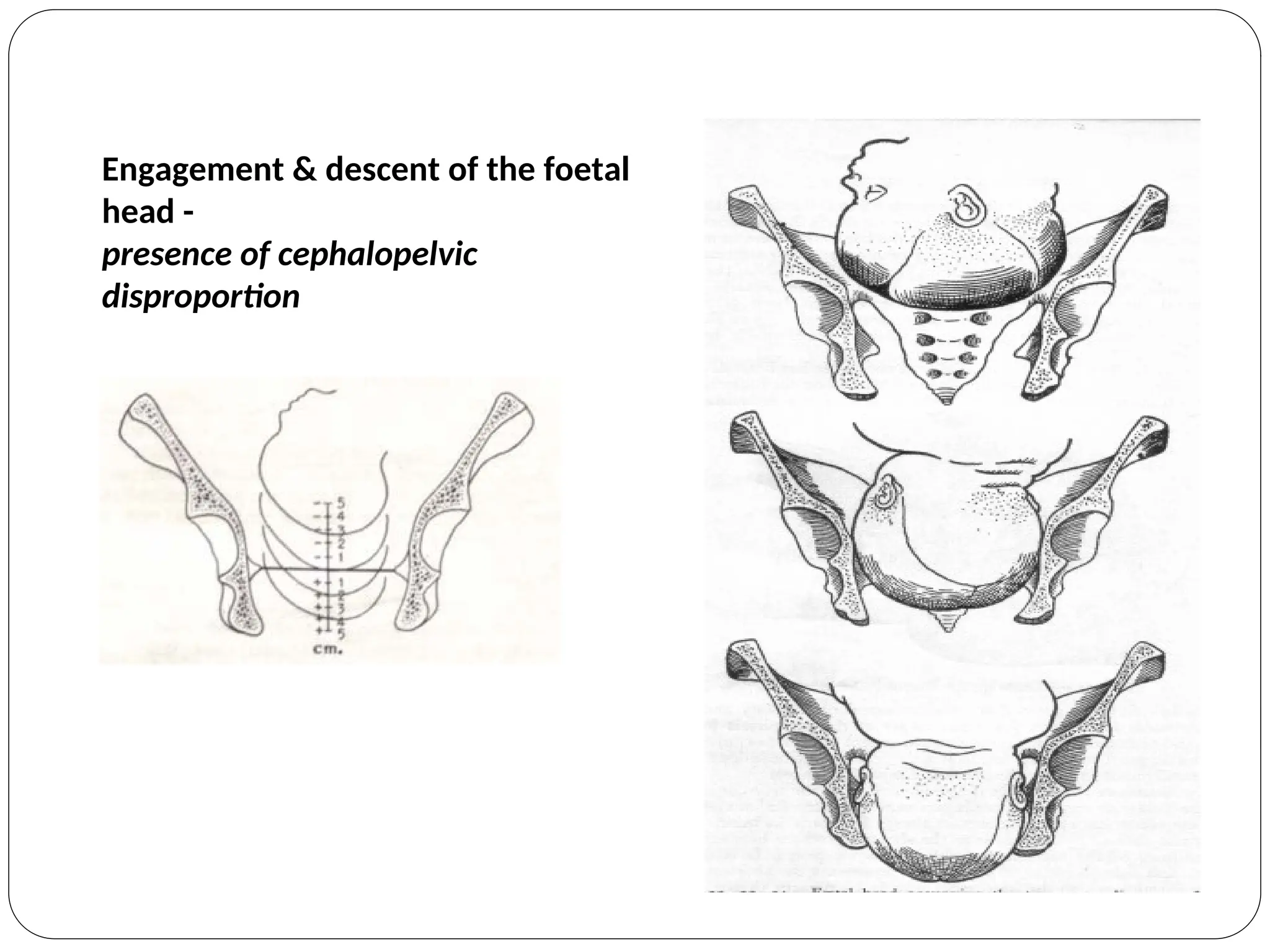
Engagement & descentof the foetal
head -
presence of cephalopelvic
disproportion
Labour disorders dueto inefficient
uterine action
prolonged latent phase beyond 12 hours
a. Hypotonic or hypertonic dysfunction
b. Predisposing factors are sedation, anaesthesia , false
labour,unknown cause.
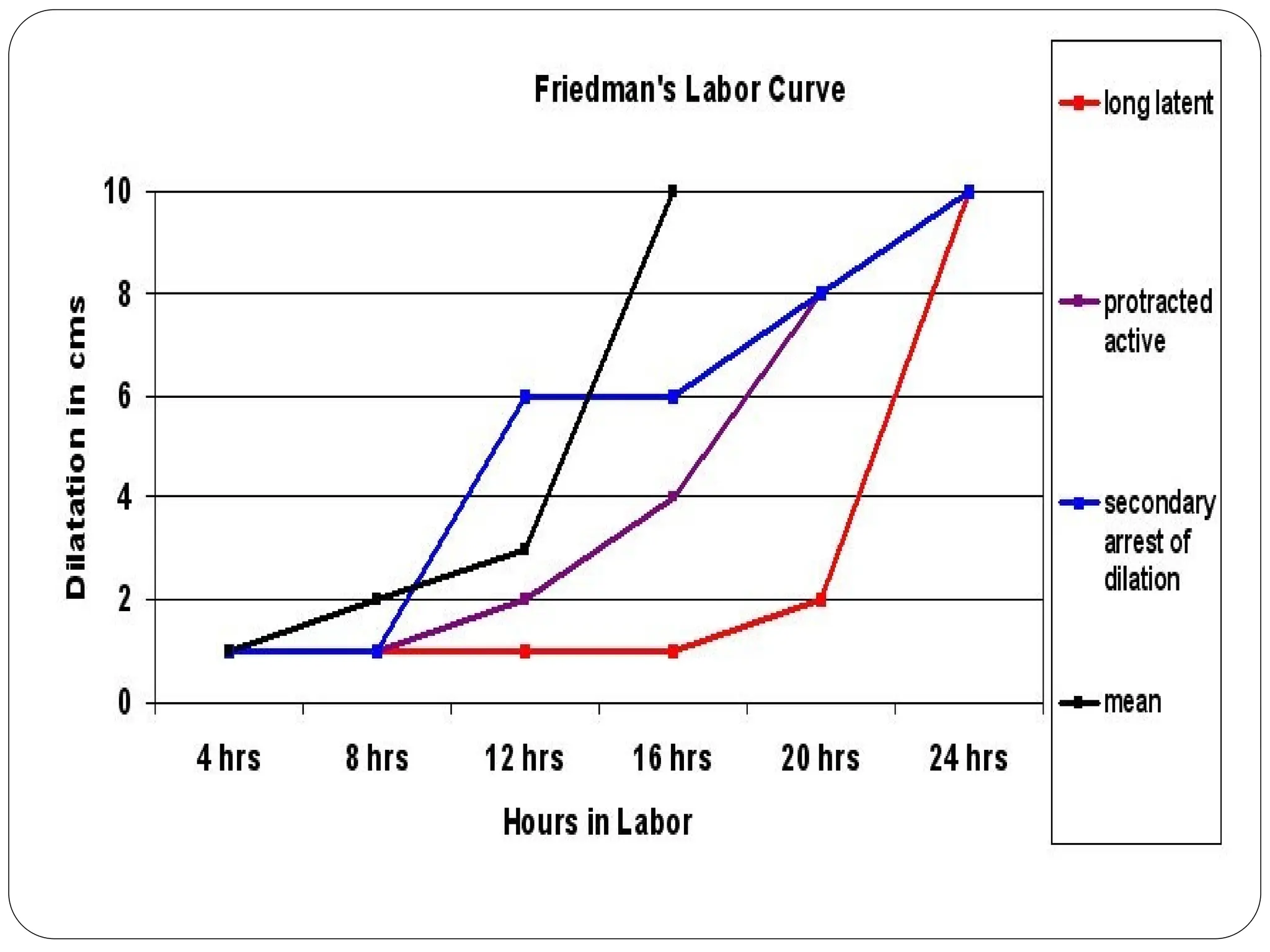
Prolonged active phase[ protraction disorder]
Slow rate of cervical dilatation below 1cm/hr in
nullipara and 1.5 cm/hr in multipara
Caused by hypotonic dysfunction, hyperactive lower
segment.
Predisposing factors :CPD,fetal malpositions and
sedation
75.
Cont…
secondary arrest ofcervical dilatation or head descent
Arrest of cervical dilatation is taken when there is no
cervical change for 2 hrs.
there is head descent less than 1cm/hr in nullipara or
less than 2cm/hr in multipara and no head descent for
one hour.
Due to hypotonic dysfunction and incordinate uterine
dysfunction.
The causative factors are occipito posterior positions
[70%], pelvic contraction ,excessive sedation.
76.
DIAGNOSIS
Clinical features
Hypotonic
dysfunction
[more frequent]
Hypertonic
dysfunction
[less frequent]
1. Timing of
dysfunction
[more
frequent]
At latent phase
from start of labour
usually running to
active phase
Latent phase from start of
labour
2.Labour pains Less painful, short
lasting,
infrequent
abdominal pain
and no back ache
Severely painful ,prolonged
lasting, frequent pain as
abdominal colic or as
backache ,desire to bear
down during contraction
with incompletely dilated
cervix.
77.
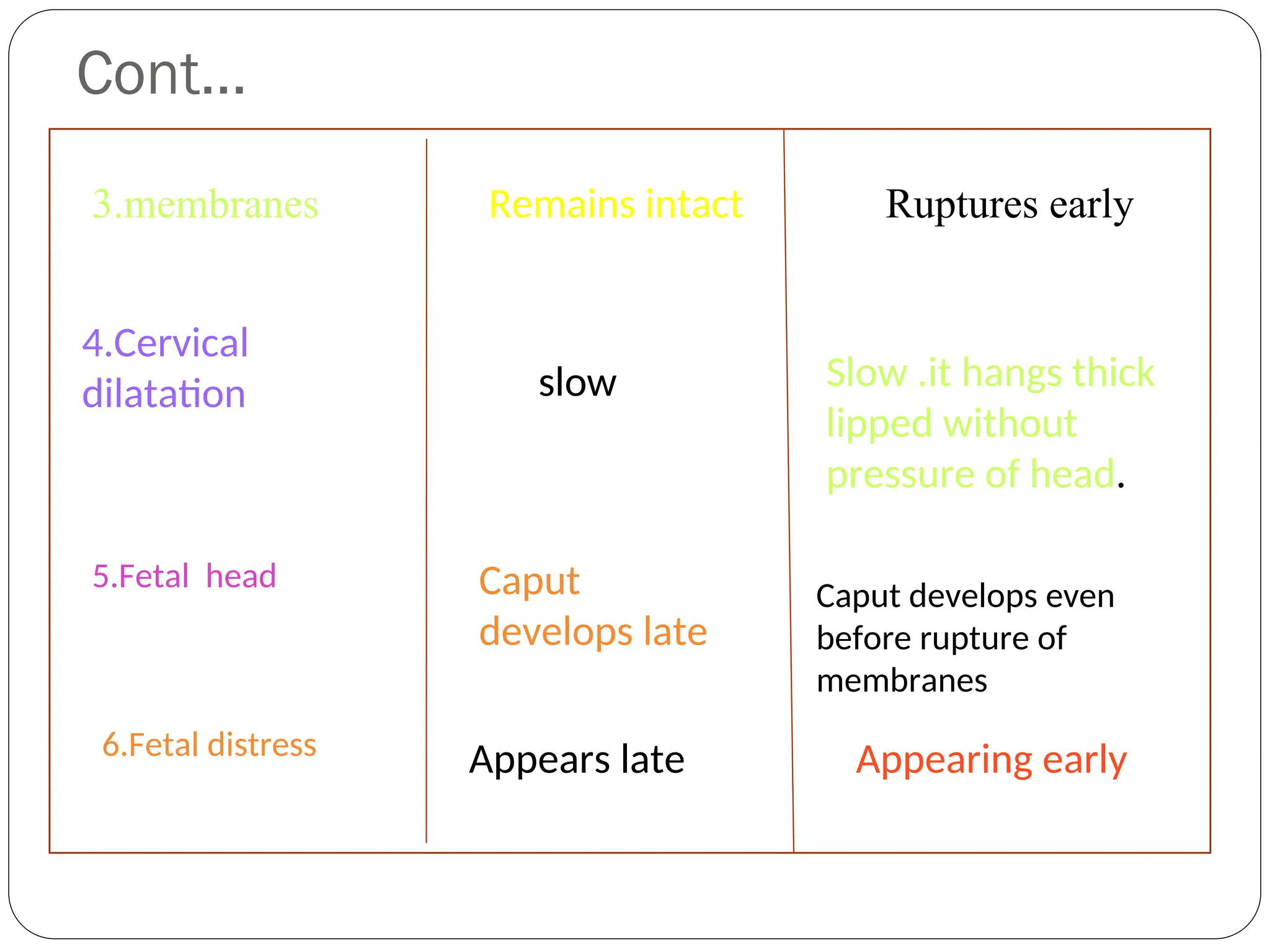
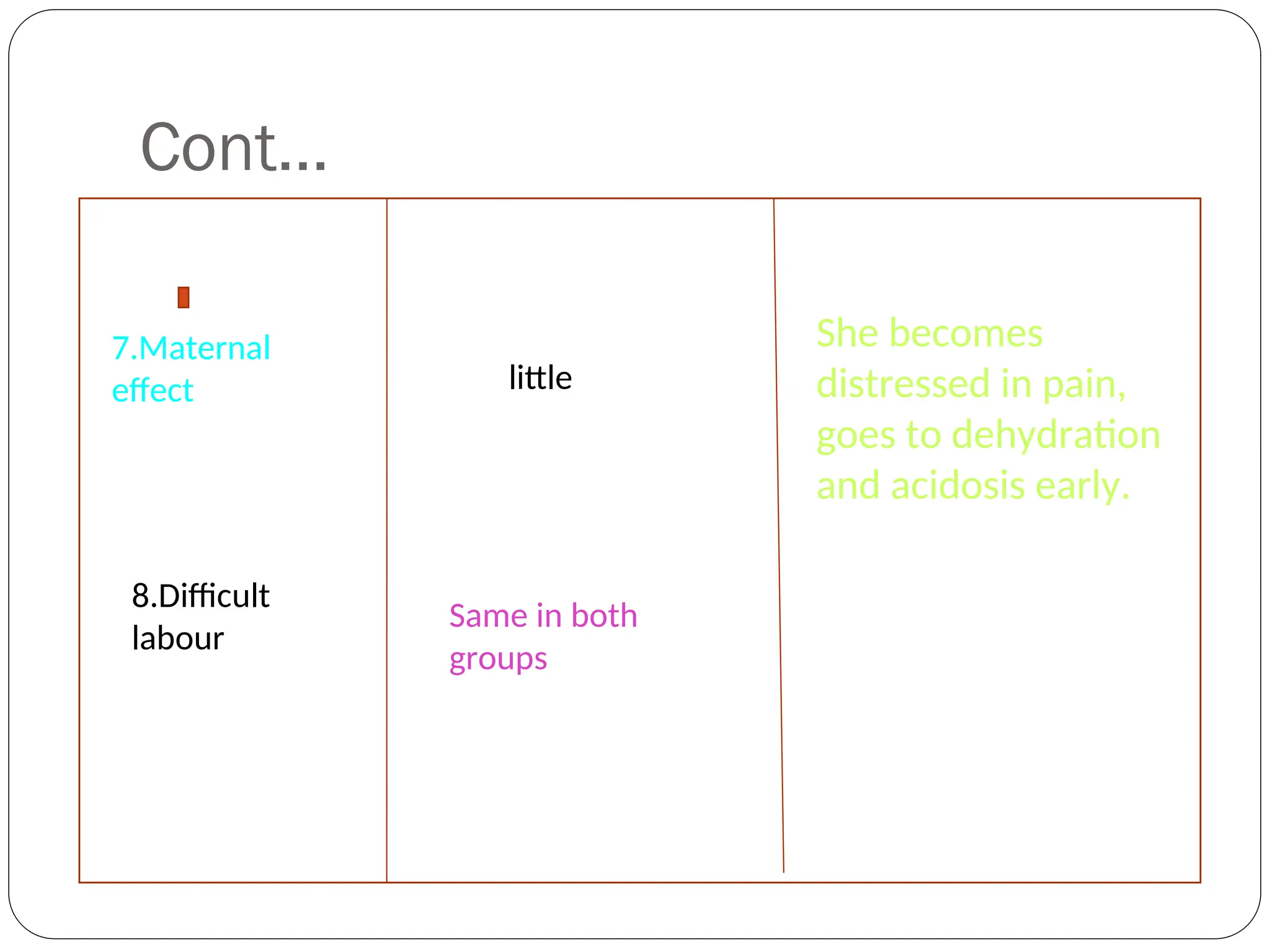
Cont…
3.membranes Remains intactRuptures early
4.Cervical
dilatation slow Slow .it hangs thick
lipped without
pressure of head.
5.Fetal head Caput
develops late
Caput develops even
before rupture of
membranes
6.Fetal distress Appears late Appearing early
Cont…
Other measures suchas :
radiography, CT or MRI
Abdominal and vaginal examination.
partograph
80.
Cont…
First stage: isconsidered prolonged
When the duration of labour is more than 12 hrs
The rate of cervical dilatation is < 1 cm / hr in a primi and
< 1.5 cm/ hr in a multi
when the cervicograph crosses the alert line and falls on
zone2
Intervention is required when the cervico graph crosses
the action line and falls on zone 3
81.
Cont…
Secondary arrest :is defined when the active phase of
labour ( cervical dilatation ) commences normally but
stops or slows significantly for 2 hrs or more prior to
full dilatation of the cervix. It is commonly due to
malposition or CPD
84.
Cont…
Second stage: isconsidered prolonged
When it lasts for more than 2 hrs in primi and 1 hr in
multi.
Diagnosis :
Sluggish or non descent of the presenting part even
after full dilatation of the cervix.( failure of head
descent within 1 hr of full dilatation is called
protraction of descent.)
Variable degrees of molding and caput formation in
cephalic presentation.
Identification of the course of prolongation.
Management
Prevention :
Antenatal orearly intra natal detection of the factors
likely to produce prolonged labour.
Use of partograph
Selection and judicious augmentation of labour by
low rupture of the membranes followed by oxytocin
drip.
Change of posture in labour, other than supine to
increase uterine contractions, avoidance of
dehydration in labour and use of adequate analgesia
for pain relief.
Cont…
Definitive Rx :
Firststage
patient is referred to level 11 care without any solid food.
Only water is allowed orally.
Maintain partograph
Identify or diagnosis of hypotonic and hypertonic labour
dysfunction.
Monitor maternal vital signs and FHS
Identify CPD or fetal mal position.
Maintain I.V line with 5% DW/RL
Antibiotics ( cefazoline ) 1 gm I.V and repeated after 6 hrs on
PROM
90.
