Mycobacterium tuberculosis is one of the most deadliest disease and infecting many people around the world.
It is most commno in the poor/unhygeine community.
Antigenic structure ofMycobacterium tuberculosis
• The antigenic structure of bacteria is the parts of a bacterial cell that can act as antigens, or
markers that the immune system can recognize: Surface proteins, Capsules, Cell walls, Flagella,
and Toxins.
• The antigenic structure of Mycobacterium tuberculosis (MTB), the causative agent of tuberculosis,
is complex and plays a crucial role in its interaction with the host immune system. The structure
includes a wide range of antigens, which play key role in both the immune response and vaccine
development. Some of the antigenic structure are as follows:
1. Cell wall antigen: The cell wall of MTB has unique property and contains many immunogenic
components that contribute to its pathogenicity and immune recognition.
• Mycolic acids: MTB cell wall contain long chain fatty acids chains known as mucolic acids,
which makes bacteria less susceptible to antibiotic and also paly major role to hide
bacteria from host immune response and allow bacteria to grow inside macrophages.
3.
Continue….
• Lipoarabinomannan (LAM):LAM is a glycolipid which is a potential virulence factor of MTB and is the
heat-stable that can inhibit monocyte functions and regulate the immune response in the host.
According to WHO LAM can be used to diagnostic method of TB in HIV patients from the urine
sample of patient’s as it is secreted from the urine.
• Phosphatidylinositol Mannosides (PIM): Phosphatidyl-myo-inositol mannosides (PIMs) are glycolipids
that are a key structural component of the cell envelope of Mycobacterium species. PIM are thought
to be play important role in infection. They facilitate MTB adherence to host cells, promoting
infection. They play a role in modulating apoptosis and autophagy in infected macrophages, favoring
MTB survival. They serve as precursors for more complex glycolipids such as lipomannan (LM) and
lipoarabinomannan (LAM), which are essential for maintaining the structural integrity of the cell wall
and its permeability.
• Arabinogalactan: It is the critical polysaccharide present in the cell wall of MTB and play important
role in structure, function and pathogenicity. Arabinogalactan covalently link the mycolic acid with
peptidoglycan forming the complex known as mycolyl-arabinogalactan-peptidoglycan (mAGP)
complex.
4.
Continue…..
• mAGP cmplexis essential for cell viability and structural integrity. Due to the dense and
hydrophobic nature of cell wall by connection of Arabinogalactan with mycolic acid it limits the
diffusible substances like antibiotic and provide resistance to oxidative enzymatic attacks by host
immune cells.
2. Secreted Proteins (ESAT-6 and CFP-10): ESAT-6 and CFP-10 is a protein secreted by the
bacterium Mycobacterium tuberculosis that are vital to the pathogenesis of tuberculosis. ESAT-
6 is a protein that acts as a virulence factor and T cell antigen. It can disturb macrophage
activation, induce apoptosis, and subvert the host's immunity. CFP-10 is a protein that acts as a
chaperone for ESAT-6. It has no direct biological activity, but it may contribute to neutrophil
recruitment and activation during infection. The ESAT-6 and CFP-10 proteins form a 1:1 complex
that binds to the surface of macrophage and monocyte cells. This binding may modulate host
cell behavior to the pathogen's advantage.
5.
Virulence factor ofMycobacterium Tuberculosis
• Virulence factor play major role in causing disease by MTB. Some of the virulence factor are as
follows:-
1. Cell wall component as described above.
2. Trehalose-6, 6-dimycolate (TDM): It is the cord factor of mycobacteria and has been long
known to be major virulence factor of MTB. TDM causes granuloma formation, influence
immune responses, and inhibit tumor growth. It also promotes MTB survival by decreasing
phagosomal acidification and phagolysosomal fusion in macrophages
3. Phthiocerol dimycocerosate (PDIM) and Phenolic glycolipids (PGL): PDIM and PGL include a
group of related cell wall lipids, non-covalently bounded to the mycobacterial surface. PDIM
and PGL are major virulence factors of mycobacterium which required for bacterial duplication
during the acute phase. PDIM help to form the pathogen-associated molecular patterns
(PAMPs) that hide the MTB for detection of host innate immune system. PDIM enhances the
MTB to replicate inside the host macrophages and during early stage of infection it create
protective environment with in the host for growth and replication of bacteria.
