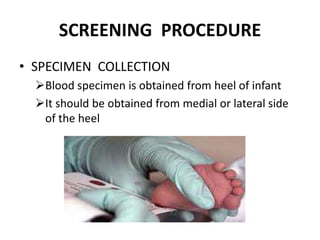
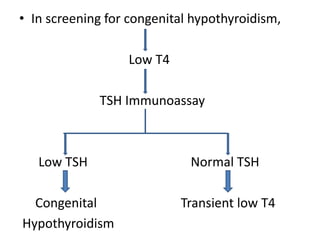
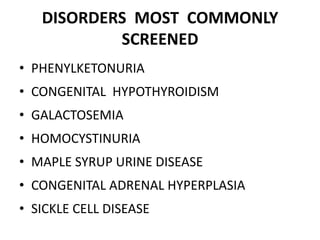
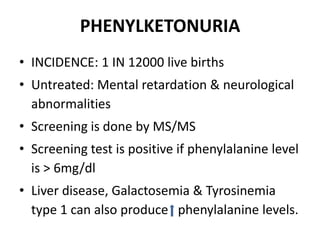
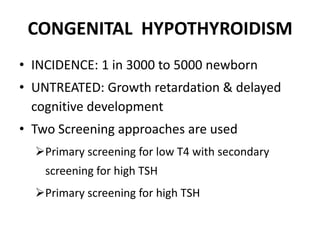


Newborn screening is a public health program that screens infants shortly after birth for treatable genetic or metabolic conditions. The goal is early detection so medical treatment can be promptly initiated to prevent irreversible damage. Conditions commonly screened for include phenylketonuria, congenital hypothyroidism, galactosemia, and maple syrup urine disease. Screening methods have advanced from bacterial assays of individual conditions to tandem mass spectrometry, which can screen for over 50 conditions in a single test.