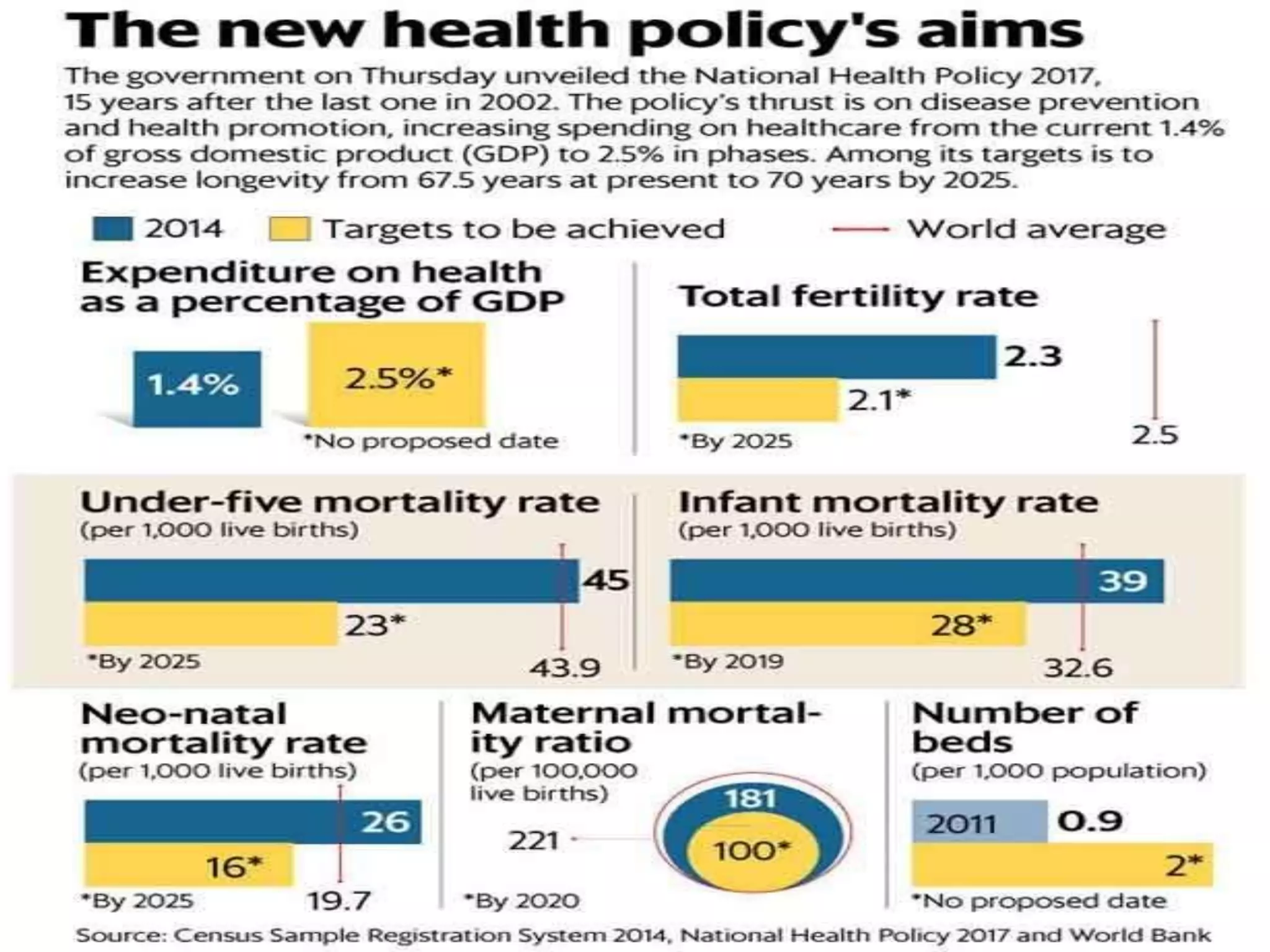
The document discusses India's national health policies from 1983 to 2017. It provides key details on the objectives, goals and quantitative targets of each policy. The National Health Policy of 1983 aimed to attain the goal of "Health for All by 2000 AD" through focus on preventive, promotive and public health aspects. Subsequent policies in 2001 and 2017 continued this aim and set targets to reduce disease burdens and mortality rates, strengthen health systems and increase health expenditure and infrastructure by certain dates. The policies adopted extensive stakeholder consultations and sought to achieve universal health coverage through a preventive and promotive healthcare approach.