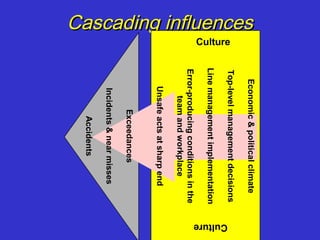
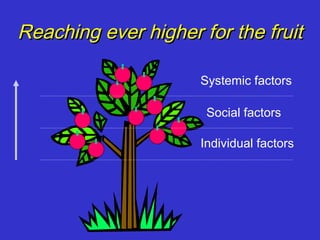
1) The document discusses the history and evolution of error management in complex systems over the past century from a focus on individual factors to increasingly wider systemic and organizational factors.
2) Key events and investigations like Tenerife, Challenger, and Columbia shifted focus to organizational culture and policies in addition to technical issues.
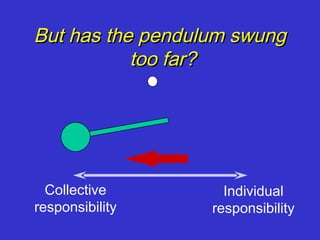
3) However, the document notes concerns that the focus on remote and systemic factors may have swung too far away from individual responsibility and that revisiting individual factors could again benefit prevention efforts.