Downloaded 21 times

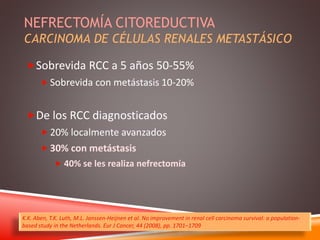
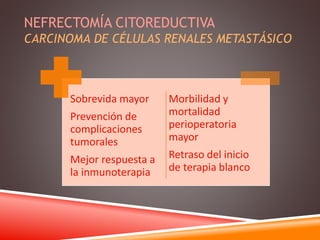
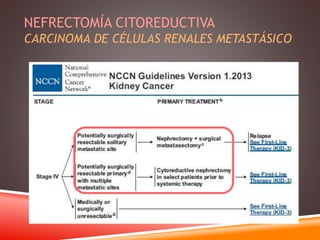
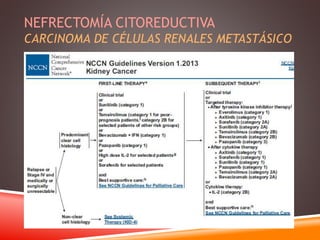
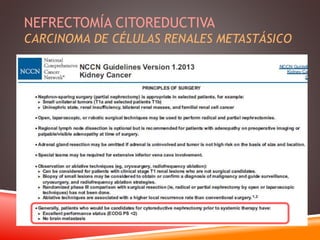
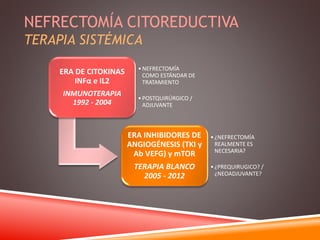
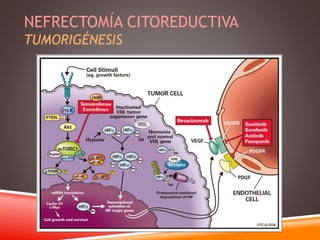
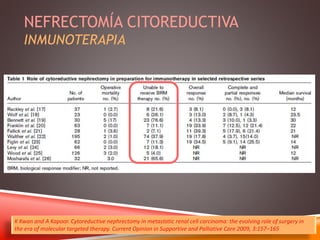
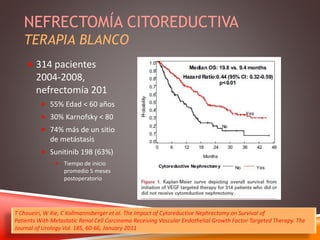
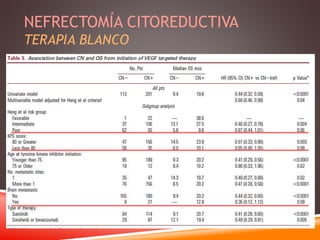
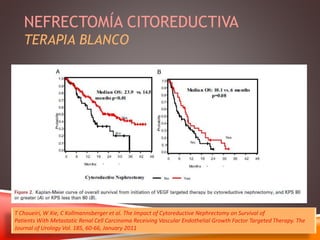
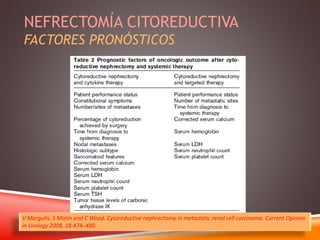
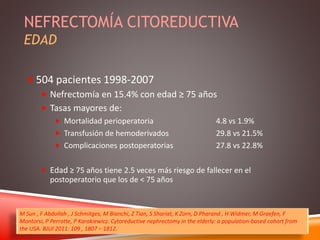
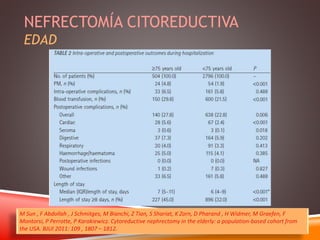
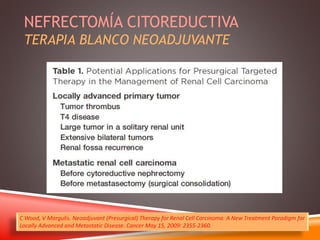
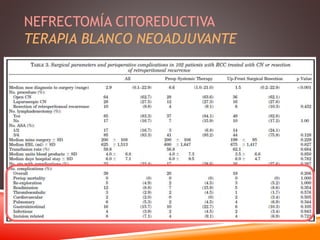
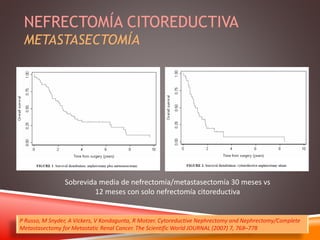
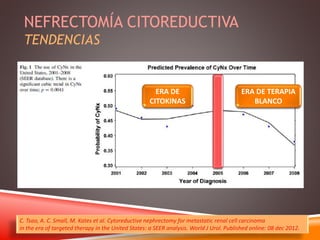
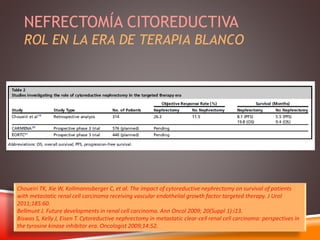
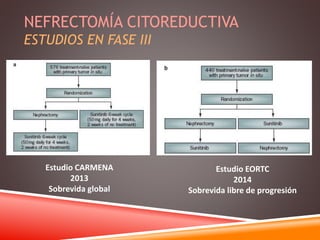

This document discusses cytoreductive nephrectomy for metastatic renal cell carcinoma (RCC), outlining survival rates, treatment approaches, and prognostic factors. It highlights the importance of nephrectomy in improving outcomes and reviews the evolving role of surgery alongside molecular targeted therapies. The document emphasizes risks associated with older patients and explores neoadjuvant therapies as a strategic option before surgery.




























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