6.
Continue…..
PGL suppress theproduction of pro-inflammatory cytokines (e.g. TNF-a) which reduces the host
immune response and promote bacterial survival. It also interfere with host pattern recognition
receptors such as toll-like receptor signaling thus decreasing immune activation.
4. Catalase-Peroxidase: It is a key enzyme produced by MTB that plays a dual role in its
pathophysiology. It is involved in oxidative stress defense by converting hydrogen peroxide into
water and oxygen. Similarly peroxidase breaks the organic peroxides which help in bacterial
survival.
5. Superoxide Dismutase (SOD): SOD help to neutralize the reactive oxygen species (ROS)
generated by host immune system as the defense mechanism against MTB. This detoxification
help MTB to survive in macrophages which is the first site of infection. SOD also allow MTB to
escape microbiocidal effect of host immune response and help in intracellular survival and
proliferation of bacteria.
6. Tuberculosis necrotizing toxin (TNT): TNT is a toxin produced by the tuberculosis pathogen,
Mycobacterium tuberculosis that kills infected macrophages.
7.
Continue….
• Inside thehost macrophages TNT exerts its cytotoxic effects by cleaving the essential coenzyme
NAD⁺ (Nicotinamide Adenine Dinucleotide). The NAD+
is important because it help to repair the
damage cell and also help in cellular energy metabolism of host cell. TNT action decreases the
NAD+
which leads to tissue necrosis which create suitable environment for MTB replication.
• TNT necrosis prevents the containment of MTB within granulomas to facilitating bacterial escape
and spread to new host cells. TNT play major role in causing chronic TB and transmission of TB to
new host.
Pathogenesis of Mycobacterium tuberculosis
• The pathogenesis of Mycobacterium tuberculosis is the process by which the bacteria caused
tuberculosis (TB) in the human body. The process involves the bacteria entering the body,
replicating and escaping the immune system. The process occur when a person inhales air that
contains droplet nuclei containing M. tuberculosis.
8.
Continue…….
• The largerdroplets become lodged in the upper respiratory tract (the nose and throat), where
infection is unlikely to develop. However, smaller droplet nuclei may reach the small air sacs of
the lung (the alveoli), where infection may begin.
• When the alveolar macrophages ingested MTB, the bacteria are not killed but multiple inside
macrophages by killing macrophages with the help of CD8 lymphocytes. Infected macrophages
releases cytokines (e.g. TNF-a, IL-2) that releases other immune cells like neutrophils, monocytes,
and lymphocytes to the site. These immune cells clump together and create tiny nodules at the
site of infection which is known as granuloma.
• The central part of the granuloma may undergo caseous necrosis (cheese-like appearance due to
necrotic tissue). The combination of live bacilli, immune cells and necrotic tissue, all together
form the ghon focus.
• When theses infection spread to the regional hilar lymph nodes, a Ghon complex is formed. The
Ghon complex is consist of Ghon focus and enlarged and caseous hilar or paratracheal lymph
nodes due to the spread of bacteria through lymphatics. All these occur in primary tuberculosis.
10.
Continue…..
• Latent tuberculosis:It is also known as latent tuberculosis infection (LTI). It occurs when a person
is infected with Mycobacterium tuberculosis but does not have active tuberculosis disease. In this
state, the bacteria remain dormant in the body, and the individual is asymptomatic and non-
contagious.
• However, latent TB can reactivate and progress to active TB, particularly in individuals with
weakened immune systems. According to WHO, 2021, about 23% of world’s population have
suffered from the latent tuberculosis.
• As the MTB enters inside the targeted organ, immune system of the host covers the bacilli by
forming granuloma. The bacilli seems to be metabolically inactive but remain viable.
• Active tuberculosis: Active tuberculosis is a serious infection which occur after the inhalation of
Mycobacterium tuberculosis droplets. The primary site of infection is lungs and also known as
pulmonary tuberculosis. The pattern of infection is similar as the primary tuberculosis infection.
11.
Continue…..
• When theactive tuberculosis moves out of the lungs such as lymph nodes, bones, central
nervous system or gastrointestinal, it is known as extra pulmonary tuberculosis.
• The spread of extra pulmonary tuberculosis occurs when TB bacteria comes in contact with
blood, with the help of lymphatic system, by invading tissues of lungs TB bacteria can enter to the
adjacent tissues. It may enter to the spine causing the Pott’s disease (TB of vertebrates).