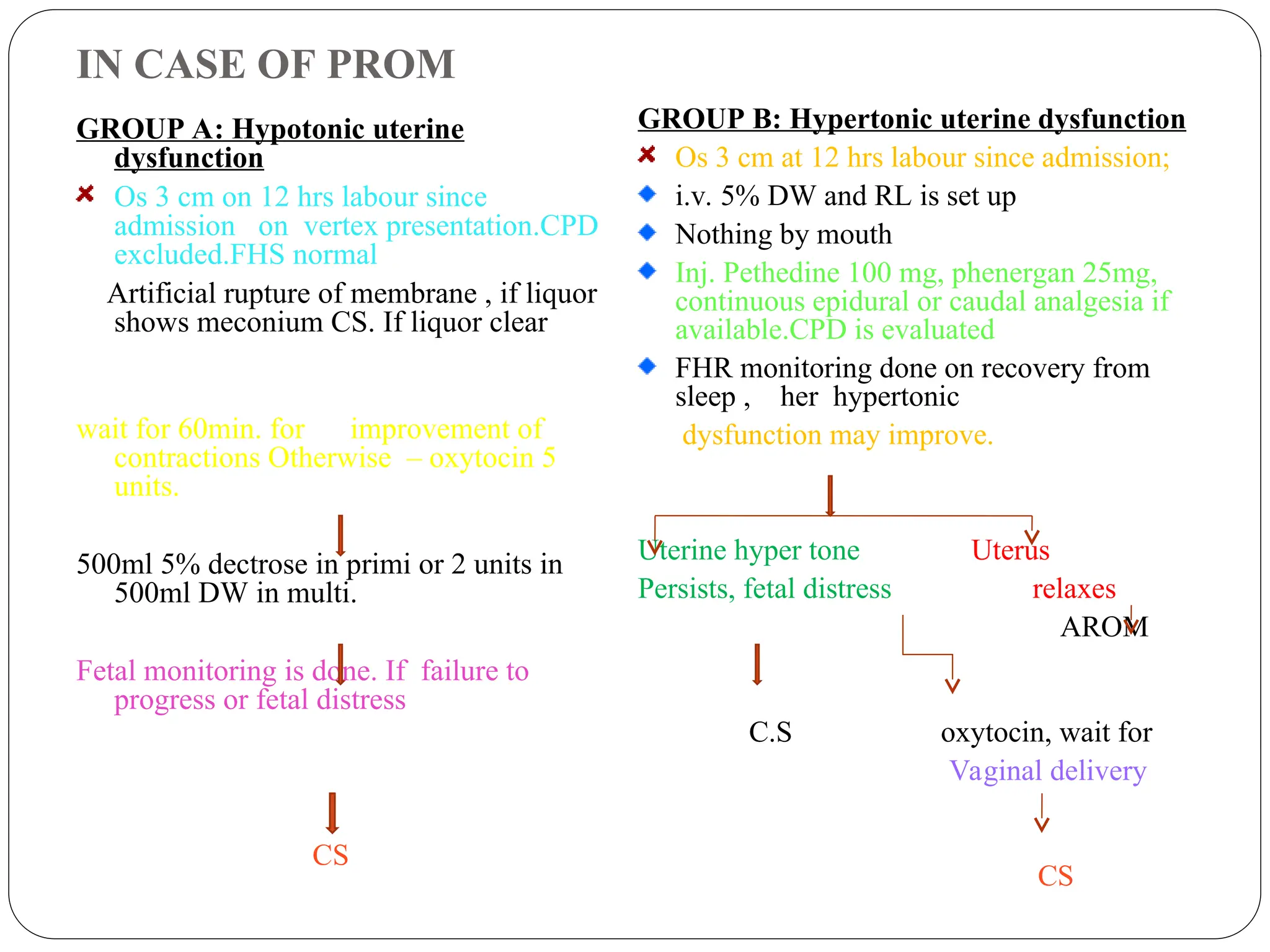
IN CASE OFPROM
GROUP A: Hypotonic uterine
dysfunction
Os 3 cm on 12 hrs labour since
admission on vertex presentation.CPD
excluded.FHS normal
Artificial rupture of membrane , if liquor
shows meconium CS. If liquor clear
wait for 60min. for improvement of
contractions Otherwise – oxytocin 5
units.
500ml 5% dectrose in primi or 2 units in
500ml DW in multi.
Fetal monitoring is done. If failure to
progress or fetal distress
CS
GROUP B: Hypertonic uterine dysfunction
Os 3 cm at 12 hrs labour since admission;
i.v. 5% DW and RL is set up
Nothing by mouth
Inj. Pethedine 100 mg, phenergan 25mg,
continuous epidural or caudal analgesia if
available.CPD is evaluated
FHR monitoring done on recovery from
sleep , her hypertonic
dysfunction may improve.
Uterine hyper tone Uterus
Persists, fetal distress relaxes
AROM
C.S oxytocin, wait for
Vaginal delivery
CS
91.
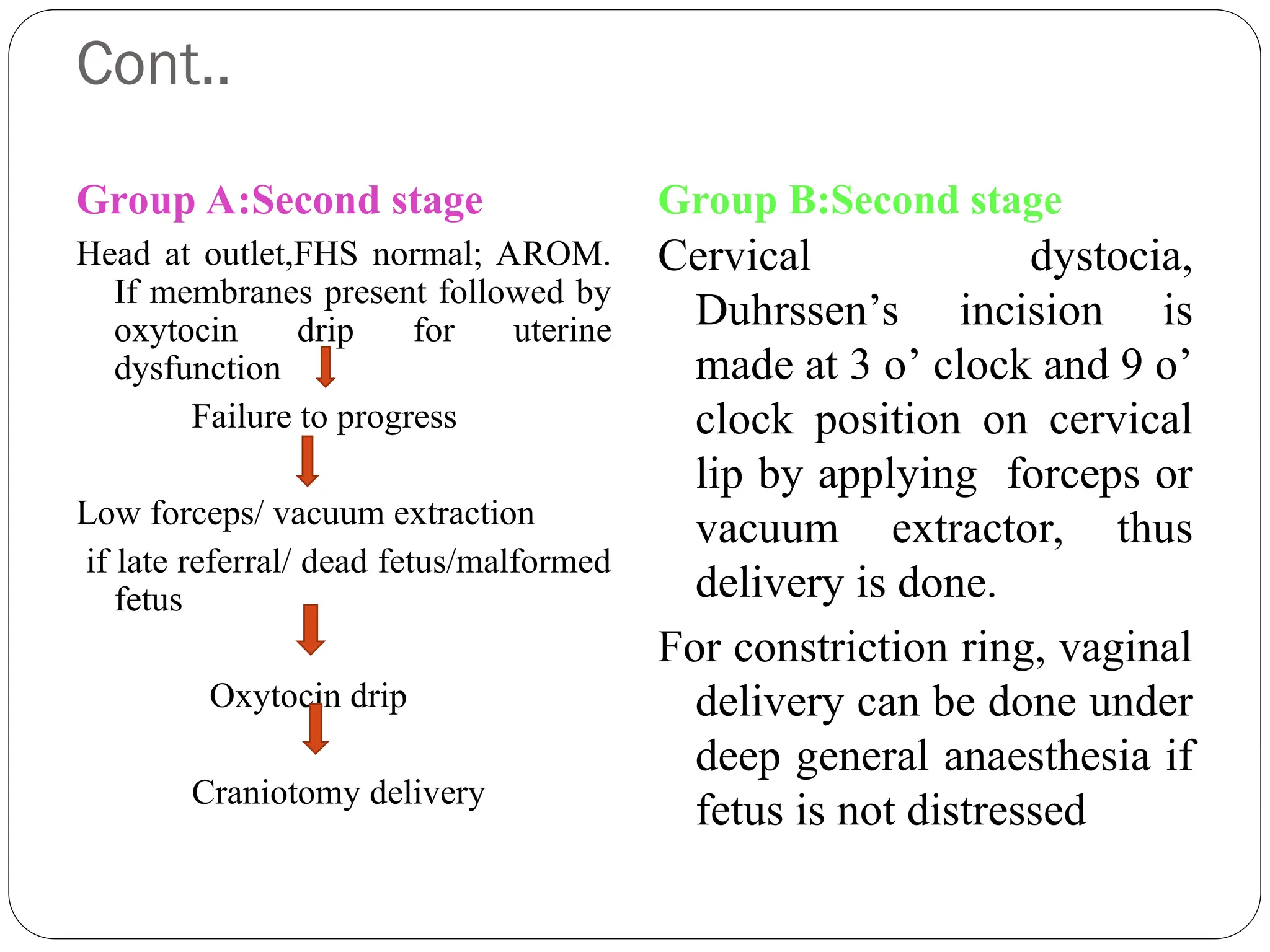
Cont..
Group A:Second stage
Headat outlet,FHS normal; AROM.
If membranes present followed by
oxytocin drip for uterine
dysfunction
Failure to progress
Low forceps/ vacuum extraction
if late referral/ dead fetus/malformed
fetus
Oxytocin drip
Craniotomy delivery
Group B:Second stage
Cervical dystocia,
Duhrssen’s incision is
made at 3 o’ clock and 9 o’
clock position on cervical
lip by applying forceps or
vacuum extractor, thus
delivery is done.
For constriction ring, vaginal
delivery can be done under
deep general anaesthesia if
fetus is not distressed
92.
Cont…
Third stageactively managed
Neonatal care is important due to meconium aspiration
93.
Nursing diagnosis
Riskfor injury to mother and fetus
Fatigue and exhaustion related prolonged efforts and
pain
Anxiety related to process and outcome of labour
Knowledge deficit related to labour process
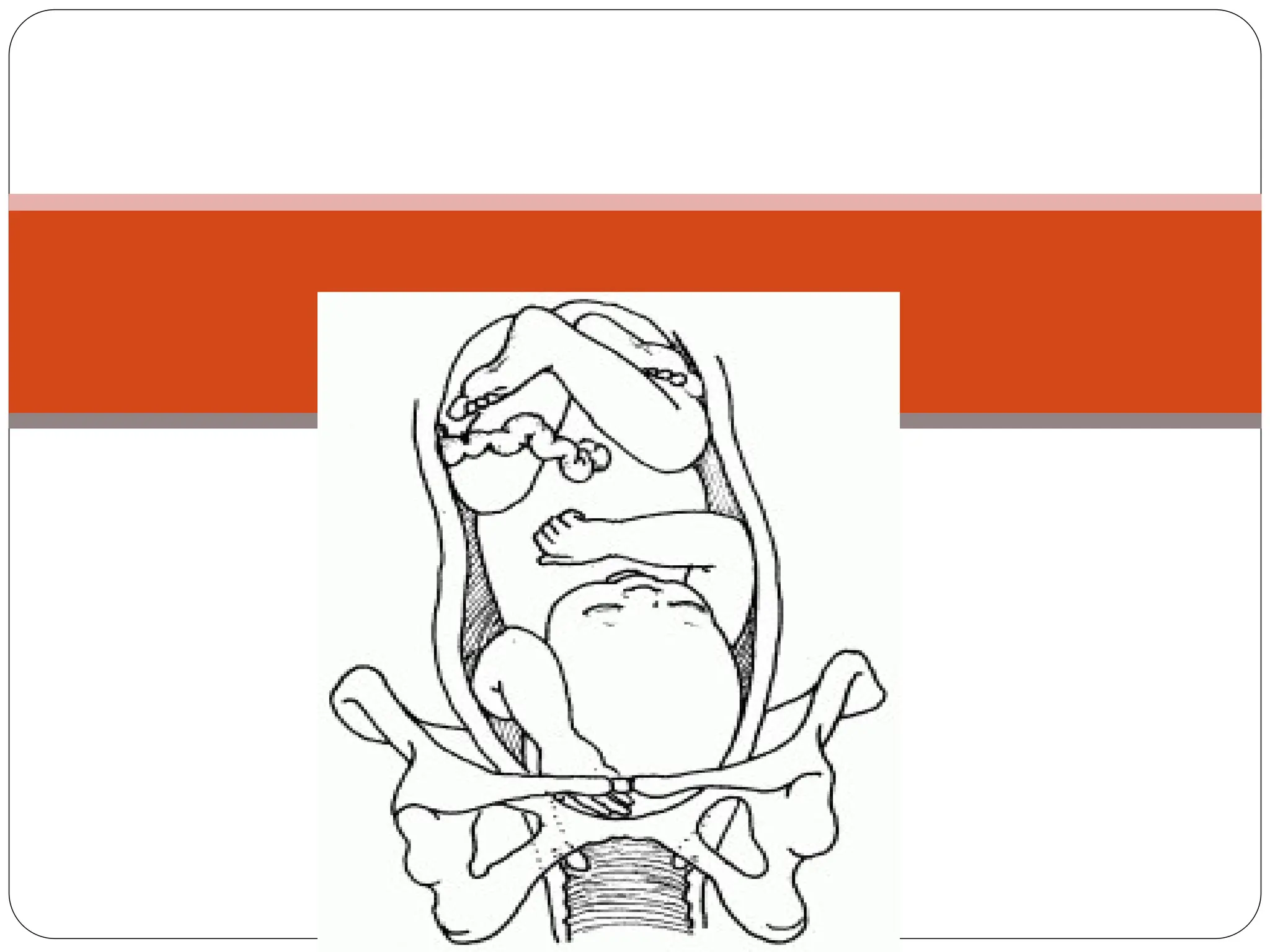
SIGNS OF OBSTRUCTEDLABOUR.
EARLY SIGNS:
PRESENTING PART DOES NOT ENTERTHE PELVIC
BRIM.
SLOW CERVICAL DILATATION.
LOOSELY HANGING CERVIX.
EARLY RUPTURE OF MEMBRANE OR FORMATION
OF A LARGE ELONGATED SAC OF FOREWATERS.
120.
LATE SIGNS:
I. MOTHERMAY BE DEHYDRATED AND KETOTIC AND IN
CONSTANT PAIN.
II. CLINICAL SIGNS:-
a) PYREXIA,TACHYCARDIA.
b) DIFFICULT ABDOMINAL PALPATION.
c) DIFFICULT ABDOMINAL EXAMINATION.
d) COMPLICATEDVAGINAL EXAMINATION.
121.
CONTI…
e) LESS URINEOUTPUT,HAEMATURIA.
f) EVIDENCE OF FETAL DISTRESS.
g) PHYSIOLOGIC RETRACTION RING.
h) VISIBLE RETRACTION RING OR BANDL’S RING.
i) HOT,DRYVAGINA.
j) PRESENTING PARTWILL BE HIGH AND
IMMOVABLE.
DEFINITION
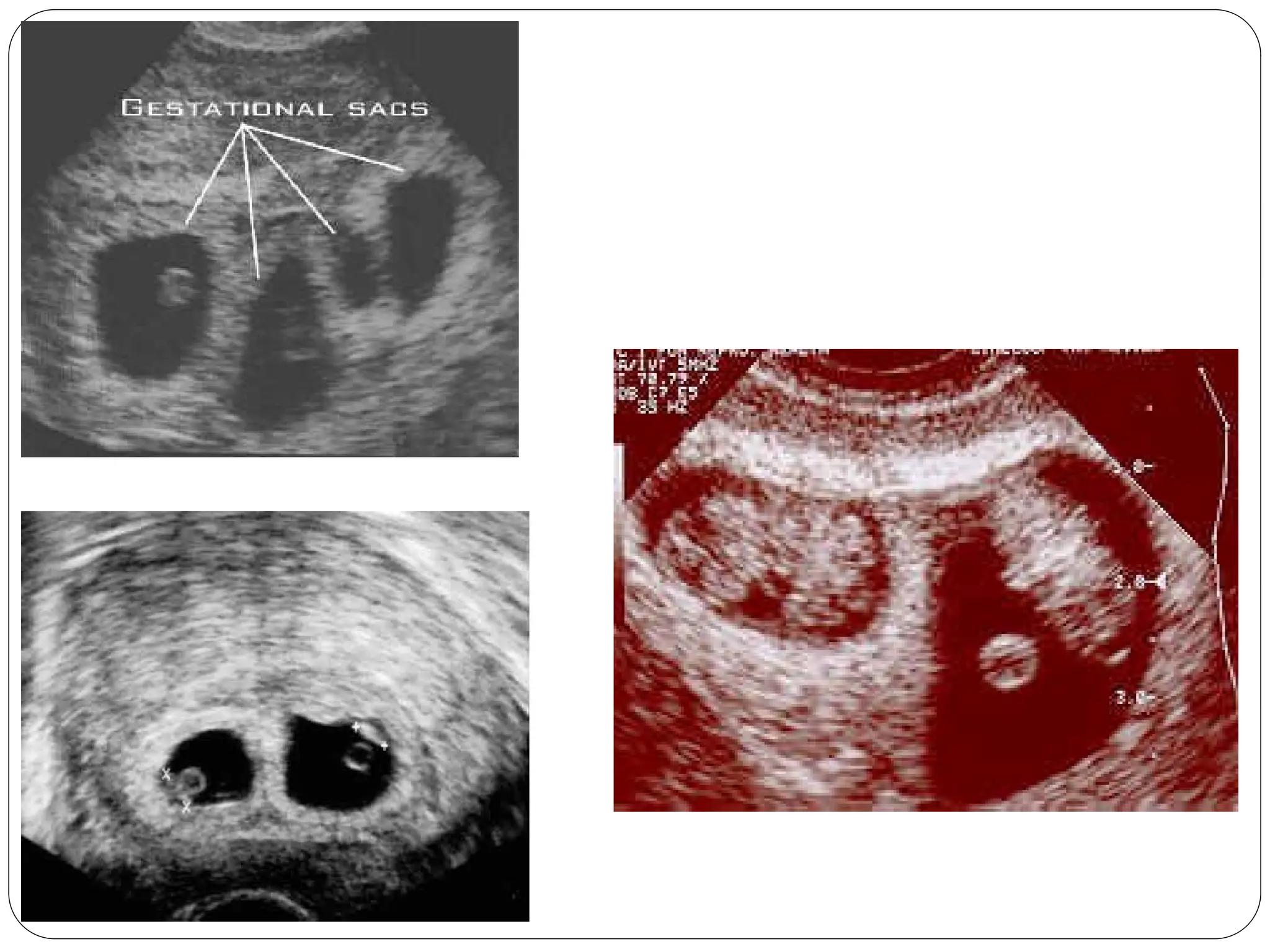
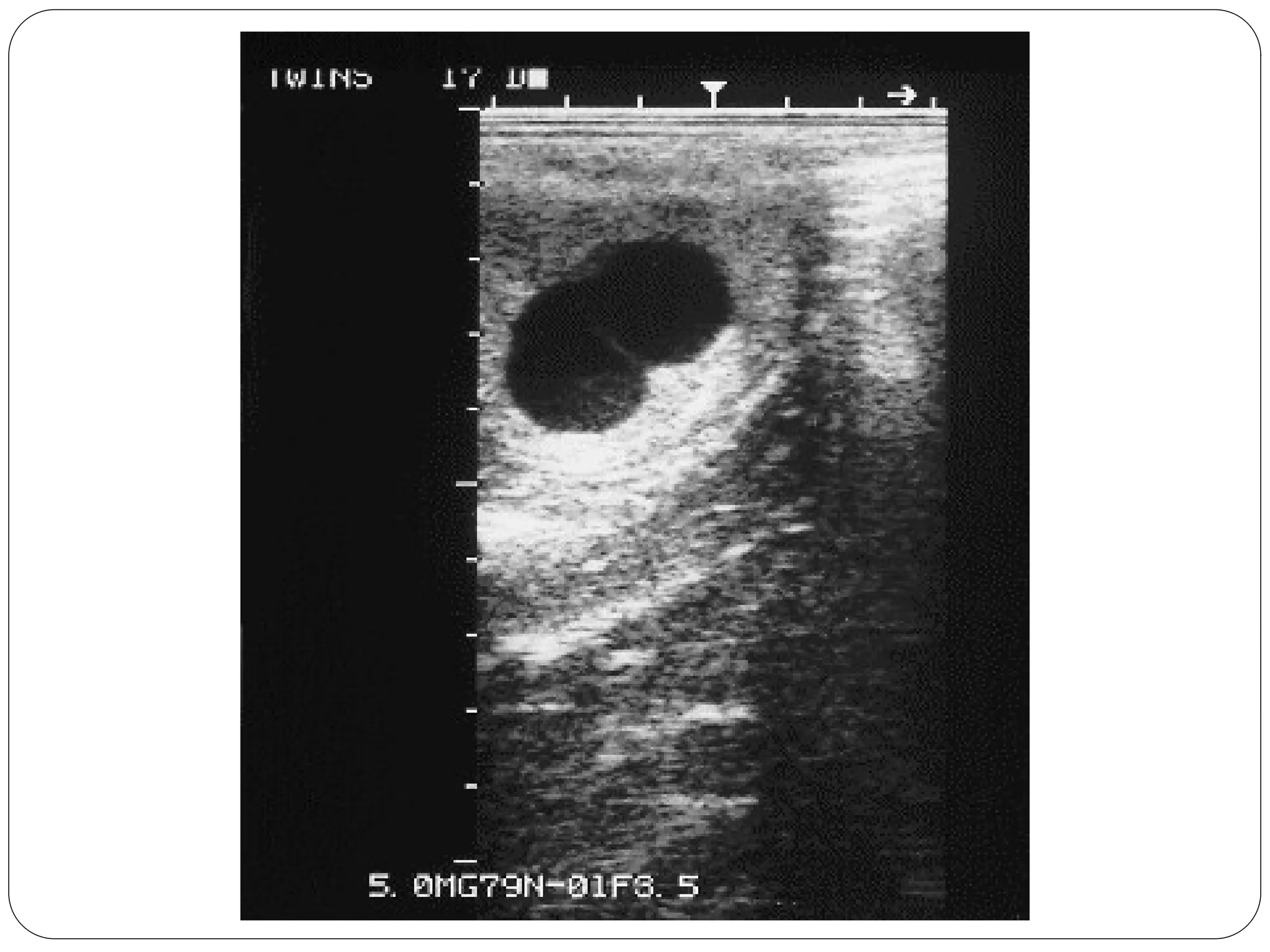
When more thanone fetus
simultaneously develops in the
uterus ,it is called multiple
pregnancy.
