This document provides information about migraine in women. Some key points:
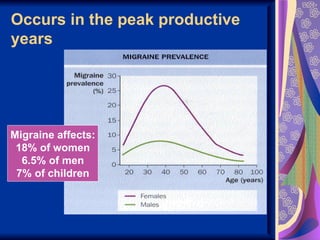
- Migraine is 3 times more common in women than men. Hormonally-associated migraines affect 12 million women in the US.
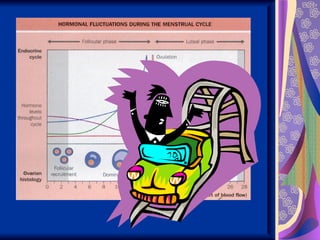
- Migraines are often associated with changes in hormone levels, such as during menstruation, pregnancy, use of oral contraceptives, and menopause.
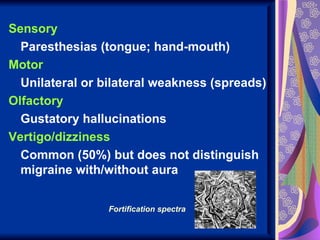
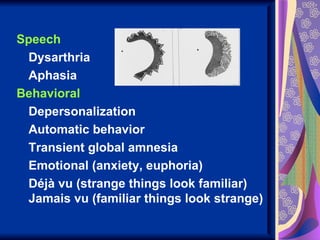
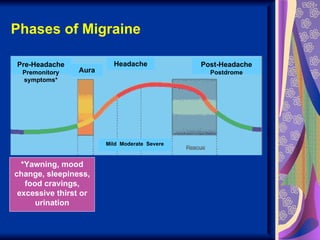
- Diagnosis of migraine involves evaluating symptoms such as headache duration/intensity, nausea, light/sound sensitivity, visual/sensory disturbances (aura).
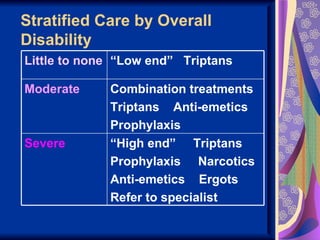
- Treatment involves both acute symptomatic relief and preventive medications, though choices are more limited during pregnancy/breastfeeding due to safety.









![[ppt] RCpsych - Failing medical care of psychiatric patients (vMar11)](https://cdn.slidesharecdn.com/ss_thumbnails/mitchell11-failingmedicalcareofpsychiatricpatientsv3ajmitchell-110307123958-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