12.
Continue……
Some of theactive tuberculosis are mention below:
• Tuberculosis meningitis: Tubercle bacilli reach the meninges with the blood. Tuberculosis
meningitis occurs more frequently in non-immune infants and young children as a complication of
primary tuberculosis but it can occur at any stage. The condition is often fatal unless treated at an
early stage, but acid fast bacilli are difficult to find in cerebrospinal fluid (C.S.F). Lymphocytes are
usually found (neutrophils in the early stages).
• Miliary tuberculosis: Widespread military infection can occur if a site of primary infection
ruptures through a blood vessels and bacilli are disseminated throughout the body. Many small
granulomata are formed which on chest X-ray, look like millet seeds (hence name military
tuberculosis). Patients are often acutely ill with fever but a chronic form of the disease can also
occur. The liver, spleen, and lymph glands may be enlarged and the meninges may also become
infected.
13.
Continue….
• Renal andurogenital tuberculosis: Tubercle bacilli reach the kidneys and genital tract by way of
the blood circulations, usually some years following primary tuberculosis. Renal infection is often
suspected when repeated urine specimens are found to contain pus cells but no organisms are
isolated by routine culture. There may be frequency in passing urine, hematuria, and usually a
recurring fever. Tuberculosis of the genital tract (epididymitis in male, endometrial tuberculosis
on females) can cause infertility and pelvic inflammatory disease.
• Bone and joint tuberculosis: A commonly infected site is the spine which may lead to the collapse
of vertebrate and the formation of cold abscess in the groin. This form of the disease is rare.
Symptoms of Tuberculosis
The symptoms of tuberculosis is mention below as per the site of infections:
1. Latent TB infection:
• Symptoms: Individuals with latent TB do not show any symptoms and are not
contagious.
14.
Continue…..
2. Active TBinfection:
• Pulmonary TB (Lungs): Symptoms include
• Persistent cough lasting three weeks or longer
• Chest pain
• Coughing up blood or sputum
• Fatigue and weakness
• Weight loss
• Loss of appetite
• Fever and chills
• Night sweats these symptoms can be mild for many months, leading to delays in seeking
care and increasing the risk of transmission.
15.
Continue……
Extra pulmonary TB(Outside the Lungs): Symptoms include as per the location, which are as
follows:
• Lymphatic System (Tuberculous Lymphadenitis): Swollen and sometimes painful lymph nodes,
commonly in the neck.
• Central Nervous System (Tuberculous Meningitis): Symptoms are as follows
• Persistent headaches
• Nausea and vomiting
• Mental status changes
• Sensitivity to light
• Skeletal System (Pott Disease of the Spine): Symptoms are as follows
• Back pain
• Stiffness
• Possible neurological deficits if spinal nerves are compressed
16.
Continue…
• Genitourinary System:Symptoms are as follows
• Flank pain
• Frequent urination
• Blood in the urine
• Abdominal TB: Symptoms are as follows
• Abdominal pain
• Ascites (fluid accumulation in the abdomen)
• Altered bowel habits
• Weight loss
• Fever
• A feeling of a lump in the abdomen
• Note: It's important to note that extrapulmonary TB may coexist with pulmonary TB, and symptoms
can overlap. Additionally, individuals with weakened immune systems, such as those with HIV, are at
higher risk for extrapulmonary TB. Early detection and appropriate treatment of TB are crucial to
prevent complications and transmission. If you or someone you know exhibits these symptoms,
especially if there's a history of exposure to TB, it's important to seek medical evaluation promptly.
17.
