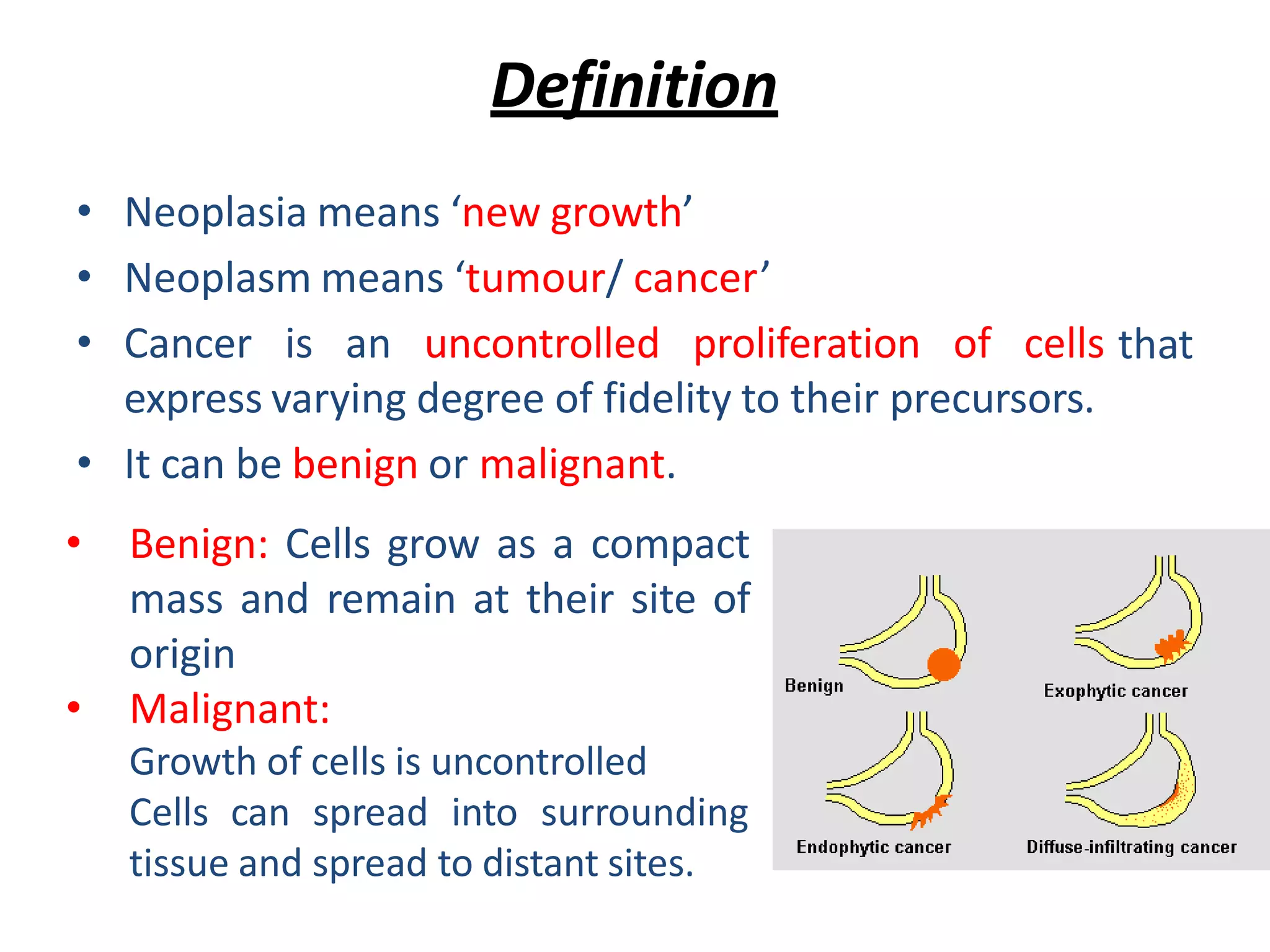
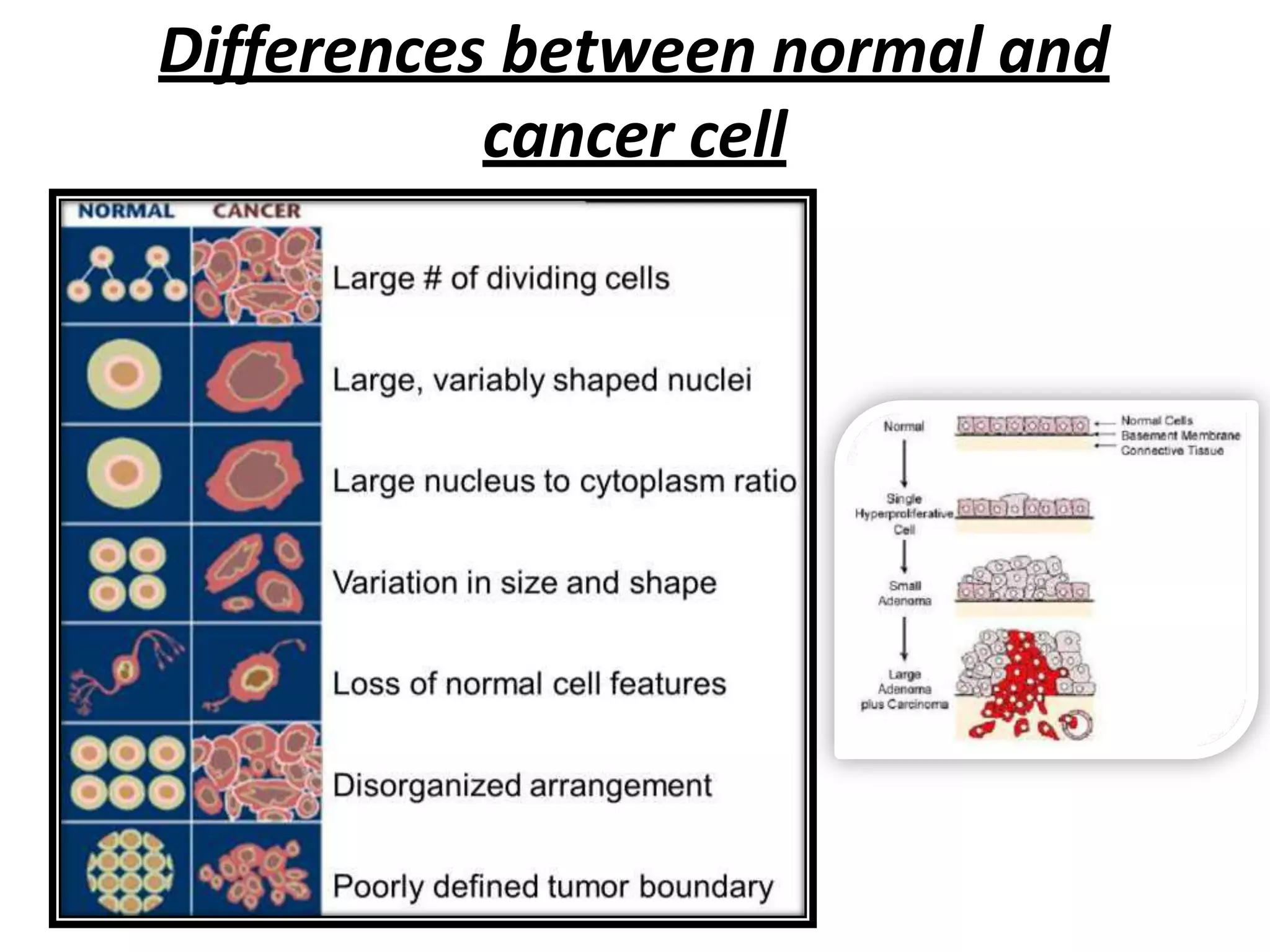
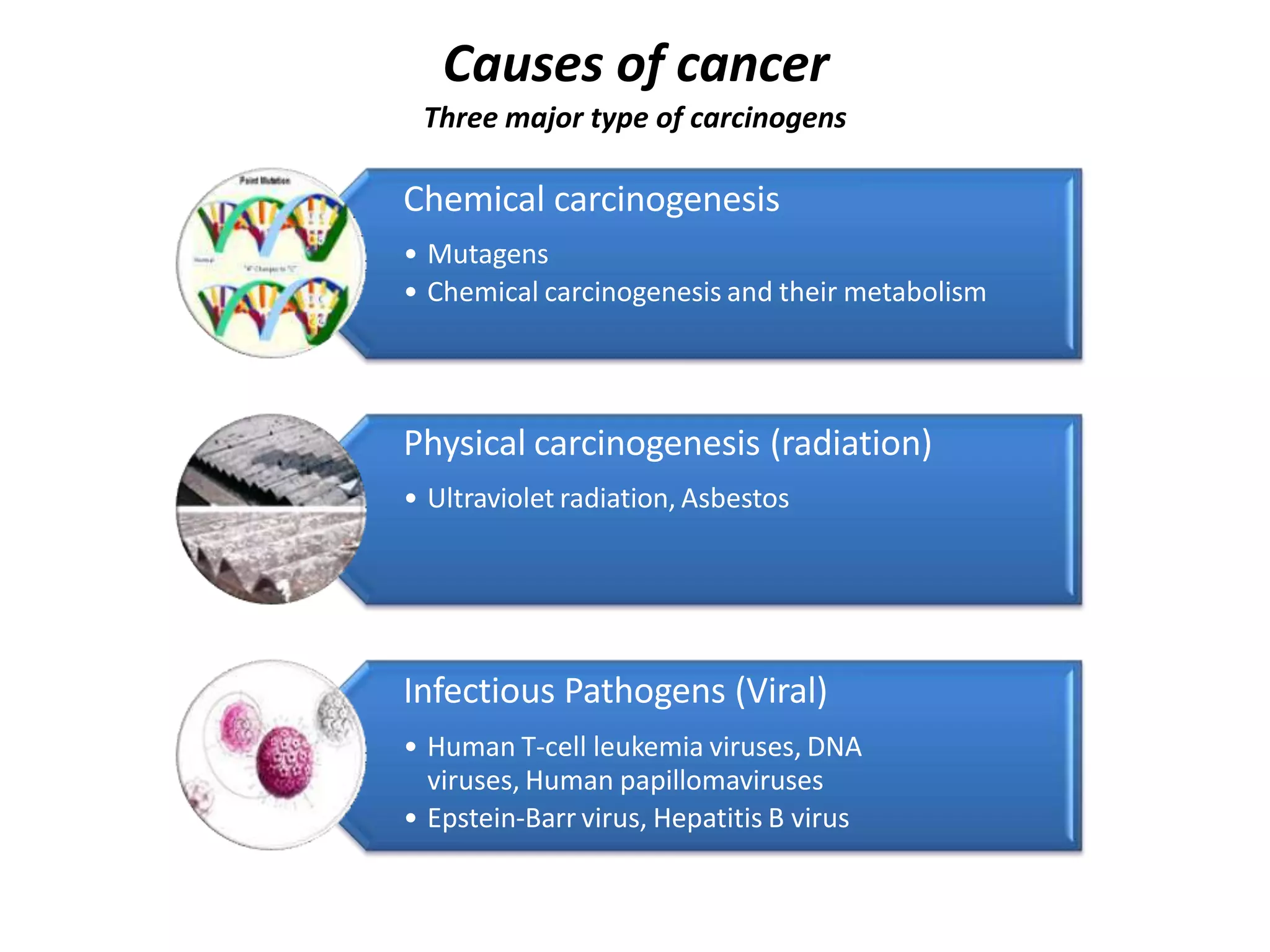