124.
According to theirnumber, they could be
categorized into:
Twins (most common)
Triplets
Quadruplets
Quintuplets
Sextuplets
125.
Types
Monozygotic
Identical/Uniovular
Fertilization of a single ovum,
Similar sex.
Identical in every way including
the HLA genes
Not genetically determined
Dizygotic
Fertilization of 2 seperate
ova
Fraternal /Dizygotic
126.
Monozygotic Twins…
Different Scenariosof Cleavage
If the separation takes place just after the first cellular
division [1st
3 days ]/ prior to morula stage
both of the twins will have their own placenta and an
amniotic sac each.
Scenario 1
Monozygotic twin pregnancy
Di-Amniotic and Di-Chorionic
or D/D
127.
Scenario 2
Monozygotic twinpregnancy
Di-amniotic - Mono-chorial
and or D/M
Separation can also take place a little
later in the development [4-8 days after
the formation of inner cell mass when
chorion has developed]
of the embryonic cells but before the
blastocyte has defined the roles of each
cell.
Twins will be in the same placenta, but
they will have 2 amniotic sacs.
128.
Scenario 3
Monozygotic twinpregnancy
Mono-amniotic and Mono-
chorial
Separation takes place at the stage when the amniotic bag is
already being formed
[day 8-14]
Twins will be in the same placenta, and in the same amniotic
129.
Conjoined Twins
Ifthe division occur after 2 weeks
of the embryonic disc formation,
incomplete or conjoined twins
will occur.
They may be joined
anteriorly [thoracopagus-
commonest],
posteriorly [pyopagus]
cephalic [craniopagus] o
caudal [ischiopagus].
130.
Dizygotic twin pregnancy
Di-chorialand Di-amniotic.
Dyzygotic twins, are descended from a double ovulation and a double fertilization.
The 2 eggs are completely independent.
This configuration represents two thirds of all twin pregnancies.
132.
Superfecundation
It is thefertilization of two different ova
released in the same menstrual cycle,by
separate act of coitus within a short period of
time.
133.
Superfetation
It is thefertilization of two ova released in
different menstrual cycle
One fetus over another
Possible until decidual space is obliterated by
12 weeks of pregnancy
134.
Fetus papyraceous orcompressus
One fetus dies early
Dead fetus is flattened and compressed
between the membranes of the living fetus
and the uterine wall
135.
Fetus acardicus
Occurs onlyin monozygotic twins
Part of the fetus remains amorphous and
becomes parasitic without a heart
Vanishing twins
USG inearly pregnancy revealed occassional
death of one fetus and continuation of
pregnancy with surviving one
138.
ETIOLOGY
Race –Highest among negroes and lowest among mongols
Hereditary- Transmitted through female
Advancing age of the mother- Maximum between 30-35 years
Parity – 5th
gravida onwards
Iatrogenic – Gonadotrophin(20-40%),clomephene citrate(5-
6%)
139.
Maternal physiological changes
Increaseweight gain and cardiac out put
Plasma volume is increased by an additional of
500ml
Increased fetoprotein level and GFR
140.
History…
Patient profile:
Etiological factors; with positive past history and family history
specially maternal.
Early pregnancy
Hyperemesis, bleeding.
Mid-pregnancy
Greater weight gain than expected
Abdominal size > period of amenorrhea
early PIH symptoms, persistent fetal activity.
Late pregnancy
Pressure symptoms (dyspnea, dyspepsia, UTI, piles, edema and
varicose veins in LL).
141.
Examination
General:
An earlyincrease weight gain,
Pallor
Less mid-trimisteric fall blood pressure
Early PIH
Eary edema, and varicose veins in LL.
Abdominal:
Fundal level > amenorrhea especially in mid-pregnancy
exclude other causes.
Palpation: Multiple fetal
identify presentations.
Auscultation of FHS:
2 different recordings by 2 observers and a difference > 10 bpm a Gallop between 2
points[ Arnoux sign]
Pelvic: Specially during the course of labor
small presenting part compared to abdominal size
142.
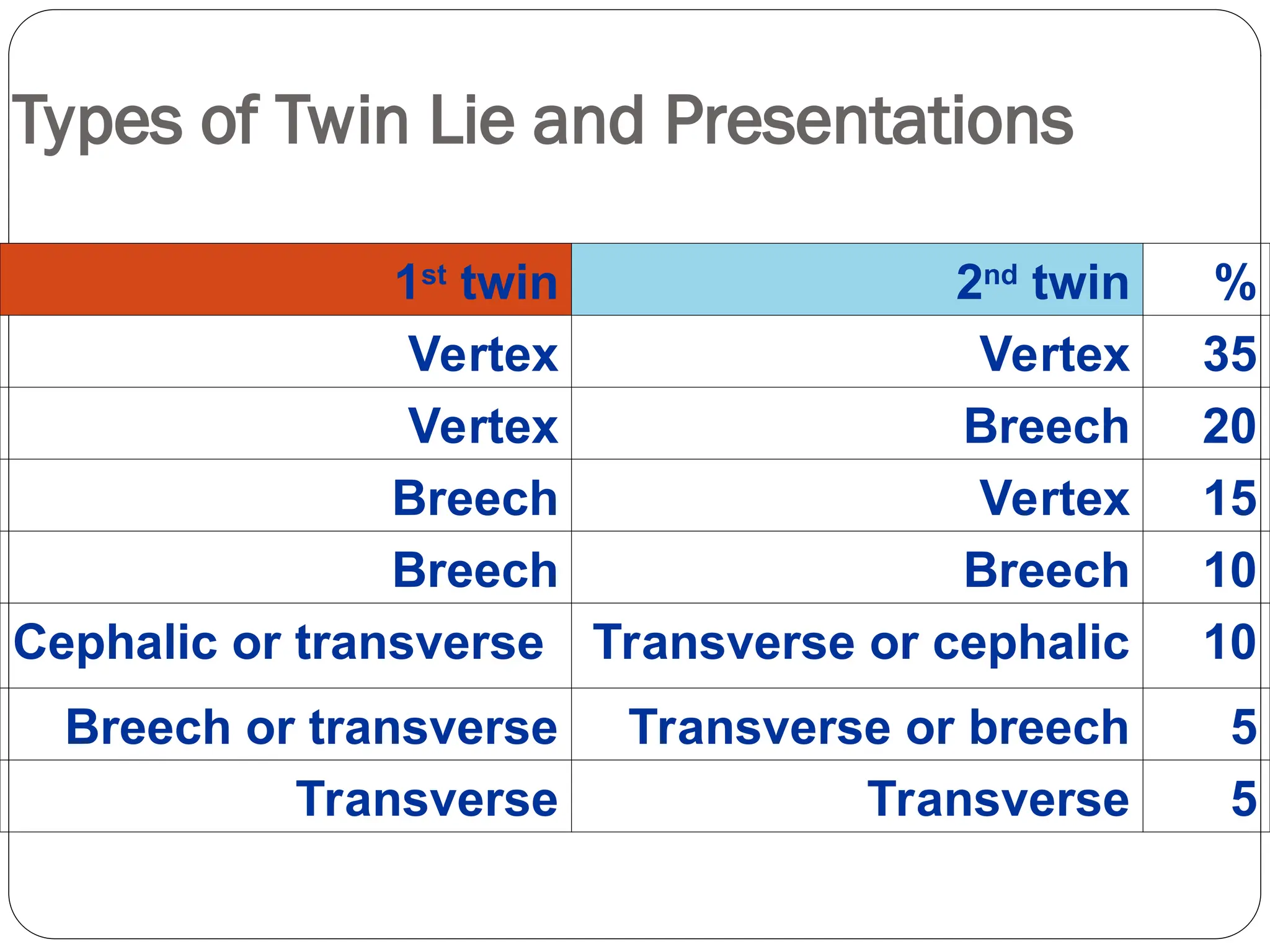
Types of TwinLie and Presentations
1st
twin 2nd
twin %
Vertex Vertex 35
Vertex Breech 20
Breech Vertex 15
Breech Breech 10
Cephalic or transverse Transverse or cephalic 10
Breech or transverse Transverse or breech 5
Transverse Transverse 5
143.
Selective Embryo Reduction
The presence of > 3 fetuses carries the risk of losing
them all (preterm delivery).
The number is reduced to twins only by injecting
potassium chloride intracardiac under U/S guidance
(about 1.5 ml of 15% solution).
Potassium chloride may diffuse and affect other fetuses.
144.
Maternal Complications
DURING PREGNANCY
Nausea and vomiting
Anaemia
Pre eclampsia
Hydramnios
Antepartum haemorrhage
Malpresentation
Preterm labour
Mechanical distress
145.
Maternal Complications
DURING LABOUR
Early rupture of membranes and cord prolapse
Prolonged labour
Increased operative interference
Bleeding
Postpartum haemorrhage
DURING PUERPERIUM
Sub involution
Infection
Lactation failure
146.
Fetal Complications
Miscarriagerate is increased
Premature rate
Growth problem
Intrauterine death of one fetus
Fetal anomalies
Asphyxia and still birth
147.
Antenatal Management
ANTENATALADVISES
Diet – extra 300 Kcal, extra protein
Increased rest at home
Travel restriction
Supplementary therapy – Fe 60-100mg,Additional Ca, Vitamin
and Folic acid
Frequent antenatal visit
Prophylactic os tightening
Fetal surveillance
HOSPITALISATION
Management During Labour
DELIVERY OF THE FIRST BABY
Same as singleton pregnancy
Liberal episiotomy
Forceps delivery
Do not give IV ergometrine with the delivery of the anterior
shoulder of the first baby
Clamp cord at two places and cut in between
Leave at leat 8-10 cm of the cord
Label bay as no 1
150.
Contd….
DELIVERY OFTHE SECOND BABY
External cephalic version
Rupture fore water after correcting the lie
Wait for 10min for spontaneous delivery
Syntocinon drip
Vaccum extraction or Breech extraction
151.
Contd….
CESAREAN SECTION
Severe PIH
Bad obstetrics history
Long history of infertility
Elderly primi
Preterm delivery
Breech presentation
152.
MANAGEMENT OFTHIRD STAGE AND PUERPARIUM
Prevention of PPH
Treatment of anemia
Psychological adjustment
Family planning advice
153.
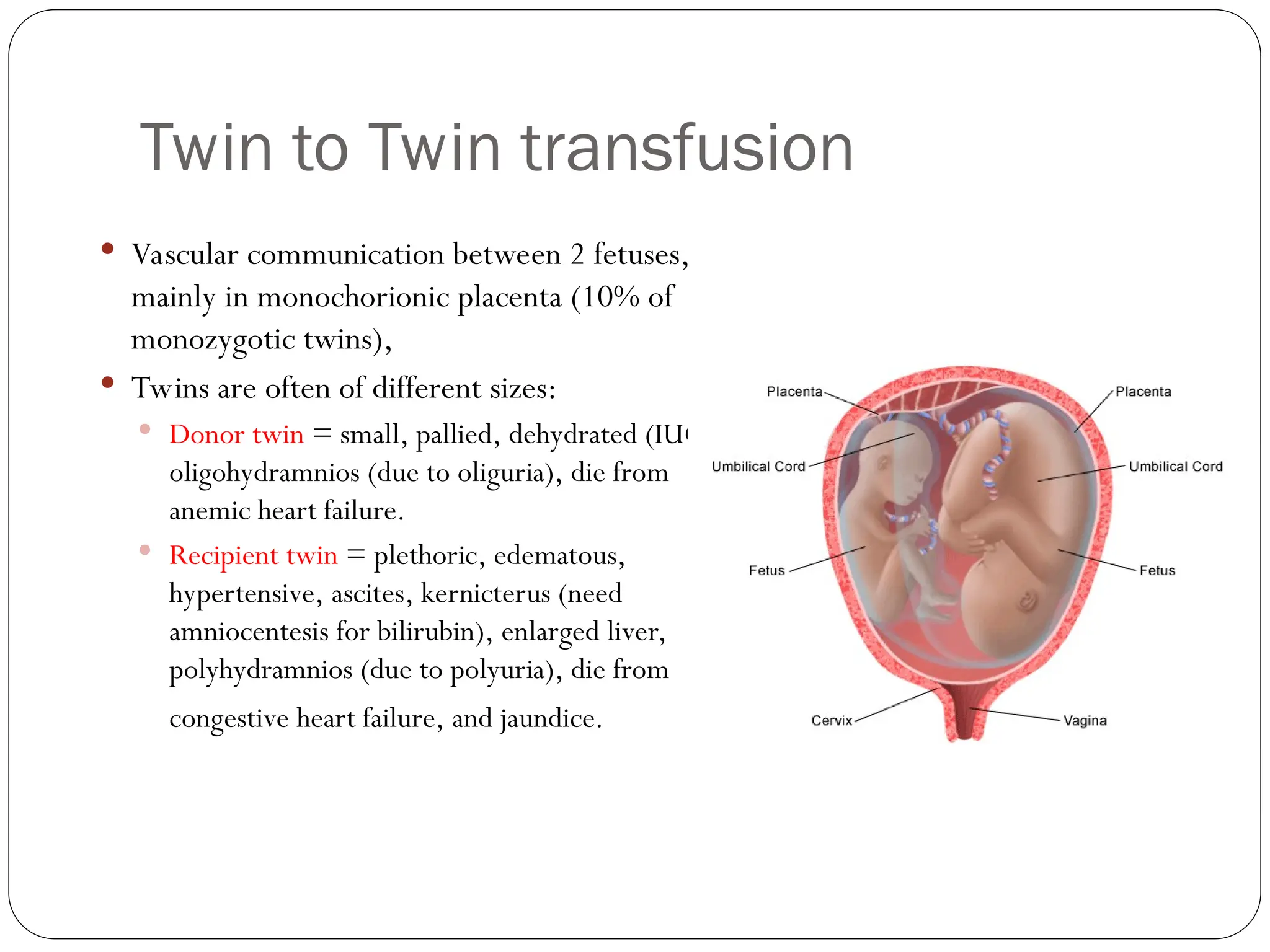
Twin to Twintransfusion
Vascular communication between 2 fetuses,
mainly in monochorionic placenta (10% of
monozygotic twins),
Twins are often of different sizes:
Donor twin = small, pallied, dehydrated (IUGR),
oligohydramnios (due to oliguria), die from
anemic heart failure.
Recipient twin = plethoric, edematous,
hypertensive, ascites, kernicterus (need
amniocentesis for bilirubin), enlarged liver,
polyhydramnios (due to polyuria), die from
congestive heart failure, and jaundice.
DEFINITION
•Fetal distress isthe term commonly used to describe
Fetal distress is the term commonly used to describe
fetal
fetal hypoxia
hypoxia
•It is a clinical diagnosis made by
It is a clinical diagnosis made by indirect
indirect methods and
methods and
should be defined as:
should be defined as:
Hypoxia that may result in fetal damage / death if not
Hypoxia that may result in fetal damage / death if not
reversed or the fetus delivered immediately
reversed or the fetus delivered immediately
•It includes
It includes acute
acute distress and
distress and chronic
chronic distress
distress
MECHANISM
There arepotentially limitless causes for fetal distress, but
There are potentially limitless causes for fetal distress, but
several key mechanisms are usually involved
several key mechanisms are usually involved
Contractions reduce temporarily placental blood flow and can
Contractions reduce temporarily placental blood flow and can
compress the umbilical cord
compress the umbilical cord
If a women is in labor longer then this can cause fetal distress via
If a women is in labor longer then this can cause fetal distress via
the above mechanism
the above mechanism
162.