Laboratory Diagnosis ofMycobacterium tuberculosis
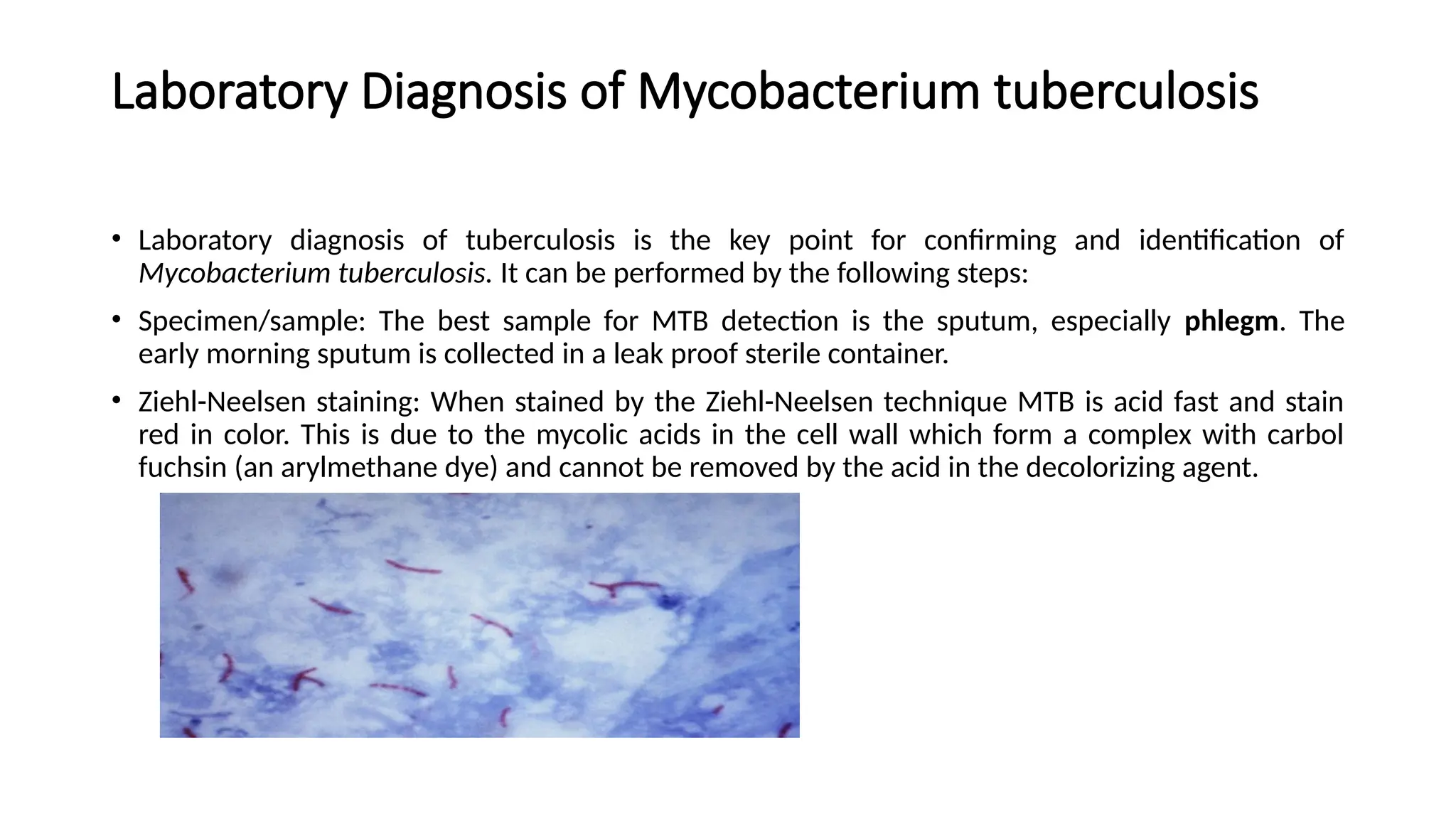
• Laboratory diagnosis of tuberculosis is the key point for confirming and identification of
Mycobacterium tuberculosis. It can be performed by the following steps:
• Specimen/sample: The best sample for MTB detection is the sputum, especially phlegm. The
early morning sputum is collected in a leak proof sterile container.
• Ziehl-Neelsen staining: When stained by the Ziehl-Neelsen technique MTB is acid fast and stain
red in color. This is due to the mycolic acids in the cell wall which form a complex with carbol
fuchsin (an arylmethane dye) and cannot be removed by the acid in the decolorizing agent.
18.
Continue…
• Culture andBiochemical test: Culture and biochemical test of MTB are described above under
morphology.
• Identification of MTB culture:
• Examination of a Ziehl-Neelsen stained smear: To confirm that the organisms is acid fast.
Following culture, the organisms are difficult to emulsify on a slide and are often seen laying
together like pieces of string or cord. This cording is not specific to MTB and may occur to lesser
degree with other Mycobacterium species.
