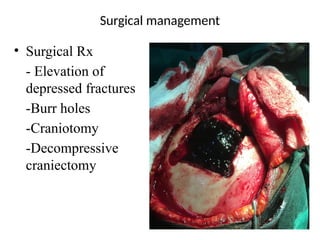
Head injury refers to trauma affecting the scalp, skull, or brain and can lead to cognitive and psychosocial impairments. It is categorized into external and internal injuries, with various causes including vehicle accidents and falls, and types such as concussions and contusions. The document outlines clinical manifestations, diagnostic methods, management strategies, and potential complications associated with head injuries.

![Head Injury
It is an external mechanical injury to the scalp,
skull and/or the brain which can lead to impaired
cognitive or psychosocial/psychomotor functions
or alterations in consciousness.
A head injury is any form of trauma that injures
the scalp, skull or brain.
It is used interchangeably with traumatic brain
injury[TBI]](https://image.slidesharecdn.com/headinjury-240810081543-888780db/85/Presentation-Package-on-HEAD-INJURY-pptx-2-320.jpg)
![INCIDENCE
• Almost 10 million head injury occurs annually in the
united states
• About 4-7million cases is recorded annually in
Nigeria.
• About 20% of which are serious enough to cause brain
damage
• Head injury occurs twice as many in males ,under
35yrs[usually vehicle/motor cycle collision account
are the chief cause of death].[Brindles L.M,Elizabeth
B.2012]](https://image.slidesharecdn.com/headinjury-240810081543-888780db/85/Presentation-Package-on-HEAD-INJURY-pptx-3-320.jpg)
![• Classification by
mechanism of injury
-blunt [closed]
head injury
-penetrating
[open] head injury-
high & low velocity.](https://image.slidesharecdn.com/headinjury-240810081543-888780db/85/Presentation-Package-on-HEAD-INJURY-pptx-11-320.jpg)






























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
