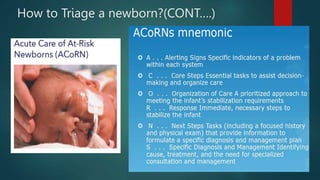
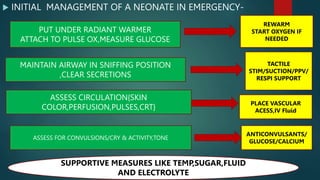
This document discusses neonatal emergencies and how they differ from adult emergencies. It notes that fetal emergencies can begin in utero and involve issues like blood type incompatibility between mother and fetus. Neonatal emergencies are challenging due to infants having limited physiological reserves and non-specific symptoms. A multidisciplinary approach is needed. Recognition and stabilization of sick newborns is important to prevent high morbidity and mortality, as any delays can be detrimental. Scoring systems can help triage infants based on factors like weight and gestational age. The initial steps in stabilizing an infant include addressing temperature, airway, breathing, circulation, and other supportive measures.







































![Neonatal resuscitation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/neonatalresuscitationautosaved-210325082037-thumbnail.jpg?width=640&height=640&fit=bounds)



![Identification ,management & referral of a sick.ppt [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/identificationmanagementreferralofasick-150224064250-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)