• Testing for pigment production: This is done by leaving the culture in light for 2 hours (avoiding
direct sunlight), reincubating it at 35-370
C overnight and then examining the colonies for the
development if a yellow pigment. Mycobacterium tuberculosis is a nonchromogen, i.e. it does not
produced pigment in light or dark.
• Growth on Lowenstein Jensen medium containing 500µg/ml 4 (p)-nitrobezoic acid, MTB will not
grow on 4 (p)-nitrobezoic acid (PNB) medium.
19.
Molecular Diagnostics:
• NucleicAcid Amplification Tests (NAATs): A nucleic acid amplification (NAA) test is a powerful tool
to assist in the early diagnosis of tuberculosis (TB) and determination of drug resistance. Two NAA
tests are approved by the U.S. Food and Drug Administration (FDA) and are available for testing
respiratory specimens:
a). Hologic Amplified MTD test (GenProbe): Sputum (spontaneous or induced) or bronchial
specimens; patient on anti-TB therapy ≤ 7 days.
b). Xpert® MTB/RIF assay: Sputum (spontaneous or induced) only; patient on anti-TB therapy ≤ 3
days
• NAA testing should be performed on at least one respiratory specimen from each patient with
signs and symptoms of active pulmonary TB disease.
Immunological tests: The type tests are:
• Tuberculin Skin Test (TST): The Tuberculin Skin Test (TST), also known as the Mantoux test, is a
skin test that measures the body's immune response to tuberculosis (TB) bacteria.
20.
Continue……
• The termTB skin test, tuberculin skin test, and PPDs are often used interchangeably. The TST is an
intradermal injection of 0.1 ml of tuberculin (PPD) on the inner surface of the forearm. The skin
test reaction should be read between 48 and 72 hours after administration. The positive result
should increase the swelling about ≥ 10 mm after 48-72 hours of placement.
• People who have been vaccinated with Bacille Calmette-Guérin (BCG) should not be exempted
from TB skin testing. The TST is not used to diagnose TB disease, but rather to identify people
with latent tuberculosis infection (LTBI) who are at risk of developing TB. A false positive reaction
can occur for a number of reasons, including previous BCG vaccination, infection with non-
tuberculosis mycobacteria, or incorrect administration of the test.
21.
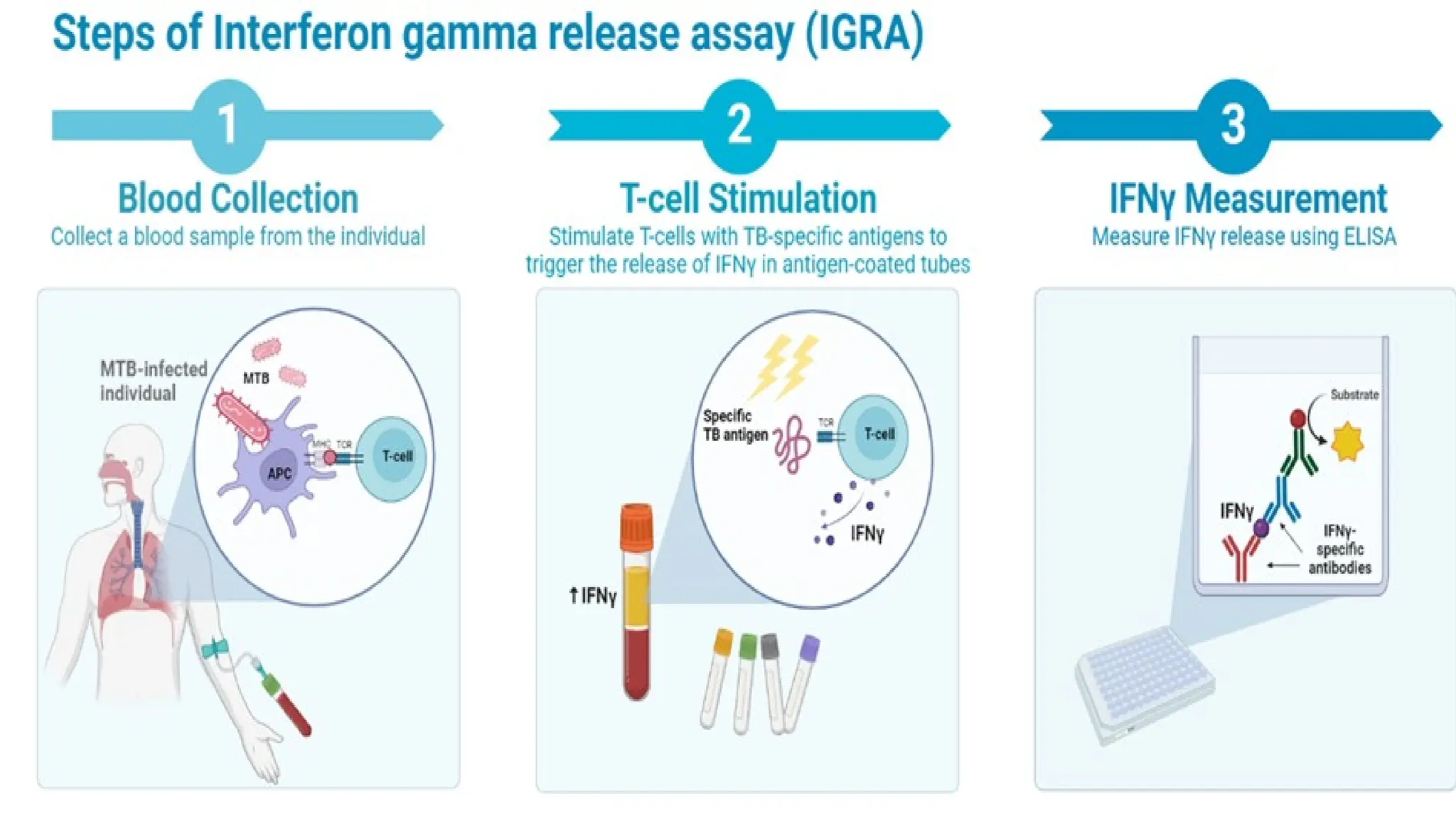
Interferon-Gamma Release Assays(IGRAs):
• Interferon-Gamma Release Assays (IGRAs): It is a blood test that measures the body's immune