MECHANISM
Acute distresscan be a result of:
Acute distress can be a result of:
placental abruption
placental abruption
prolapse of the umbilical cord
prolapse of the umbilical cord (especially with breech presentations)
(especially with breech presentations)
hypertonic uterine states
hypertonic uterine states
use of oxytocin
use of oxytocin
Hypotension
Hypotension can be caused by either epidural anesthesia or the
can be caused by either epidural anesthesia or the
supine position, which reduces inferior vena cava return of blood to
supine position, which reduces inferior vena cava return of blood to
the heart
the heart
The decreased blood flow in hypotension can be a cause of fetal
The decreased blood flow in hypotension can be a cause of fetal
distress
distress
Cardiotocography signs:
Cardiotocographysigns:
Increased / decreased fetal heart
Increased / decreased fetal heart (tachycardia and bradycardia),
(tachycardia and bradycardia),
especially
especially during
during and
and after
after a contraction decreased varibility in the
a contraction decreased varibility in the
fetal heart rate
fetal heart rate
Abnormal fetal heart rate
Abnormal fetal heart rate (< 120 or > 160 bpm)
(< 120 or > 160 bpm)
A normal fetal heart rate may slow during a contraction but usually recovers to
A normal fetal heart rate may slow during a contraction but usually recovers to
normal as soon as the uterus relaxes
normal as soon as the uterus relaxes
A very slow fetal heart rate in the absence of contractions or persisting after
A very slow fetal heart rate in the absence of contractions or persisting after
contractions is suggestive of fetal distress
contractions is suggestive of fetal distress
SIGNS AND SYMPTOMS
165.
A
A rapidfetal heart rate
rapid fetal heart rate may be a response to:
may be a response to:
maternal fever
maternal fever
drugs
drugs
hypertension
hypertension
amnionitis
amnionitis
In the absence of a rapid maternal heart rate, a rapid fetal heart
In the absence of a rapid maternal heart rate, a rapid fetal heart
rate = a sign of fetal distress
rate = a sign of fetal distress
For a diagnosis of fetal distress to be made, one or more of the
For a diagnosis of fetal distress to be made, one or more of the
following must be present:
following must be present:
persistent severe variable deceleration
persistent severe variable deceleration
persistent and non-remediable late declarations
persistent and non-remediable late declarations
persistent severe bradycardia
persistent severe bradycardia
SIGNS AND SYMPTOMS
166.
Amniotic fluidis contaminated by
Amniotic fluid is contaminated by meconium
meconium
There are 3 degrees about contaminated
There are 3 degrees about contaminated
I -
I - slight
slight contamination
contamination
The color of the amniotic fluid =
The color of the amniotic fluid = slight green
slight green
II
II -
- mild
mild contamination
contamination
Color of the amniotic fluid =
Color of the amniotic fluid = dark green
dark green
III -
III - severe
severe contamination
contamination
Color of the amniotic fluid is dark yellow.
Color of the amniotic fluid is dark yellow.
If the amniotic fluid is severely contamination, it suggests the,
If the amniotic fluid is severely contamination, it suggests the, fetal distress
fetal distress -
-
it must be managed as soon as possible
it must be managed as soon as possible
SIGNS AND SYMPTOMS
167.
Decreased fetalmovement felt by the mother
Decreased fetal movement felt by the mother
Biochemical signs - assessed by collecting a small sample of
Biochemical signs - assessed by collecting a small sample of
baby‘s blood from a scalp prick through the open cervix in
baby‘s blood from a scalp prick through the open cervix in
labor:
labor:
Fetal acidosis elevated fetal blood lactate levels
Fetal acidosis elevated fetal blood lactate levels
A fetal scalp
A fetal scalp pH < 7.2
pH < 7.2 ,
, Po
Po2
2 >60mmHg
>60mmHg suggests fetal distress
suggests fetal distress
SIGNS AND SYMPTOMS
Decreased ordisappear fetal movement:
Decreased or disappear fetal movement:
< 10 times per 12 hours is regarded as decreased
< 10 times per 12 hours is regarded as decreased
With the first effect of hypoxia, the fetal movement is increased
With the first effect of hypoxia, the fetal movement is increased
If the hypoxia persists, the fetal movement is decreased, and may
If the hypoxia persists, the fetal movement is decreased, and may
disappear
disappear
If the fetal movement lost, the fetal heart beat will be disappearing
If the fetal movement lost, the fetal heart beat will be disappearing
within 24 hours
within 24 hours
Cautions: Dangerous for the fetus if the fetal movement disappear.
Cautions: Dangerous for the fetus if the fetal movement disappear.
Management immediately!!
Management immediately!!
SIGNS AND SYMPTOMS
170.
Abnormal cardiotocographysigns:
Abnormal cardiotocography signs:
Slow fetal heart rate(<120bpm) or rapid fetal heart rate
Slow fetal heart rate(<120bpm) or rapid fetal heart rate
(>180bpm)
(>180bpm) last more than 10 min
last more than 10 min in the absence of
in the absence of
contractions
contractions is suggestive
is suggestive of fetal distress
of fetal distress
The fetal heart rate > 160 bpm , especially > 180 bpm, it
The fetal heart rate > 160 bpm , especially > 180 bpm, it
suggests
suggests early hypoxia
early hypoxia, unless the maternal heart rate is faster
, unless the maternal heart rate is faster
SIGNS AND SYMPTOMS
171.
FHR <120bpm, typically less than 100bpm
FHR < 120bpm, typically less than 100bpm
It is very danger for fetus
It is very danger for fetus
The fetal heart rate normally show continuous minor
The fetal heart rate normally show continuous minor
variations, with a range of about 5 bpm, loss of base line
variations, with a range of about 5 bpm, loss of base line
variability implies that the cardiac reflexes are impaired,
variability implies that the cardiac reflexes are impaired,
either from the effect of
either from the effect of hypoxia
hypoxia or of
or of drugs
drugs such as
such as valium
valium
It may be serious
It may be serious
SIGNS AND SYMPTOMS
172.
Early deceleration
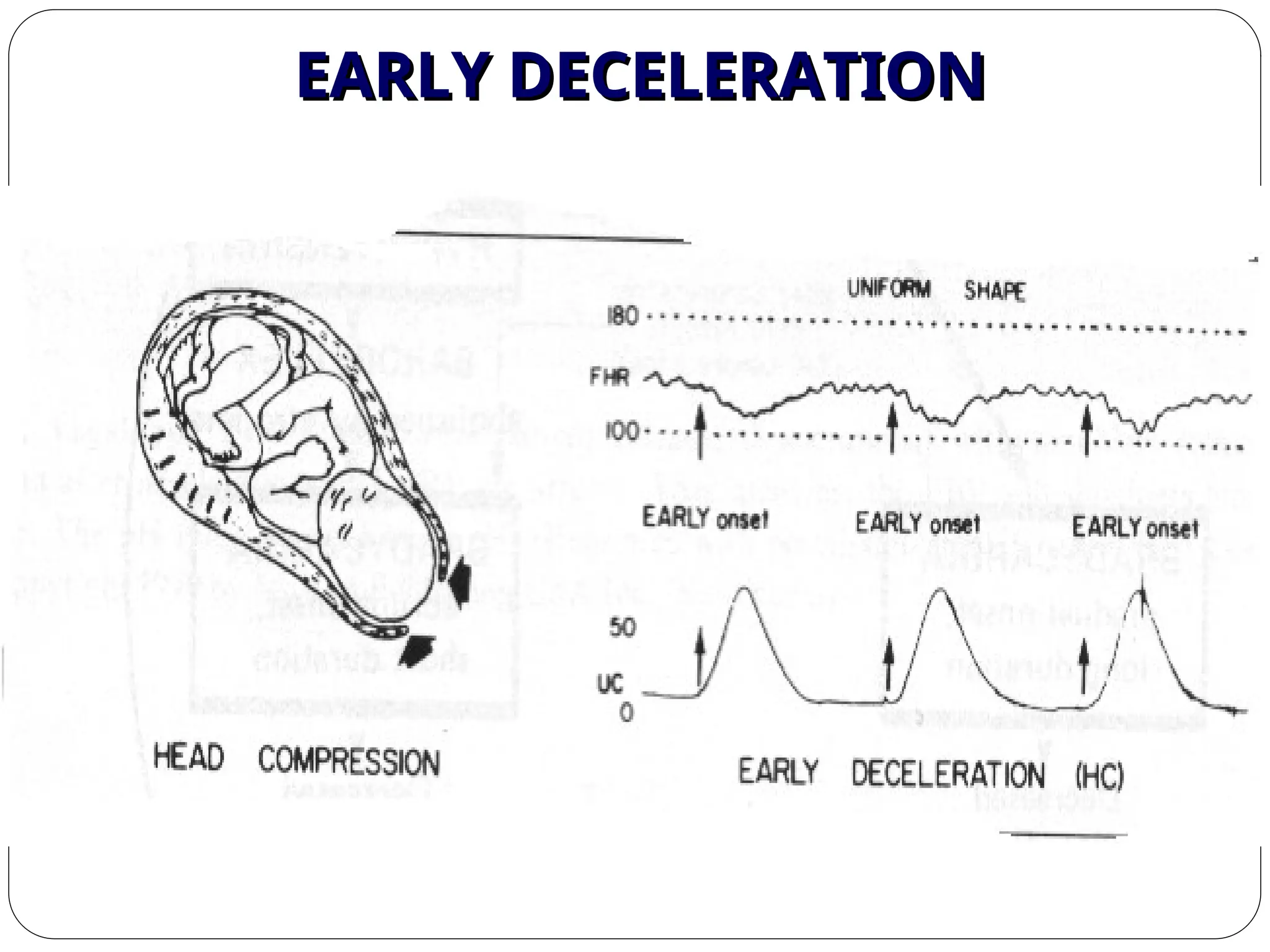
Earlydeceleration: with each contraction the rate often slows, but
: with each contraction the rate often slows, but
it returns to normal soon after removal of the stress
it returns to normal soon after removal of the stress
The early deceleration in the heart rate start within 30 seconds of
The early deceleration in the heart rate start within 30 seconds of
the onset of the contraction and return rapidly to the baseline rate
the onset of the contraction and return rapidly to the baseline rate
It is not of serious significance
It is not of serious significance as a rule and indicate that while the
as a rule and indicate that while the
fetus is undergoing some stress the cardiac control mechanisms are
fetus is undergoing some stress the cardiac control mechanisms are
responding normally
responding normally
SIGNS AND SYMPTOMS
Variable deceleration
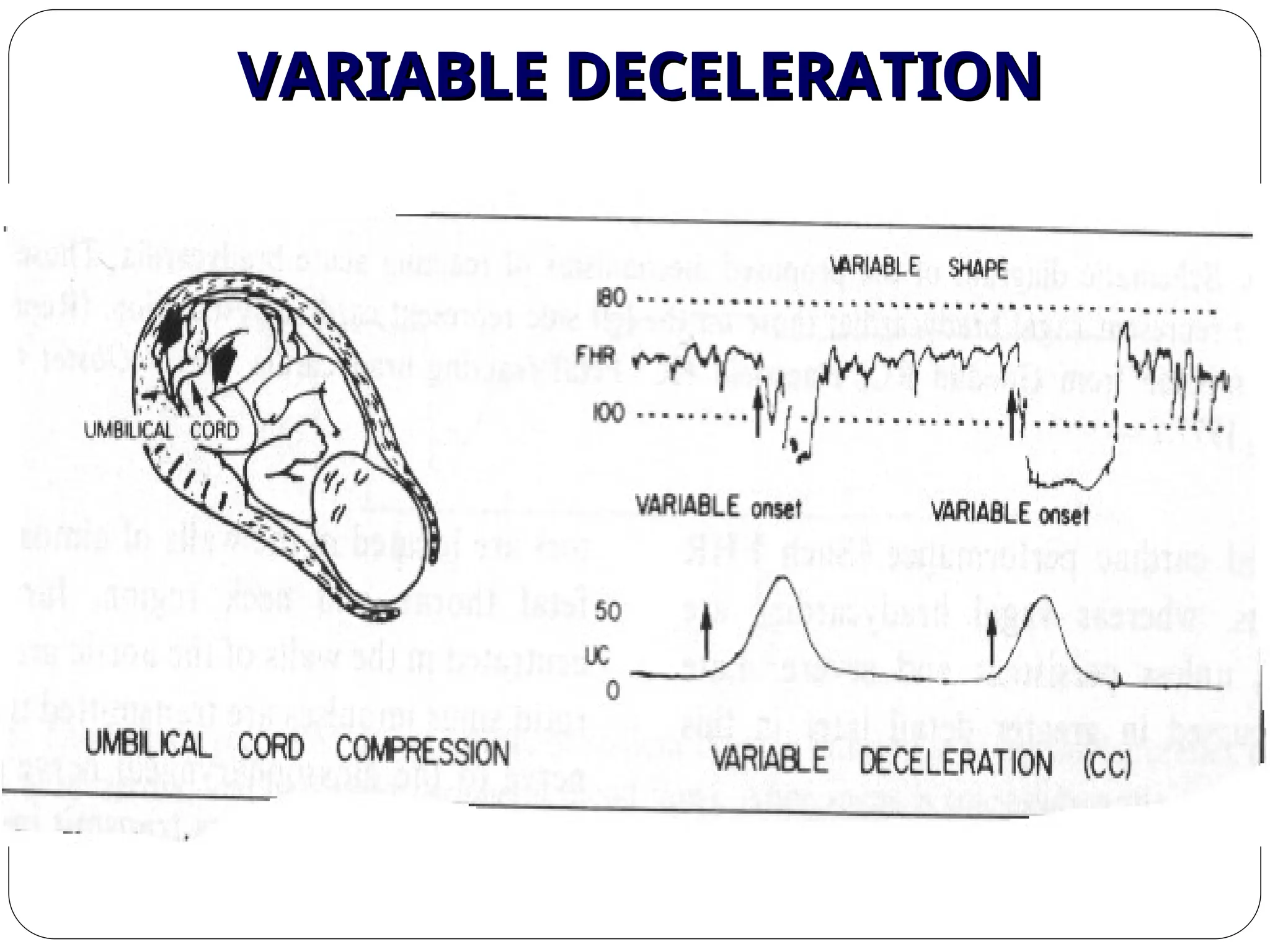
Variabledeceleration: no consistent relationship with uterine
: no consistent relationship with uterine
contraction.
contraction.
It is sometimes caused by compression of the umbilical cord
It is sometimes caused by compression of the umbilical cord
between the uterus and the fetal body, or because it is looped
between the uterus and the fetal body, or because it is looped
round some part of the fetus
round some part of the fetus
Provided that it does not persist for more than a few minutes it
Provided that it does not persist for more than a few minutes it
may have little significance, but
may have little significance, but persistence for more than 15
persistence for more than 15
minutes
minutes would call for treatment
would call for treatment
SIGNS AND SYMPTOMS
The mostserious pattern of heart rate changes is
The most serious pattern of heart rate changes is fetal bradycardia
fetal bradycardia
with loss of baseline variability and
with loss of baseline variability and late decelerations
late decelerations
Decrease (defined as onset of deceleration to nadir =30 seconds)
Decrease (defined as onset of deceleration to nadir =30 seconds)
and return to baseline FHR associated with a uterine contraction.
and return to baseline FHR associated with a uterine contraction.
The deceleration is delayed in timing, with the nadir of the
The deceleration is delayed in timing, with the nadir of the
deceleration occurring after the peak on the contraction
deceleration occurring after the peak on the contraction
SIGNS AND SYMPTOMS
Biophysical Profile:
BiophysicalProfile:
Amniotic Fluid Volume Normal = 2 Points
Amniotic Fluid Volume Normal = 2 Points
Non-Stress Test Result Positive = 2 Points
Non-Stress Test Result Positive = 2 Points
Fetal Breathing Movements Active = 2 Points
Fetal Breathing Movements Active = 2 Points
Fetal Extremity/Trunk Movements Active = 2 Points
Fetal Extremity/Trunk Movements Active = 2 Points
Fetal Movements Active= 2 Points
Fetal Movements Active= 2 Points
If Biophysical Profile scores
If Biophysical Profile scores < 4
< 4 suggest fetal distress
suggest fetal distress
Placental Insufficiency: Low estriol levels, E
Placental Insufficiency: Low estriol levels, E3
3 in urine
in urine <
<
10mg/24h
10mg/24h
BIOPHYSICAL PROFILE
179.
TREATMENT
Reposition patient:left-side-lying position
Reposition patient: left-side-lying position
Administer oxygen by mask
Administer oxygen by mask
Perform vaginal examination to check for prolapsed cord
Perform vaginal examination to check for prolapsed cord
Ensure that qualified personnel are in attendance for resuscitation
Ensure that qualified personnel are in attendance for resuscitation
and care of the newborn
and care of the newborn
Note: each institution shall define in writing the term qualified
Note: each institution shall define in writing the term qualified
personnel for resuscitation and care of the newborn
personnel for resuscitation and care of the newborn
180.
Each ofthe following actions should be performed and
Each of the following actions should be performed and
documented prior to starting a Cesarean section for fetal distress:
documented prior to starting a Cesarean section for fetal distress:
Perform vaginal exam to rule out imminent vaginal delivery
Perform vaginal exam to rule out imminent vaginal delivery
Initiate preoperative routines
Initiate preoperative routines
Monitor fetal heart tones (by continuous fetal monitoring or by
Monitor fetal heart tones (by continuous fetal monitoring or by
auscultation) immediately prior to preparation of the abdomen
auscultation) immediately prior to preparation of the abdomen
TREATMENT
181.
Ensure thatqualified personnel are in attendance for
Ensure that qualified personnel are in attendance for
resuscitation and care of the newborn (each institution shall
resuscitation and care of the newborn (each institution shall
define in writing the term qualified personnel for resuscitation
define in writing the term qualified personnel for resuscitation
and care of the newborn)
and care of the newborn)
STOP
STOP using
using oxytocin
oxytocin !
!
Oxytocin can strengthen the contraction of uterine which
Oxytocin can strengthen the contraction of uterine which
affects the baby's heart rate
affects the baby's heart rate
TREATMENT
182.
DEFINITIONS MUST GRASPED
Baseline FHR
Baseline FHR:
:
approximate mean FHR rounded to increments of 5 bpm
approximate mean FHR rounded to increments of 5 bpm
during a 10-minute segment, excluding periodic or episodic
during a 10-minute segment, excluding periodic or episodic
changes, periods of marked FHR variability, and segments of
changes, periods of marked FHR variability, and segments of
the baseline that differ by > 25 bpm
the baseline that differ by > 25 bpm
In any 10-minute window, the minimum baseline duration
In any 10-minute window, the minimum baseline duration
must be at least 2 minutes or the baseline for that period is
must be at least 2 minutes or the baseline for that period is
indeterminate
indeterminate
183.