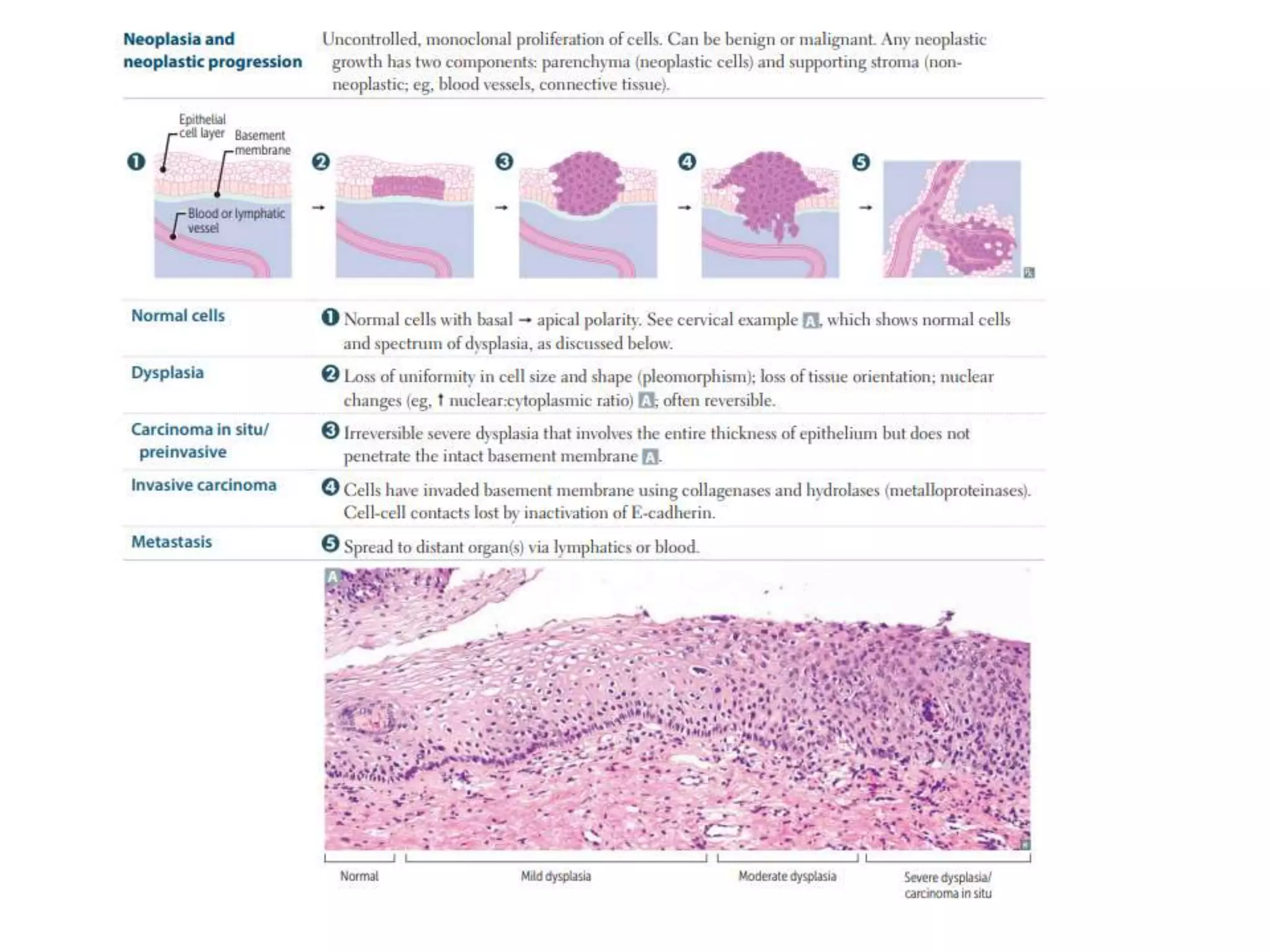
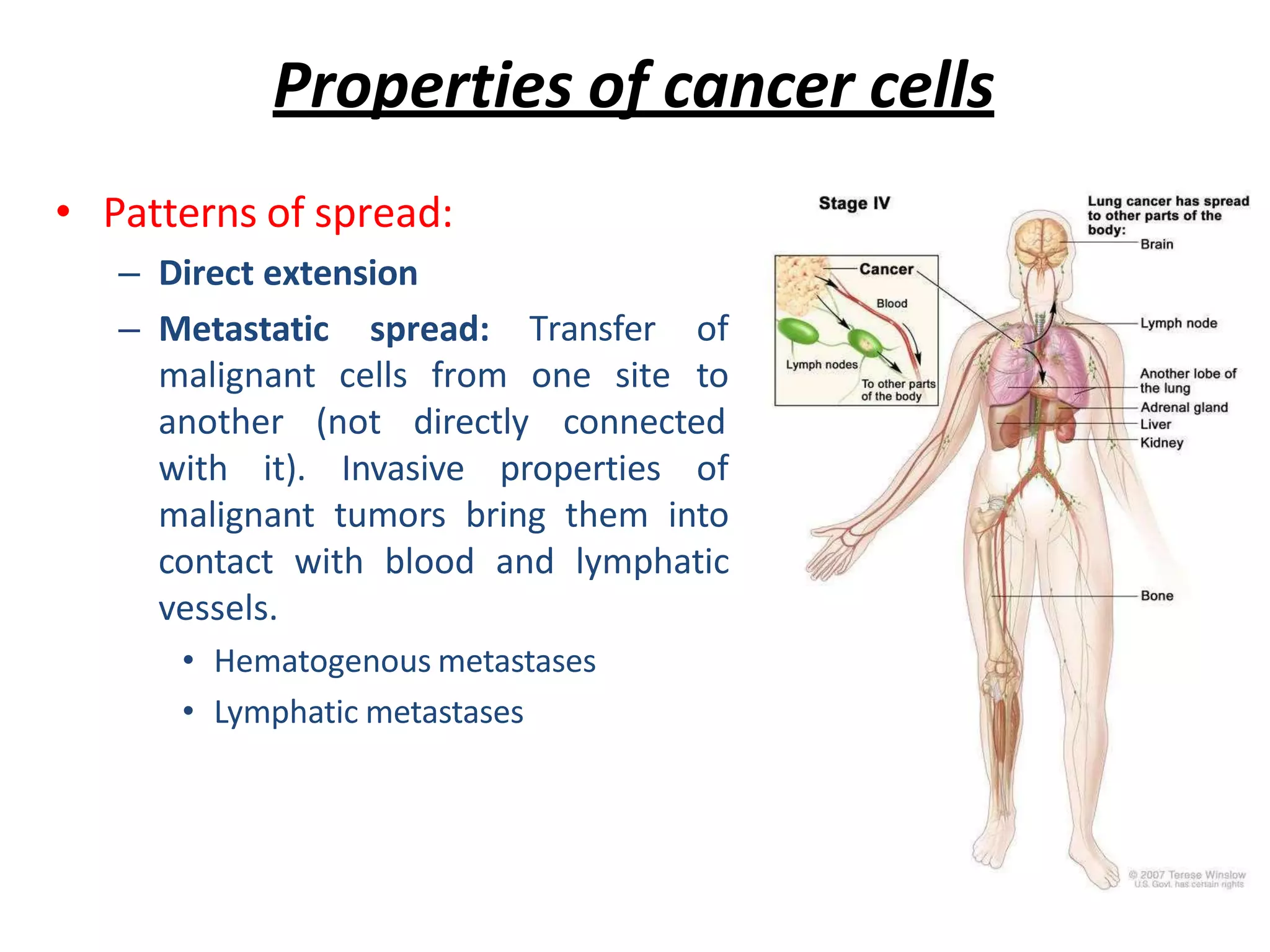
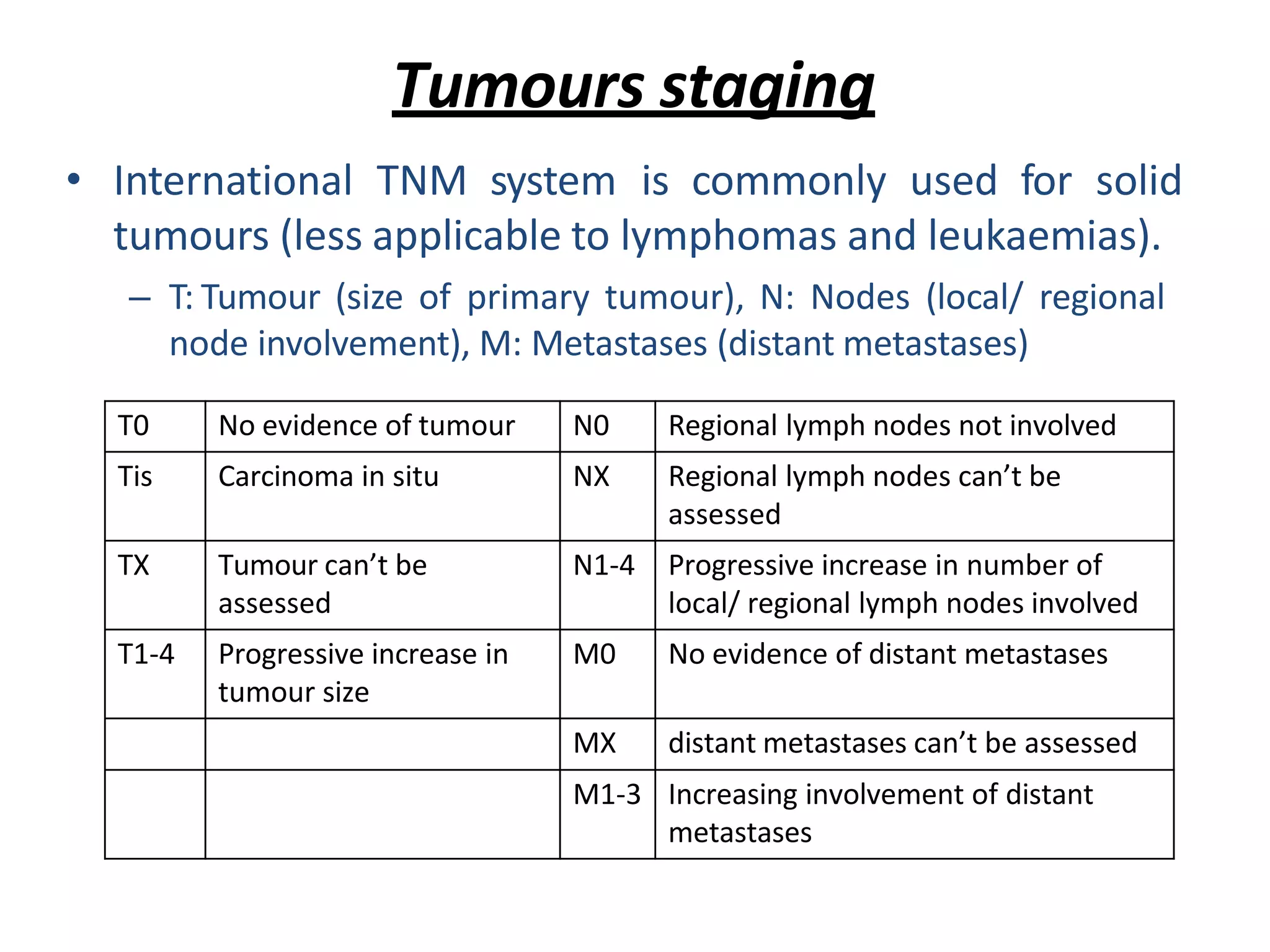
Neoplasms are characterized as either benign or malignant tumors. Benign tumors remain localized and do not invade surrounding tissue, while malignant tumors grow uncontrollably, invade surrounding areas, and metastasize to distant sites. Cancer development occurs through genetic mutations that alter cell growth and behavior over time. Malignant tumors are further classified by their site of origin, structure, and degree of differentiation through grading and staging systems.