response to the bacteria that causes tuberculosis (TB). IGRAs are used to diagnose latent TB
infection, but not active TB disease. For this test patient’s blood is mixed with peptides that
simulate TB antigens, and measures the level of interferon-gamma (IFN-γ) response. The level of
interferon-gamma was measured with the help of ELISA. Positive means the patient has likely
been infected with TB, negative means the patient probably doesn't have TB, and uninterpretable
means the result is indeterminate, invalid, or borderline. The borderline result be repeated. IGRAs
test should performed with in 24 to 48 hours after blood has been collected. The U.S. Food and
Drug Administration (FDA) has approved these two TB blood tests that are commercially available
in the United States:
• QuantiFERON®-TB Gold Plus (QFT-Plus)
• T-SPOT®.TB test (T-Spot)
23.
Drug Susceptibility Testing(DST)
• Drug Susceptibility testing determines which drug kills the tubercle bacilli. If the tubercle can be
killed by the particular drug, they are susceptibility to that drug. If the tubercle can grow in the
presence of particular drug, they are resistant to that drug.
• Multidrug-resistant TB (MDR TB): Resistant to both isoniazid and rifampin.
• Extensively drug resistant TB (XDR TB): is a rare type of MDR TB that is resistant to
isoniazid and rifampin, plus any fluoroquinolone and at least one of three injectable
second-line drugs (i.e. amikacin, kanamycin, or capreomycin).
• Drug susceptibility testing should be done when the patient is first found to have a positive
culture. This is very important to ensure the correct drugs are used. Patients who are treated with
drugs that their TB is resistant will not be cured. This can lead to further drug resistance in the
patient.
24.
Transmission of Mycobacteriumtuberculosis (TB)
• Tuberculosis (TB) is a communicable disease caused by Mycobacterium tuberculosis, primarily
affecting the lungs but capable of spreading to other organs. Understanding its transmission is
critical for prevention and control efforts.
1. Airborne Droplet Nuclei: TB spreads predominantly through the air when a person
with active pulmonary or laryngeal TB expels bacteria by
• Coughing
• Sneezing
• Speaking
• Singing
• The expelled droplets, known as droplet nuclei, can remain suspended in the air for extended
periods. When another person inhales these droplets, the bacteria can reach their lungs and
potentially cause infection.