Baseline FHRvariability
Baseline FHR variability:
:
Fluctuations in the baseline FHR =2 cycles / min
Fluctuations in the baseline FHR =2 cycles / min
These fluctuations are irregular in amplitude and frequency, and are
These fluctuations are irregular in amplitude and frequency, and are
visually quantitated as the amplitude of the peak to the trough in beats
visually quantitated as the amplitude of the peak to the trough in beats
per minute as follows:
per minute as follows:
amplitude range undetectable, absent FHR variability;
amplitude range undetectable, absent FHR variability;
amplitude range greater than undetectable but = 5 bpm, minimal FHR
amplitude range greater than undetectable but = 5 bpm, minimal FHR
variability;
variability;
amplitude range 6 bpm to 25 bpm, moderate FHR variability;
amplitude range 6 bpm to 25 bpm, moderate FHR variability;
amplitude range >25 bpm, marked FHR variability
amplitude range >25 bpm, marked FHR variability
DEFINITIONS MUST GRASPED
184.
Bradycardia
Bradycardia:
:
abaseline FHR <120 bpm
a baseline FHR <120 bpm
Tachycardia
Tachycardia:
:
a baseline FHR >160 bpm
a baseline FHR >160 bpm
DEFINITIONS MUST GRASPED
185.
Early deceleration
Earlydeceleration:
:
a visually-apparent, gradual decrease (defined as onset of
a visually-apparent, gradual decrease (defined as onset of
deceleration to nadir =30 seconds) and return to baseline FHR
deceleration to nadir =30 seconds) and return to baseline FHR
associated with a uterine contraction
associated with a uterine contraction
The decrease is calculated from the most recently determined
The decrease is calculated from the most recently determined
portion of the baseline
portion of the baseline
It is coincident in timing with the nadir of the deceleration occurring
It is coincident in timing with the nadir of the deceleration occurring
at the same time as the peak of the contraction
at the same time as the peak of the contraction
In most cases the onset, nadir, and recovery of the deceleration are
In most cases the onset, nadir, and recovery of the deceleration are
coincident with the beginning, peak, and ending of the contraction,
coincident with the beginning, peak, and ending of the contraction,
respectively
respectively
DEFINITIONS MUST GRASPED
186.
Variable deceleration
Variabledeceleration:
:
a visually-apparent, abrupt decrease in FHR below the baseline
a visually-apparent, abrupt decrease in FHR below the baseline
The decrease is calculated from the most recently determined portion
The decrease is calculated from the most recently determined portion
of the baseline
of the baseline
The decrease in FHR below the baseline is =15 bpm, lasting =15
The decrease in FHR below the baseline is =15 bpm, lasting =15
seconds and =2 minutes from onset to return to baseline
seconds and =2 minutes from onset to return to baseline
DEFINITIONS MUST GRASPED
187.
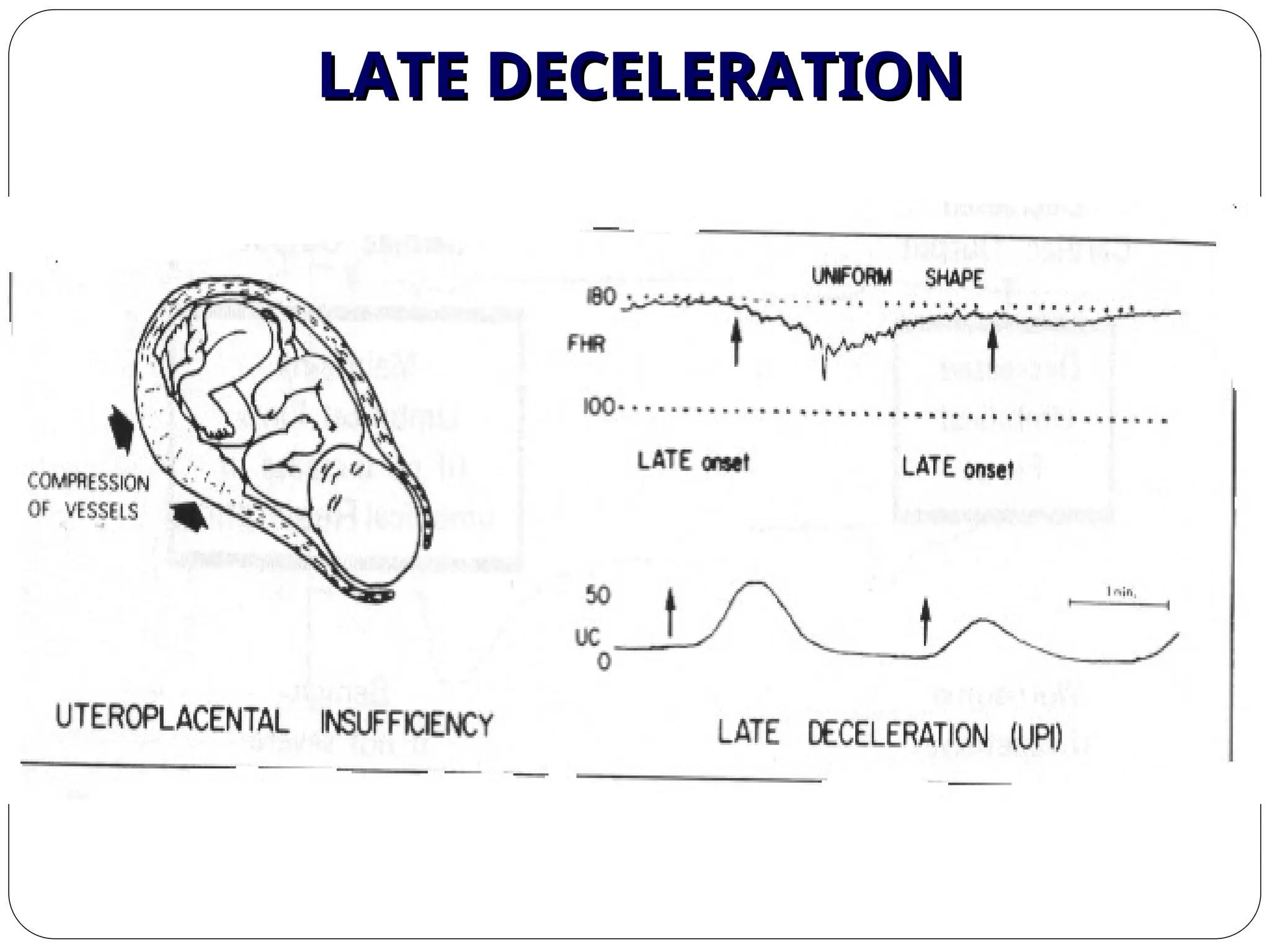
Late deceleration
Latedeceleration:
:
a visually-apparent, gradual decrease (defined as onset of
a visually-apparent, gradual decrease (defined as onset of
deceleration to nadir = 30 seconds) and return to baseline FHR
deceleration to nadir = 30 seconds) and return to baseline FHR
associated with a uterine contraction
associated with a uterine contraction
The decrease is calculated from the most recently determined
The decrease is calculated from the most recently determined
portion of the baseline
portion of the baseline
The deceleration is delayed in timing, with the nadir of the
The deceleration is delayed in timing, with the nadir of the
deceleration occurring after the peak on the contraction
deceleration occurring after the peak on the contraction
DEFINITIONS MUST GRASPED
188.
DIAGNOSIS:
DIAGNOSIS:
Absence of uterinegrowth
Absence of uterine growth
Serial ß-hcg
Serial ß-hcg
Loss of fetal movement
Loss of fetal movement
Absence of fetal heart
Absence of fetal heart
Disappearance of the signs & symptoms of pregnancy
Disappearance of the signs & symptoms of pregnancy
X-ray
X-ray
Spalding sign
Spalding sign
Robert’s sign
Robert’s sign
U/S
U/S
100% accurate Dx
100% accurate Dx
DEFINITION:
DEFINITION:
• dead fetuses or newborns weighing > 500g or > 20
dead fetuses or newborns weighing > 500g or > 20
wks gestation
wks gestation
4.5
4.5
/
/
1000
1000
total births
total births
INTRAUTERINE FETAL DEATH (IUFD)
INTRAUTERINE FETAL DEATH (IUFD)
A systematic approachto fetal death is valuable in
A systematic approach to fetal death is valuable in
determining the etiology
determining the etiology
1
1
-
-
HISTORY
HISTORY
A-Family history
A-Family history
•Recurrent abortions
Recurrent abortions
•VTE/ PE
VTE/ PE
•Congenital anomalies
Congenital anomalies
•Abnormal karyptype
Abnormal karyptype
•Hereditary conditions
Hereditary conditions
•Developmental delay
Developmental delay
B-Maternal History
B-Maternal History
I-Maternal medical conditions
I-Maternal medical conditions
•VTE/ PE
VTE/ PE
•DM
DM
•HPT
HPT
•Thrombophilia
Thrombophilia
•SLE
SLE
•Autoimmune disease
Autoimmune disease
•Severe Anemia
Severe Anemia
•Epilepsy
Epilepsy
•Consanguinity
Consanguinity
•Heart disease
Heart disease
II-Past OB Hx
II-Past OB Hx
•Baby with congenital anomaly / hereditary
Baby with congenital anomaly / hereditary
condition
condition
•IUGR
IUGR
•Gestational HPT with adverse sequele
Gestational HPT with adverse sequele
•Placental abruption
Placental abruption
•IUFD
IUFD
•Recurrent abortions
Recurrent abortions
191.
Current Pregnancy Hx
CurrentPregnancy Hx
•Maternal age
Maternal age
•Gestational age at fetal death
Gestational age at fetal death
•HPT
HPT
•DM/ Gestational D
DM/ Gestational D
•Smooking , alcohol, or drug abuse
Smooking , alcohol, or drug abuse
•Abdominal trauma
Abdominal trauma
•Cholestasis
Cholestasis
•Placental abruption
Placental abruption
•PROM or prelabor SROM
PROM or prelabor SROM
Specific fetal conditions
Specific fetal conditions
•Nonimmune hydrops
Nonimmune hydrops
•IUGR
IUGR
•Infections
Infections
•Congenital anomalies
Congenital anomalies
•Chromosomal abnormalities
Chromosomal abnormalities
•Complications of multiple gestation
Complications of multiple gestation
Placental or cord complications
Placental or cord complications
•Large or small placenta
Large or small placenta
•Hematoma
Hematoma
•Edema
Edema
•Large infarcts
Large infarcts
•Abnormalities in structure , length
Abnormalities in structure , length
or insertion of the umbilical cord
or insertion of the umbilical cord
•Cord prolapse
Cord prolapse
•Cord knots
Cord knots
•Placental tumors
Placental tumors
1
1
-
-
HISTORY
HISTORY
192.
2-EVALUATION OF STILLBORN INFANTS
2-EVALUATION OF STILL BORN INFANTS
Infant description
Infant description
•Malformation
Malformation
•Skin staining
Skin staining
•Degree of maceration
Degree of maceration
•Color-pale ,plethoric
Color-pale ,plethoric
Umbilical cord
Umbilical cord
•Prolapse
Prolapse
•Entanglement-neck, arms,
Entanglement-neck, arms,
legs
legs
•Hematoma or stricture
Hematoma or stricture
•Number of vessels
Number of vessels
•Length
Length
Amniotic fluid
Amniotic fluid
•Color-meconium, blood
Color-meconium, blood
•Volume
Volume
Placenta
Placenta
•Weight
Weight
•Staining
Staining
•Adherent clots
Adherent clots
•Structural abnormality
Structural abnormality
•Velamentous insertion
Velamentous insertion
•Edema/hydropic changes
Edema/hydropic changes
Membranes
Membranes
•Stained
Stained
•Thickening
Thickening
193.
3
3
-
-
INVESTIGATIONS
INVESTIGATIONS
Maternal investigations
Maternal investigations
•CBC
CBC
•BlGp & antibody screen
Bl Gp & antibody screen
•HB A1 C
HB A1 C
•Kleihauer Batke test
Kleihauer Batke test
•Serological screening for Rubella
Serological screening for Rubella
•CMV, Toxo, Sphylis, Herpes &
CMV, Toxo, Sphylis, Herpes &
Parovirus
Parovirus
•Karyotyping of both parents (RFL,
Karyotyping of both parents (RFL,
Baby with malformation
Baby with malformation
•Hb electrophorersis
Hb electrophorersis
•Antiplatelet anbin tibodies
Antiplatelet anbin tibodies
•Throbophilia screening
Throbophilia screening
(antithrombin
(antithrombin
Protein C & S , factor IV leiden,
Protein C & S , factor IV leiden,
Factor II mutation, , lupus
Factor II mutation, , lupus
anticoagulant,
anticoagulant,
anticardolipin antibodies)
anticardolipin antibodies)
•DIC
DIC
Fetal investigations
Fetal investigations
•Fetal autopsy
Fetal autopsy
•Karyotype
Karyotype
(
(
specimen taken from cord
specimen taken from cord
blood, intracardiac blood
blood, intracardiac blood
,
,
body fluid, skin, spleen
body fluid, skin, spleen
,
,
placental wedge, or amniotic
placental wedge, or amniotic
fluid
fluid
)
)
•Fetography
Fetography
•Radiography
Radiography
Placental investigations
Placental investigations
•Chorionocity of placenta in
Chorionocity of placenta in
twins
twins
•Cord thrombosis or knots
Cord thrombosis or knots
•Infarcts, thrombosis,
Infarcts, thrombosis,
abruption
abruption
•Vascular malformations
Vascular malformations
•Signs of infection
Signs of infection
•Bacterial culture for E.coli,
Bacterial culture for E.coli,
Listeria, gp B strpt
Listeria, gp B strpt
.
.
194.
IUFD COMPLICATIONS
IUFD COMPLICATIONS
•Hypofibrinogenemia
Hypofibrinogenemia
4-5 wks after IUFD
4-5 wks after IUFD
• Coagulation studies must be started 2 wks after
Coagulation studies must be started 2 wks after
IUFD
IUFD
• Delivery by 4 wks or if fibrinogen
Delivery by 4 wks or if fibrinogen
< 200mg/ml
< 200mg/ml
195.
PSYCHOLOGICAL ASPECT &COUNSELING
PSYCHOLOGICAL ASPECT & COUNSELING
• A traumatic event
A traumatic event
• Post-partum depression
Post-partum depression
• Anxiety
Anxiety
• Psychotherapy
Psychotherapy
• Recurrence 0-8% depending on the cause of IUFD
Recurrence 0-8% depending on the cause of IUFD
DEFINITION
The placenta issaid to be retained when it is
not expelled out even 30mts after the birth of
the baby.
C.S. Dawn
199.
Gross anatomy ofmature placenta
Shape - Circular disc
Diameter - 15-20cm
Thickness - 2.5cm at its centre,
thin off towards the edge
By touch - It feels spongy
Weights - about 500gm
Surface - fetal surface and
maternal surface
200.
Phases in expulsionof placenta
1.Separation through the spongy layer of
decidua
2.Descent into the lower segment and vagina
3.Finally its expulsion to outside
201.
Causes of retainedplacenta
- Poor voluntary expulsive efforts
- Uterine atonicity in cases of grand multipara overdistension
of uterus, prolonged labour, uterine malformation
- Incarcerated placenta following partially or completely
separated. It is due to constriction ring (hour – glass
contraction)
DANGERS:
They are:
1. Post-partumhaemorrhage.
2. Shock – mainly due to haemorrhage.
3. Puerperal sepsis.
4. Thrombophlebitis – in the pelvic and leg veins.
5. Embolism
6. Placental polyp.
205.
Diagnosis
Diagnosis is madeby an arbitary time spent following
delivery of the baby
Dangers
1. Haemorrhage
2. Shock is due to a. Blood loss
b. Retained more than one hour
c. Frequent attempts of abdominal
manipulation
3. Puerperal sepsis
4. Risk of its recurrence in next pregnancy
206.
Management
Period ofwatchful expectancy
•Watch for bleeding
•Note the signs of separation of placenta
•The bladder should be emptied using a rubber catheter
•Any bleeding during the period should be managed.
Placenta is separated and retained
- To express the placenta out by controlled cord traction. - -
Unseparated retained plaenta
- Manual removal of placenta under G.A
207.
Management of unforseencomplications during manual
removal
1. Hour glass contraction – placenta either inseparated or
separated – partially or completely, may be trapped by a
localised contraction of circular muscles of the uterus.
This ring should be made to relax by
a. Deepening the plane of plane of anaesthesia (halothane)
b. Subcutaneous injection of .5ml of 1 in 1000 adrenaline Hcl.
208.
c. Inhalation oftwo amyl nitrate capsules of 5 minim each.
If the ring is too tight and bleeding is absent
• Operation is to be postponed
• The patient is to be sedated by morphine 15mg Im
after the manual removal.
• Watch for a period of 4-6hrs
If the ring is not too tight and bleeding is continuing
The ring is to be manually stretched by the cone shaped
hand and the separation of the placenta is preferably
done from above down wards to minimise bleeding.
209.
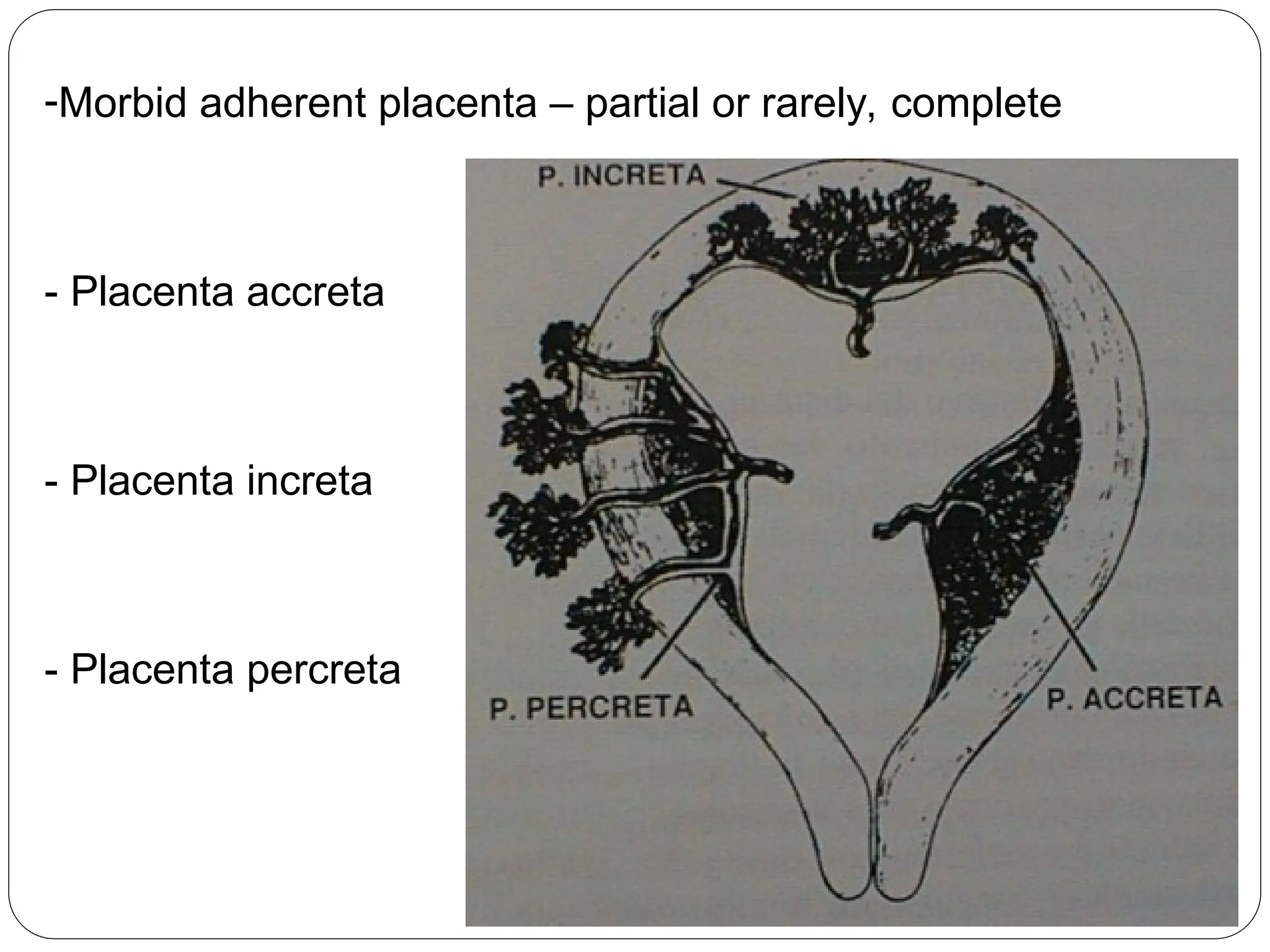
Morbid adherent placenta
-Manualremoval
Management of complicated retained placenta
1. Retained placenta with shock but no haemorrhage
• To treat shock
• Manual removal of placenta when the condition
improves.
2. Retained placenta with haemorrhage
• To assess the amount blood loss and to replace the lost
blood
210.
3. Retained placentawith sepsis
• Intrauterine swabs are taken for culture
• Administer broad spectrum antibiotic
• Blood transfusion
4. Retained placenta with an episiotomy wound
• The bleeding points of the episiotomy wound are to be
secured by artery forceps
• Manual removal of placenta followed by repair of
episiotomy wound.
211.
Placenta Acreta (morbidadherent placenta)
• The placenta is directly anchored to the myometrium partially
or completely without any intervening decidna.
• Probable cause is defective decidual formation
• The condition is usually associated when the placenta
happens to be implanted in lower segment.
212.
Management
•In case ofpartial morbid adherent placenta
•Manual removal if there is effective uterine contractions with
haemostasis
•If the uterus fails to contract an early decision of hystrectomy may
have to be taken.
213.
In totalplacenta accreta hysterectomy is indicated
• It the patient desiring to have a child conservative
management.
• Antibiotics
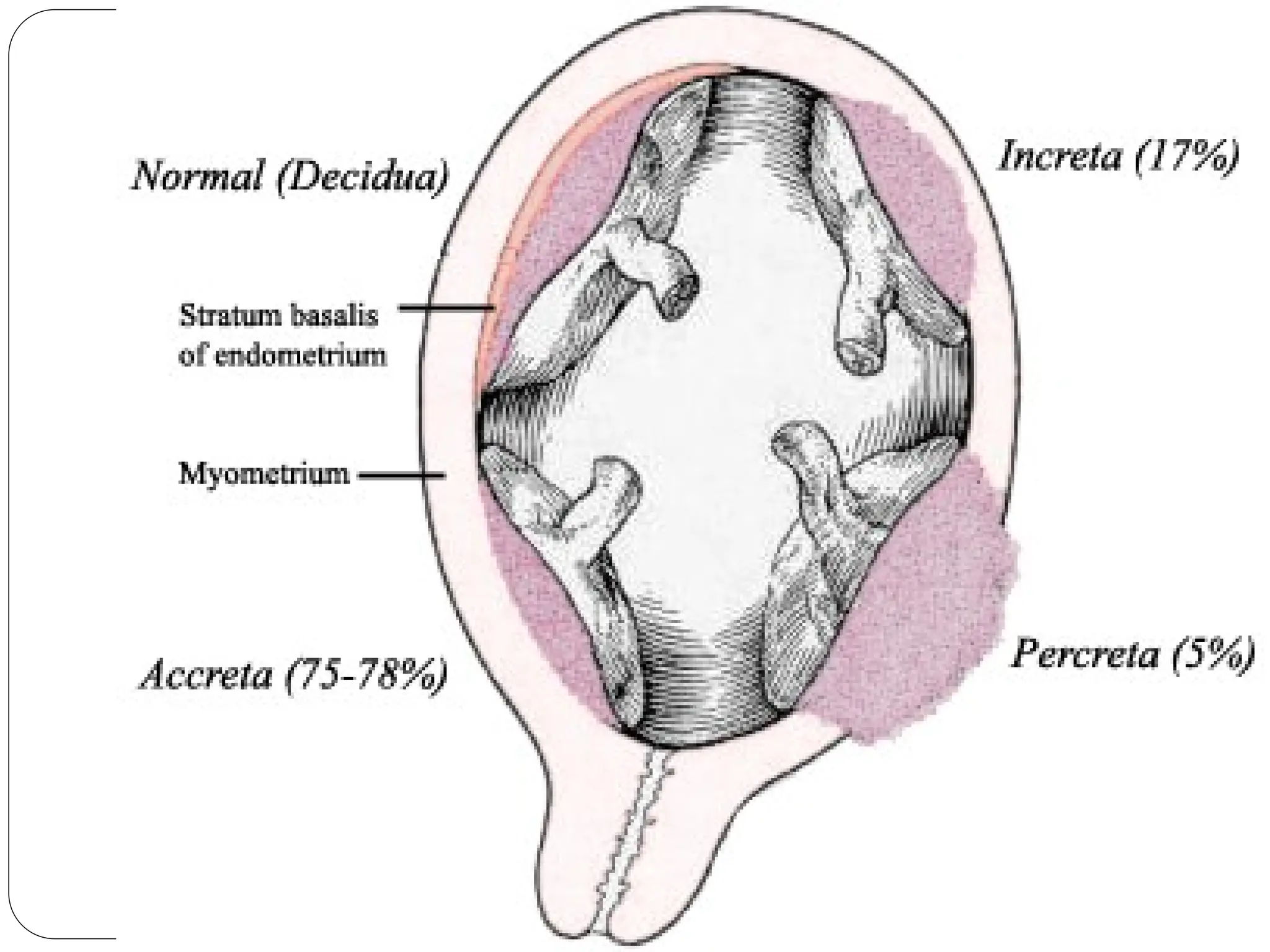
• Placenta accreta – choriomic villi invade up to the
myometrium
• Placenta increta – Choriomic villi invade the myometrium
• Placenta percreta – chronic villi penetrate the whole uterine
wall to the serosal layer.
214.
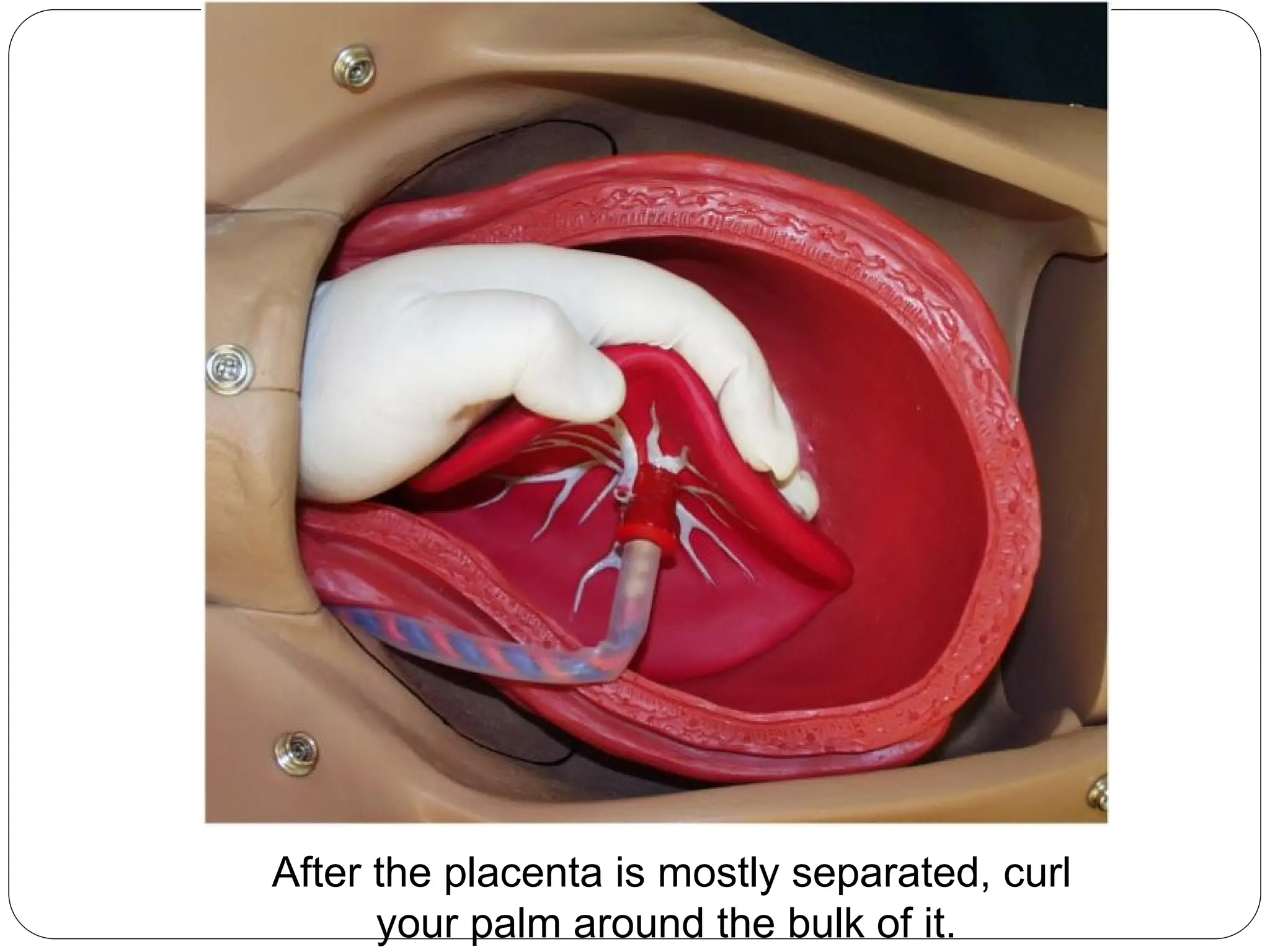
Manual Removal ofthe Placenta
One hand is inserted through the vagina and into the uterine
cavity.
1. Insert the side of your hand in between the placenta and the
uterus.
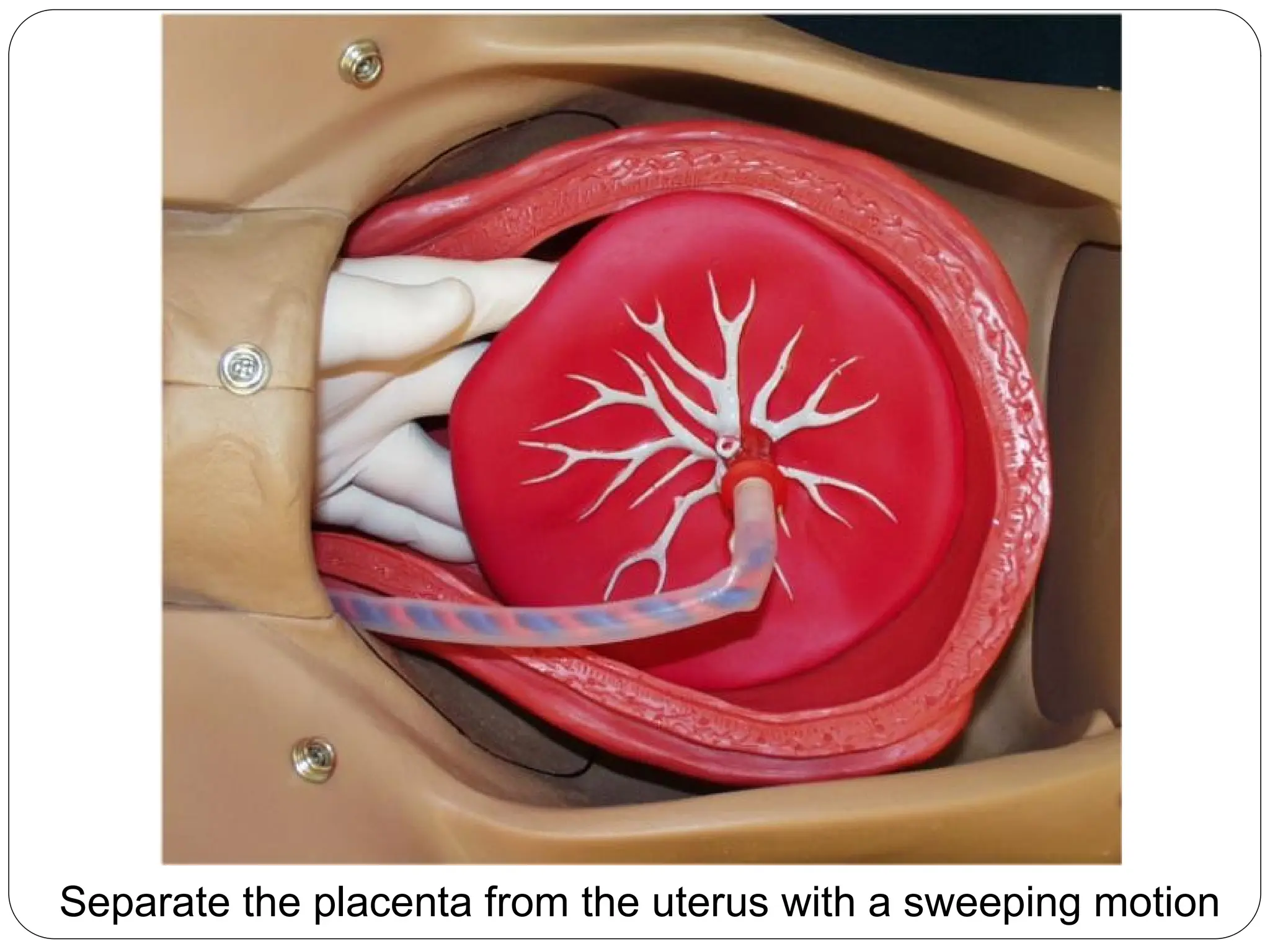
2. Using the side of your hand, sweep the placenta off the uterus.
3. After most of the placenta has been swept off the uterus, curl
your fingers around the bulk of the placenta and exert gentle
downward and outward traction. You may need to release the
placenta and then re-grab it.
4. Then pull the placenta through the cervix. Most placentas can
be easily and uneventfully removed in this way. A few prove to
be problems.
215.
Placenta Accreta andPercreta
When you manually remove the placenta, be prepared to
deal with an abnormally adherent placenta (placenta accreta or
placenta percreta). These abnormal attachments may be partial or
complete.
•If partial and focal, the attachments can be manually broken and
the placenta removed. It may be necessary to curette the
placental bed to reduce bleeding. Recovery is usually satisfactory,
although more than the usual amount of post partum bleeding will
be noted.
•If extensive or complete, you probably won't be able to remove
the placenta in other than handfuls of fragments. Bleeding from
this problem will be considerable, and the patient will likely end up
with multiple blood transfusions while you prepare her for a life-
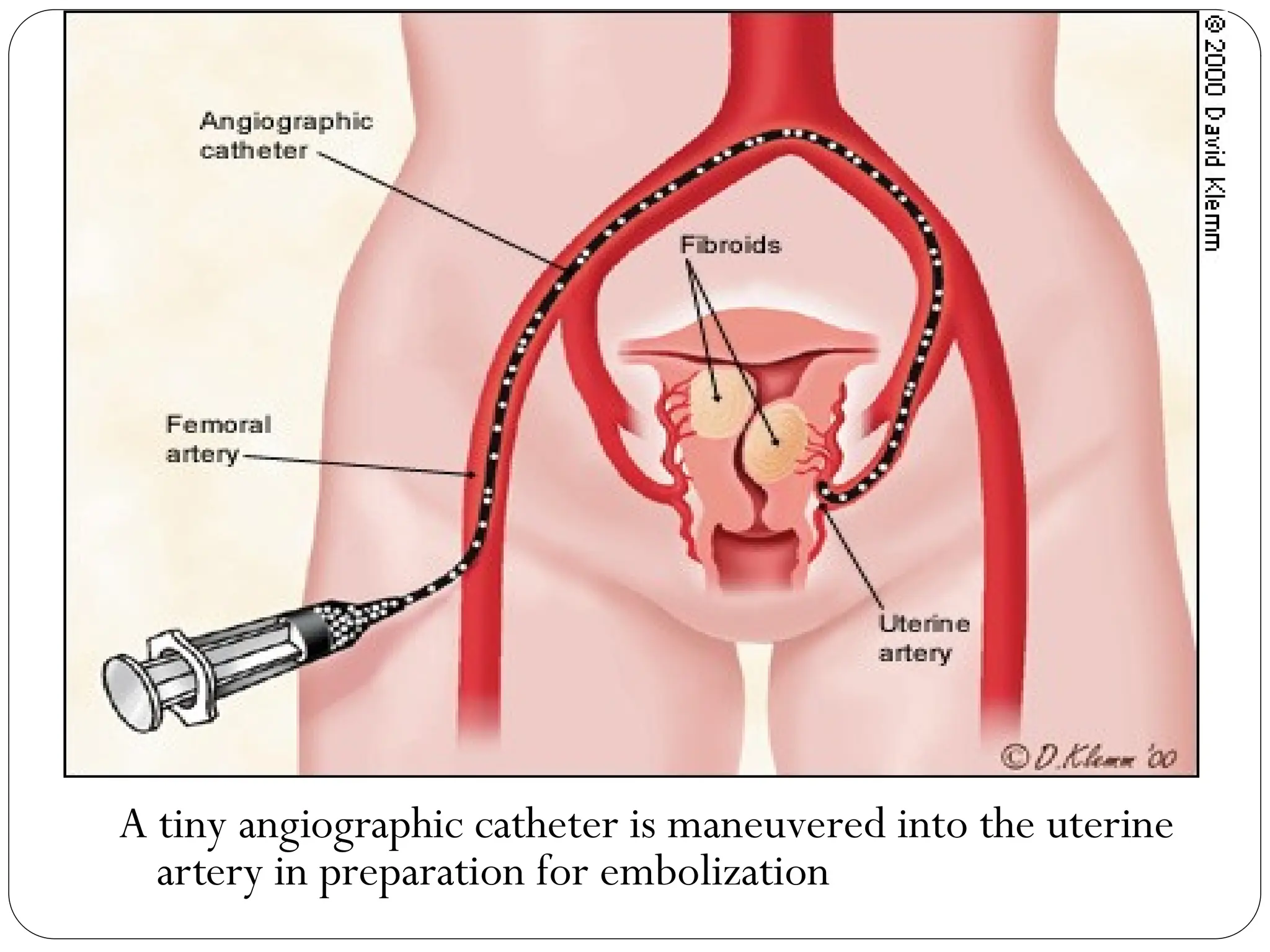
saving, post partum uterine artery ligation or hysterectomy. If
surgery is not immediately available, consider tight uterine and/or
vaginal packing to slow the bleeding until surgery is available.
After the placentais mostly separated, curl
your palm around the bulk of it.
218.
Continue to graspthe placenta as you remove it
from the uterine cavity
219.
RETAINED PLACENTA ONHOME DELIVERY:
• Prophylactic IV ergometrine or inj. Ergometrine 0.5mg and
oxytocin 5 units IM controlled cord traction on birth of baby
placenta is delivered.
• If the nurses are trained she can do manual removal under
injection diazepam IV 10-20mg.
• If she is not trained, patient is sent in a transport to the nearest
health unit.
• ANM accompanies the patient during transport.
• IV fluid on flow.
• At hospital, manual removal is done early on resuscitation of
the patient.
• Adequate blood transfusion is given.
222.
Definition
Placenta accreta occurswhen there is a defect of
the decidua basalis, in conjunction with an
imperfect development of the Nitabuch
membrane (a fibrinoid layer that separates the
decidua basalis from the placental villi)
resulting in abnormally invasive implantation
of the placenta
The ACOG committee
223.
According to Mudhaliarand Menon
Placenta accreta is defined as the abnormal adherence,either in
whole or in part,of the afterbirth to the unlying uterine wall.
According to D.C.Dutta
Placenta accreta in extremely rare form in which the placen is
directly anchored to the myometrium partially or completely thout
any intervening decidua.
225.
Incidence
From 1930to 1950--one case in 30,000 deliveries.
From 1950 to 1960, one in 19,000, deliveries.
by 1980 to one in 7,000.
the incidence has now risen to one in 2,500
deliveries
The ACOG committee
226.
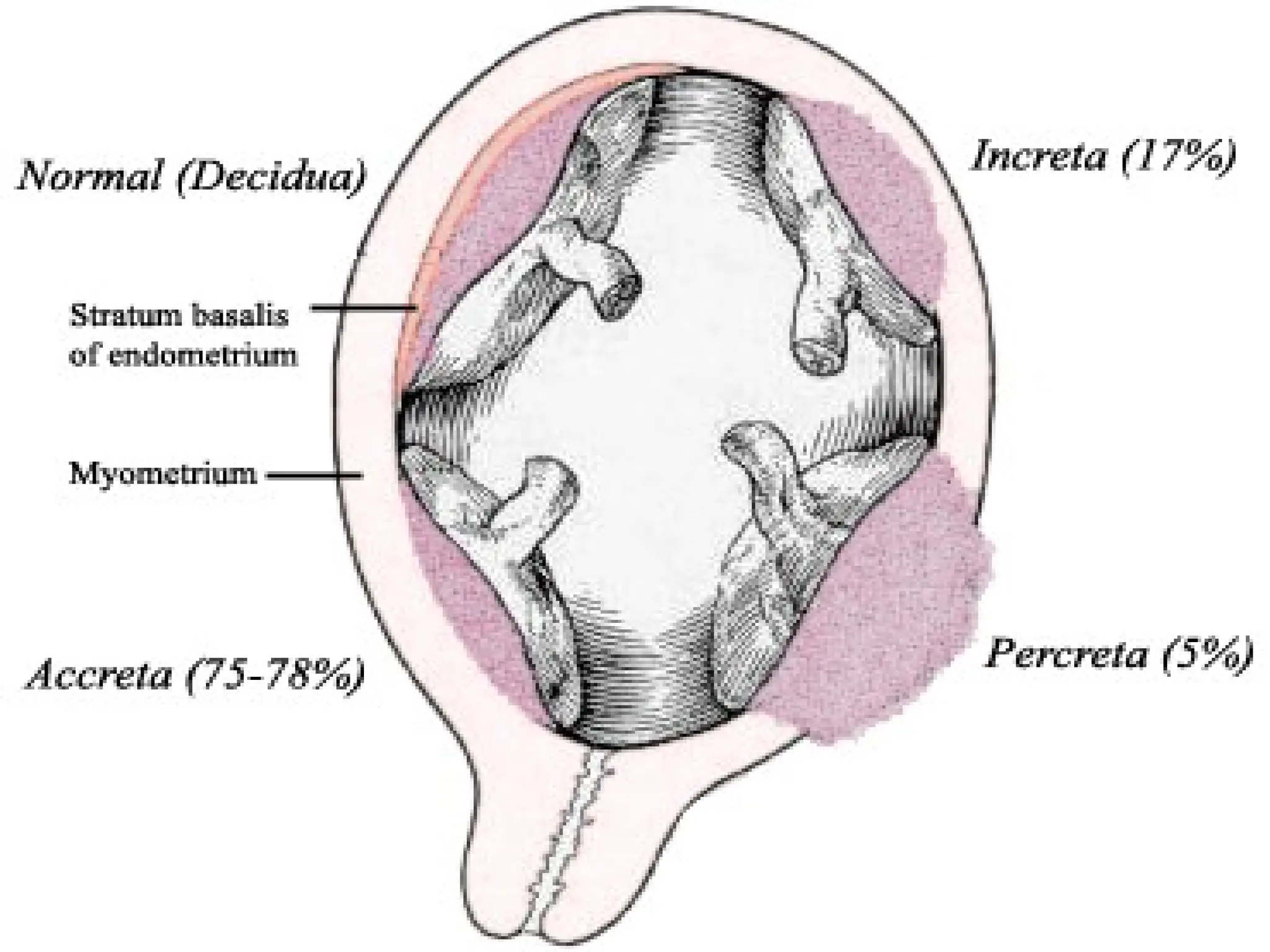
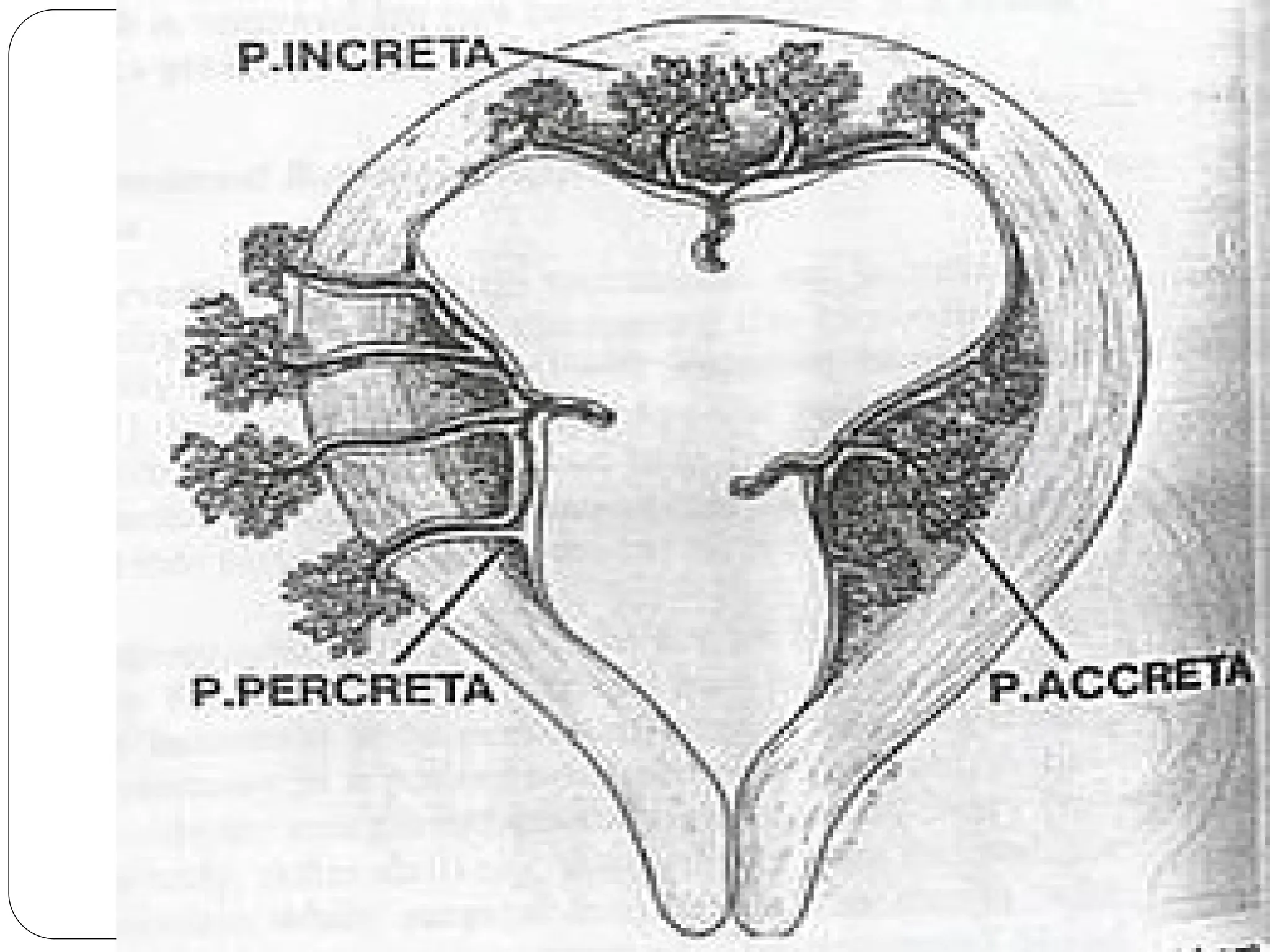
Degrees of severity/Types of Placenta
Accreta
(1) Accreta, in which the placenta adheres to the myometrium
without invasion into the muscle.
(2) Increta, in which it invades into the myometrium.
(3) Percreta, in which it invades the full thickness of the uterine
wall and possibly other pelvic structures, most frequently the
bladder.
229.
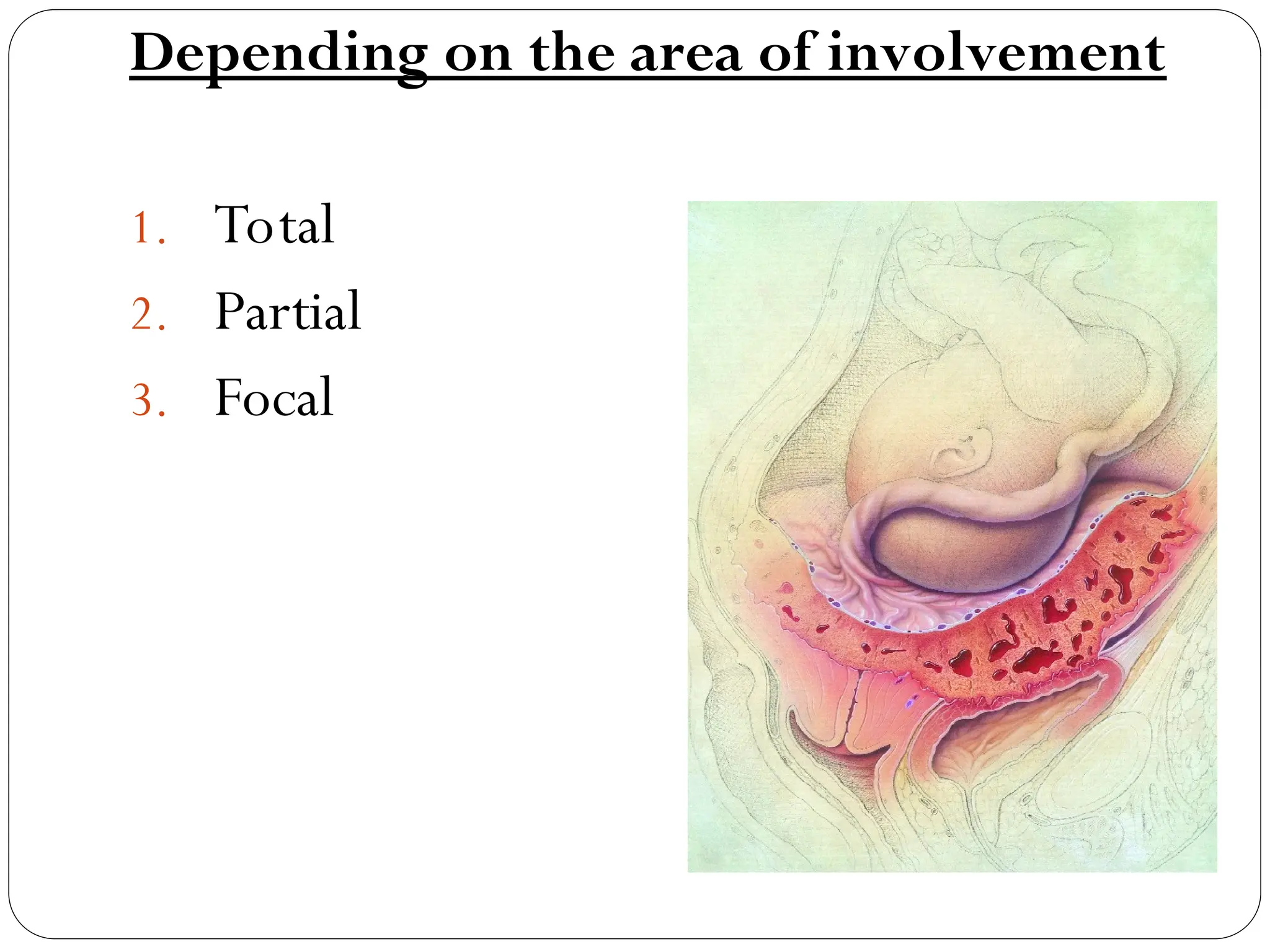
Depending on thearea of involvement
1. Total
2. Partial
3. Focal
230.
Risk factors
Placenta previawith or without previous
uterine surgery.
previous myomectomy.
previous cesarean delivery.
Asherman's syndrome.
submucous leiomyomata.
maternal age of 36 years and older.
231.
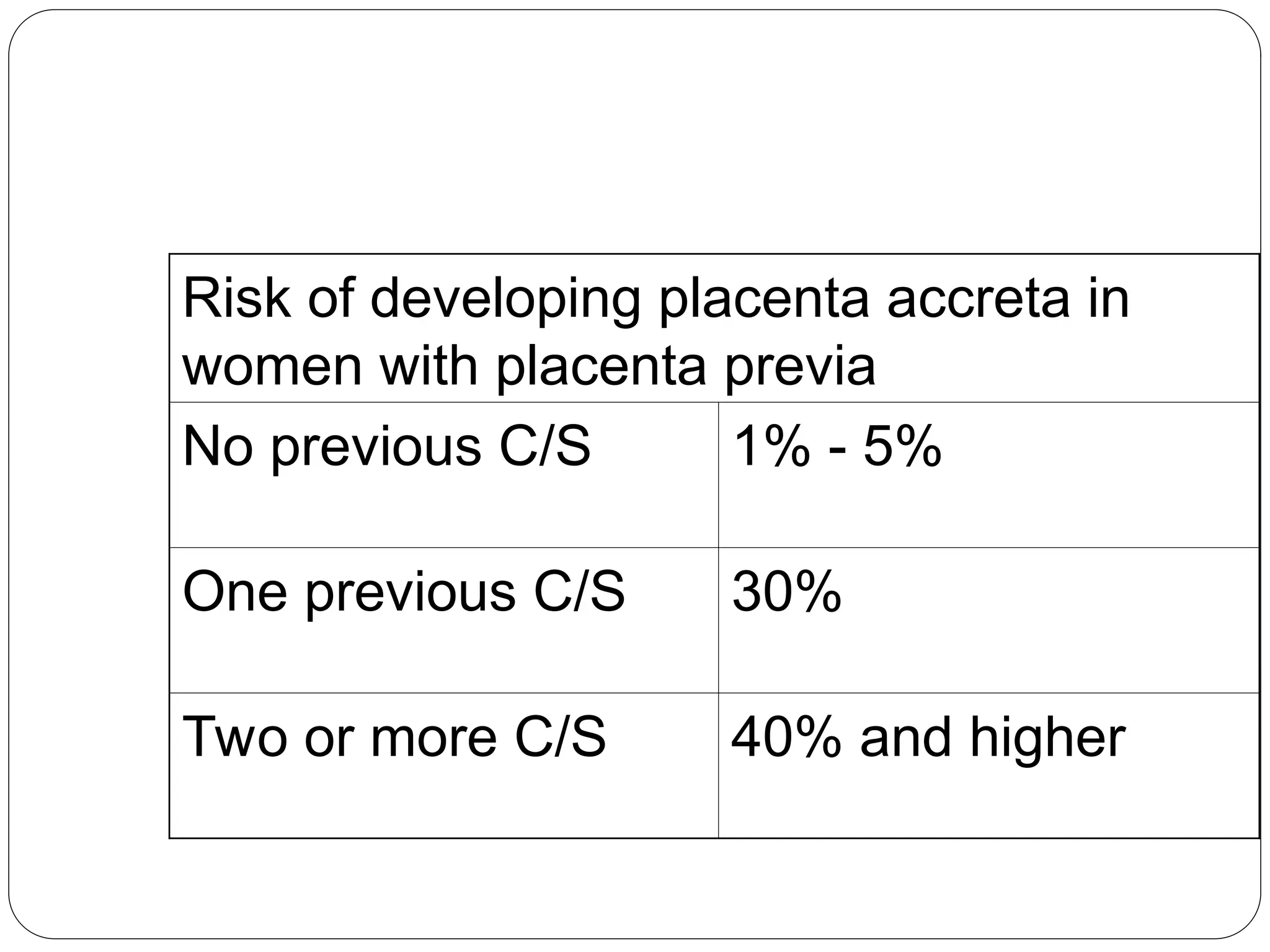
Risk of developingplacenta accreta in
women with placenta previa
No previous C/S 1% - 5%
One previous C/S 30%
Two or more C/S 40% and higher
Diagnosis
Ultrasound
loss of thenormal hypoechogenic zone between
the placenta and myometrium
abnormality of the smooth interface between the
uterus and bladder
a Swiss-cheese appearance to the placenta,
pulsatile flow of maternal blood
MRI
DEFINITION
Induction of labourmeans deliberate termination
of pregnancy beyond 28 weeks (Period of viability)
by any method which aims at initiation of labour and
a vaginal delivery.
243.
Indications
Fetal
Maternal
Combined
Post maturity
History ofIUD
DM
IUGR
Rh-isoimmunisation
Unstable lie
Fetal
IUD
Chronic polyhydramnios
Congenital malformations
Maternal
Pre –eclampsia
Minor degree of placenta praveia
Abruptio placenta
PROM
Chronic HTN
Chronic renal disease
Combined
244.
CONTRAINDICATIONS
Contracted pelvisand CPD
Persistent malpresentation
Pregnancy with previous caesarean section
Elderly primigravida
Heart disease
High risk pregnancy with compromised fetus
Pelvic tumour
245.
SUCCESS OF INDUCTIONdepends on
Period of gestation
Case profile
Sensitivity of the uterus
Pre induction scoring
Merits and demeritsof each method
Prostaglandin
Advantages
Effective method in IUD or cases with unfavourable cervix
No antidiuretic effect
Drawbacks
More systemic side effects when used orally or I/V
Hyper stimulation
248.
OXYTOCIN
Advantages
Wider availability
Less systemic side –effects
HAZARDS OF AROM
Cord prolapse
Uncontrolled escape of amniotic fluid
Injury to cervix or presenting part
Rupture of vasapraevia leading to fetal blood loss.
Amnionitis
249.
Injury to theplacenta
Accidental injury to the uterine wall
Injury to the fetal parts especially eye.
Displacement of presenting part
Intra –ammotic infection
Longer induction – delivery interval compared to LRM
250.
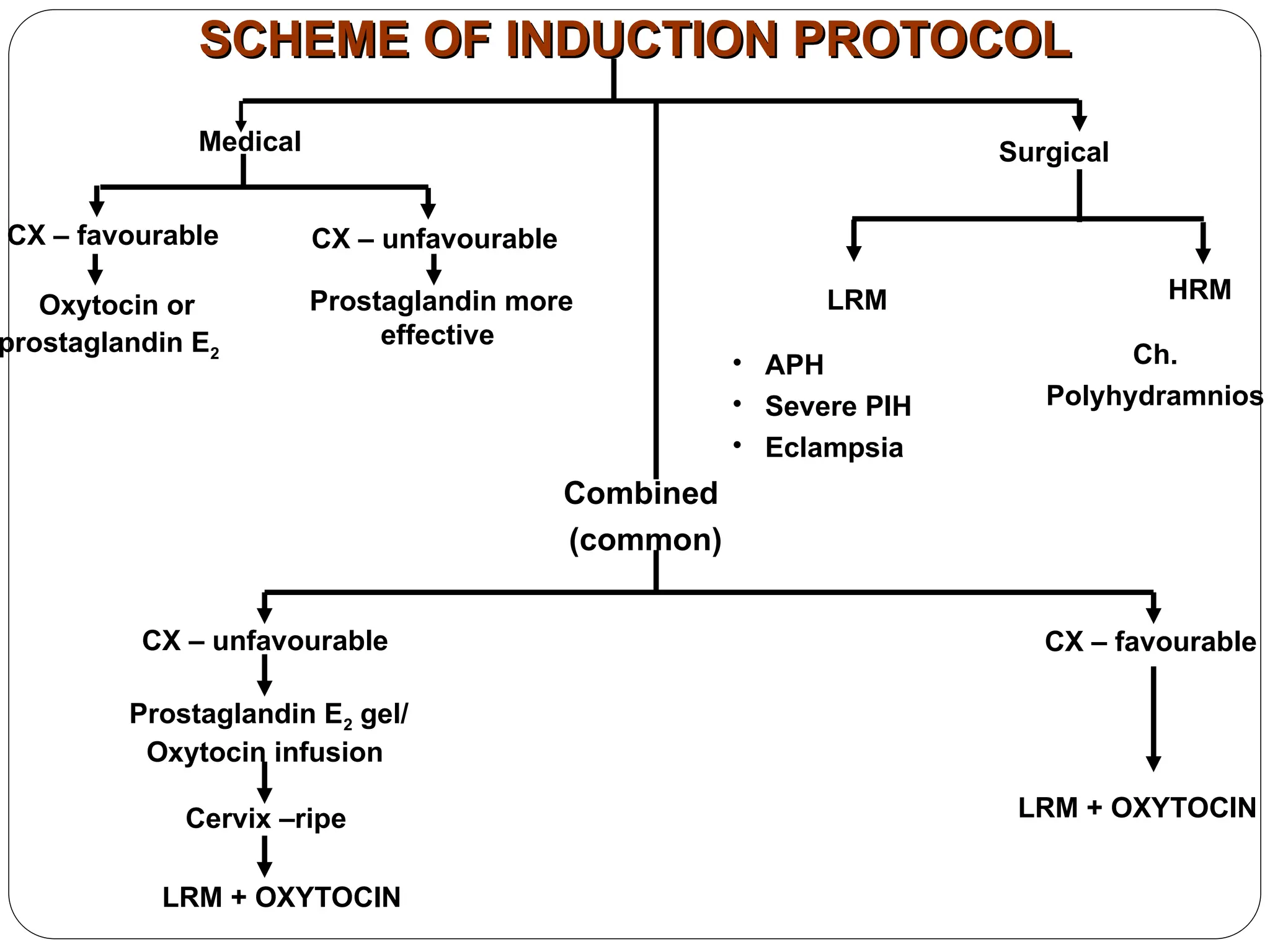
SCHEME OF INDUCTIONPROTOCOL
SCHEME OF INDUCTION PROTOCOL
CX – favourable
Surgical
Medical
CX – unfavourable
Oxytocin or
prostaglandin E2
Prostaglandin more
effective
LRM HRM
• APH
• Severe PIH
• Eclampsia
Ch.
Polyhydramnios
Combined
(common)
CX – unfavourable
Prostaglandin E2 gel/
Oxytocin infusion
Cervix –ripe
LRM + OXYTOCIN
CX – favourable
LRM + OXYTOCIN
251.
NURSING CARE
Technique ofoxytocin administration
Indications for stopping the drip
Nursing measures Consent, explain to the patient
Monitoring
Supervision and recording of findings
Pain relief
252.
Observation
Rate offlow
Uterine contractions
FHR
Progress of labor
Maternal conditions
- Vital signs
- Urine for ketoacidasis
- Intake and output chart
- Watch for prolapse of cord
253.
Observation
Rate offlow
Uterine contractions
FHR
Progress of labor
Maternal conditions
- Vital signs
- Urine for ketoacidasis
- Intake and output chart
- Watch for prolapse of cord
254.
Observation
Rate offlow
Uterine contractions
FHR
Progress of labor
Maternal conditions
- Vital signs
- Urine for ketoacidasis
- Intake and output chart
- Watch for prolapse of cord
DEFINITIONS
Series of eventsthat take place
in the genital organs in an
effort to expel out the viable
products of conception out of
the womb through the vagina
into the outer the world is
called as LABOUR
257.
AUGMENATION OF LABOUR
Inductionof labour means
initiation of uterine contractions
(after a period of viability) by
any method (medical, surgical
and combined) for the purpose
of the vaginal delivery.
ELECTIVE INDUCTION OFLABOUR
Elective Induction Of Labour
means termination of pregnancy
without any acceptable medical
induction. (It is done for the
convenience of the patient,
obstetrician or the hospital.)




![Definition
The labour is prolonged when the combined duration of the
first and second stage is more than the arbitrary time limit
of 18 hours.
[ D.C.Dutta]
Prolonged labour is defined when the first and second
stage of labour last more than 24 hours, currently duration
is taken as more than 18 hours. Duration of labour is
calculated from mother’s subjective estimate of labour
onset
[Dawn]](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-62-2048.jpg)
![Causes of prolonged labour
Faults in power [commonest cause]
*inefficient uterine dysfunction
*constriction ring
*cervical dystocia
*over dose of sedative and analgesics
* epidural analgesia
*improper use of oxytocics](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-69-2048.jpg)
![Cont…
Faults in passenger:
Occipito posterior positions of vertex
Other malpresentations
Twins
Hydramnios[ 30%]](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-73-2048.jpg)
![Labour disorders due to inefficient
uterine action
prolonged latent phase beyond 12 hours
a. Hypotonic or hypertonic dysfunction
b. Predisposing factors are sedation, anaesthesia , false
labour,unknown cause.
Prolonged active phase[ protraction disorder]
Slow rate of cervical dilatation below 1cm/hr in
nullipara and 1.5 cm/hr in multipara
Caused by hypotonic dysfunction, hyperactive lower
segment.
Predisposing factors :CPD,fetal malpositions and
sedation](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-74-2048.jpg)
![Cont…
secondary arrest of cervical dilatation or head descent
Arrest of cervical dilatation is taken when there is no
cervical change for 2 hrs.
there is head descent less than 1cm/hr in nullipara or
less than 2cm/hr in multipara and no head descent for
one hour.
Due to hypotonic dysfunction and incordinate uterine
dysfunction.
The causative factors are occipito posterior positions
[70%], pelvic contraction ,excessive sedation.](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-75-2048.jpg)
![DIAGNOSIS
Clinical features
Hypotonic
dysfunction
[more frequent]
Hypertonic
dysfunction
[ less frequent]
1. Timing of
dysfunction
[more
frequent]
At latent phase
from start of labour
usually running to
active phase
Latent phase from start of
labour
2.Labour pains Less painful, short
lasting,
infrequent
abdominal pain
and no back ache
Severely painful ,prolonged
lasting, frequent pain as
abdominal colic or as
backache ,desire to bear
down during contraction
with incompletely dilated
cervix.](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-76-2048.jpg)







![Monozygotic Twins…
Different Scenarios of Cleavage
If the separation takes place just after the first cellular
division [1st
3 days ]/ prior to morula stage
both of the twins will have their own placenta and an
amniotic sac each.
Scenario 1
Monozygotic twin pregnancy
Di-Amniotic and Di-Chorionic
or D/D](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-126-2048.jpg)
![Scenario 2
Monozygotic twin pregnancy
Di-amniotic - Mono-chorial
and or D/M
Separation can also take place a little
later in the development [4-8 days after
the formation of inner cell mass when
chorion has developed]
of the embryonic cells but before the
blastocyte has defined the roles of each
cell.
Twins will be in the same placenta, but
they will have 2 amniotic sacs.](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-127-2048.jpg)
![Scenario 3
Monozygotic twin pregnancy
Mono-amniotic and Mono-
chorial
Separation takes place at the stage when the amniotic bag is
already being formed
[day 8-14]
Twins will be in the same placenta, and in the same amniotic](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-128-2048.jpg)
![Conjoined Twins
If the division occur after 2 weeks
of the embryonic disc formation,
incomplete or conjoined twins
will occur.
They may be joined
anteriorly [thoracopagus-
commonest],
posteriorly [pyopagus]
cephalic [craniopagus] o
caudal [ischiopagus].](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-129-2048.jpg)
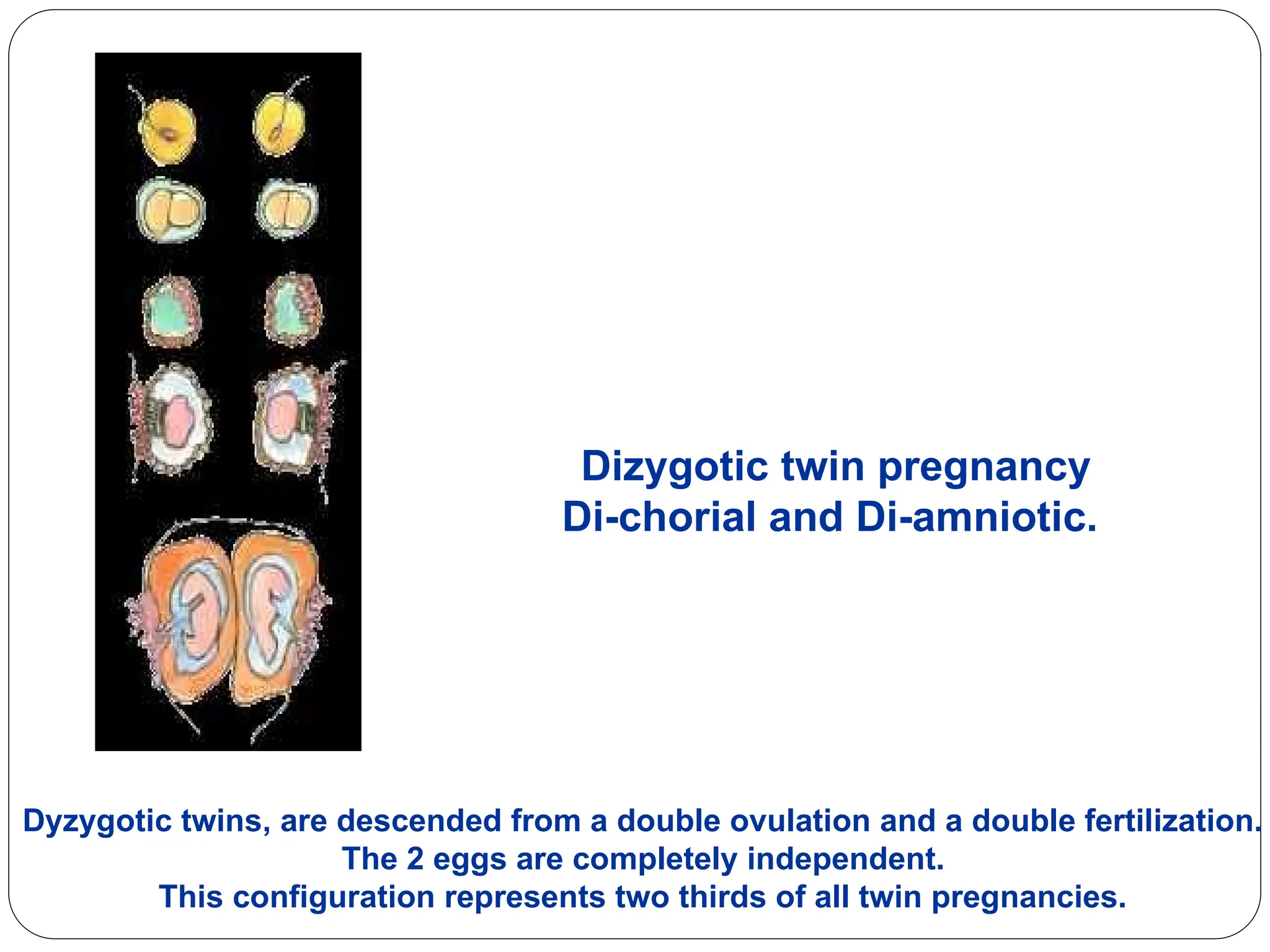
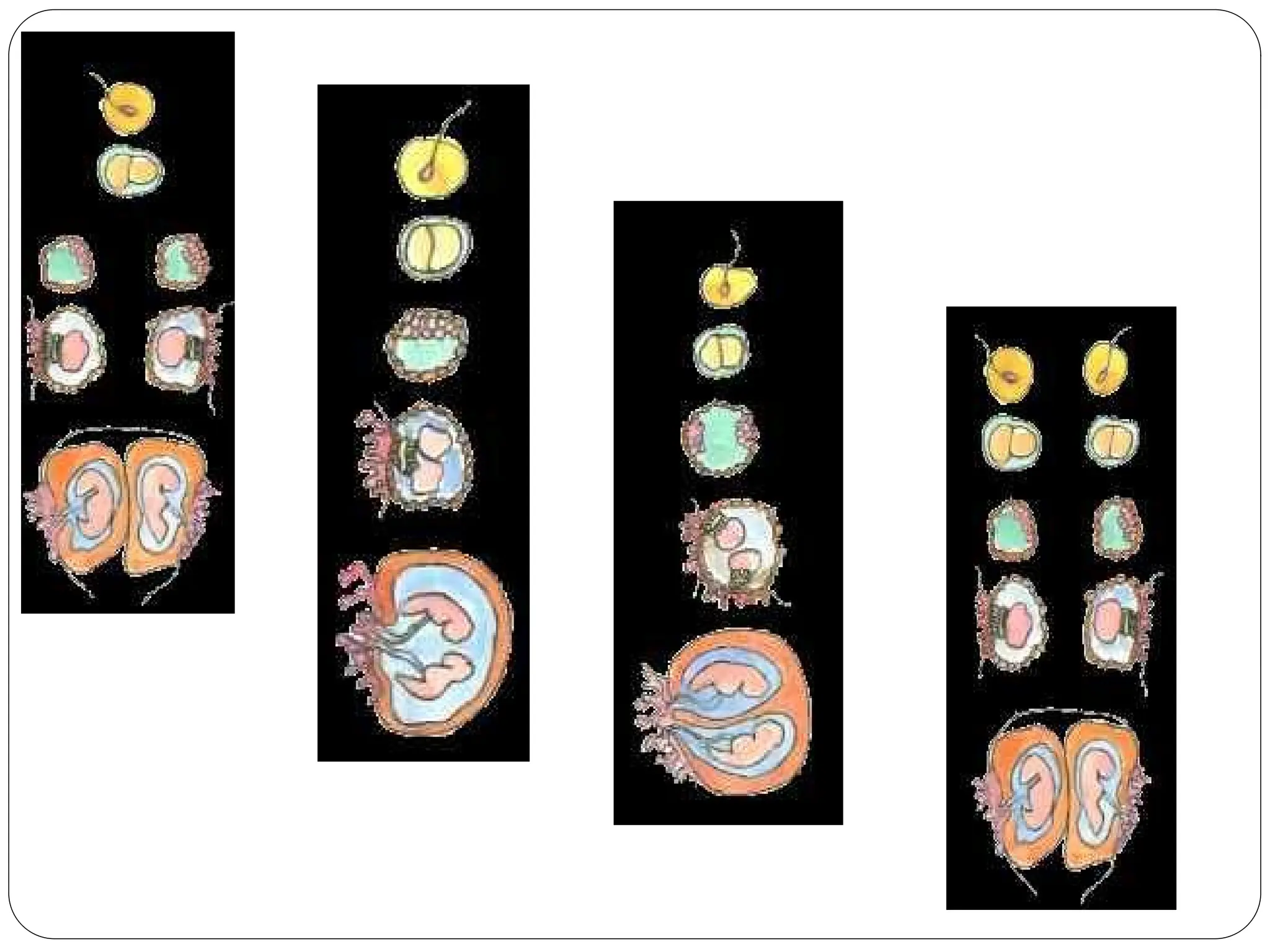
![Examination
General:
An early increase weight gain,
Pallor
Less mid-trimisteric fall blood pressure
Early PIH
Eary edema, and varicose veins in LL.
Abdominal:
Fundal level > amenorrhea especially in mid-pregnancy
exclude other causes.
Palpation: Multiple fetal
identify presentations.
Auscultation of FHS:
2 different recordings by 2 observers and a difference > 10 bpm a Gallop between 2
points[ Arnoux sign]
Pelvic: Specially during the course of labor
small presenting part compared to abdominal size](https://image.slidesharecdn.com/unit1-251009092430-e0f9f262/75/Unit-1-ppt-for-the-studentsbbbbbbbbbbbbbbbbbbbbbbbbb-141-2048.jpg)