25.
Continue……
2. Environmental Factors:The risk of transmission increases with close and prolonged exposure to
individuals with active TB, particularly in poorly ventilated environments. Family members, healthcare
workers, and close contacts are at higher risk.
• Poor ventilation and overcrowded settings increase the risk of transmission.
• Enclosed spaces with limited airflow facilitate the accumulation of infectious droplets.
Risk factors for TB
• Individuals that were under the risk of tuberculosis are mention below:
• HIV infection
• Substance use (such as injection drug use)
• Specialized treatment for rheumatoid arthritis or Crohn's disease
• Organ transplants
• Severe kidney disease
• Head and neck cancer
• Diabetes
• Medical treatments such as corticosteroids
• Silicosis
• Low body weight
26.
Continue…..
• Babies andyoung children often have weak immune systems. Children, especially those under
age five, have a higher risk of developing TB disease once infected with TB germs.
Treatment, Preventation and control of TB
1. Treatment: Treatment for MTB infection primarily involves a combination of antibiotics
targeting the bacteria over a prolonged period. Effective treatment depends on the disease
state:
a) Latent Tuberculosis Infection (LTBI): LTBI can be treated by using the first line of medicines. The
first line of medicines are listed below:
• Isoniazid (INH): 6-9 months
• Rifampin (RIF): 4 months
• Isoniazid + Rifapentine: Once-weekly dose for 3 months (directly observed therapy).
b) Active Tuberculosis Disease: This help to cure the patient and stop the spread of transmission.
• First-line drugs: Four-drug as prescribed by medical officer:
1. Isoniazid (INH) 2. Rifampin (RIF) 3. Pyrazinamide (PZA) 4. Ethambutol (EMB)
27.
Continue….
• Treatment phases:
•Intensive phase: First 2 months using all four drugs.
• Continuation phase: 4-7 months using isoniazid and rifampin.
• Drug-resistant MTB (e.g., MDR-TB, XDR-TB) requires second-line drugs like
fluoroquinolones, bedaquiline, or linezolid, often over extended durations (up to 20-24
months).
2. Prevention:
• Vaccination: Only one vaccine is available for TB i.e. Bacillus Calmette-Guérin (BCG). It is
administrated at birth or early childhood in countries with high TB prevelance. It help to protect
against severe forms of TB such as TB meningitis and miliary TB in children. According to the article
published on PUBMED suggested that BCG vaccine reduce the 19% risk of MTB infection after
exposer, compared to unvaccinated children. It also suggested that approximately 81% of exposed,
vaccinated children may still become infected. World health organization (WHO) have given priority
for the development of new TB vaccine that could be more effective than BCG vaccine.
28.
Continue…..
• Preventive Therapy:Types of preventive therapy are as follows:
• Isoniazid Preventive Therapy (IPT) are recommended for individuals with latent TB infection,
especially in high-risk populations (e.g., HIV-positive individuals, close contacts of active TB
cases).
• Infection Control Measures: The way are as follows
• Use of personal protective equipment (e.g., N95 respirators) for healthcare workers.
• Proper ventilation in TB-prone environments.
• Implementation of airborne infection isolation precautions in healthcare settings.
Control:
a) Public Health Strategies:
• Case Detection: Early identification through active case finding and improved diagnostic tools
(e.g., GeneXpert MTB/RIF, culture methods).
29.
Continue….
• Directly ObservedTherapy (DOT): Ensures adherence to treatment regimens, reducing the risk of
drug resistance.
• Surveillance Systems: Monitoring TB cases to identify outbreaks and trends.
b) Community Education: Educating communities about TB transmission, symptoms, and
treatment to reduce stigma and improve health-seeking behavior.
c) Integrated Approaches:
• TB and HIV co-management programs.
• Addressing social determinants of health (e.g., malnutrition, overcrowding) to reduce
vulnerability.
• Directly-Observed Therapy, Short-Course (DOTS) means that the patient taking the medicine
should be observed by a nominated person, and the taking of the medicine should be recorded.
This ensures that the patient takes the medication regularly, which is essential for the medicines
to be effective – and to prevent the bacteria from becoming resistant and the drug from
becoming ineffective. The World Health Organization (WHO) endorses DOTS to improve
adherence to TB treatment. The best way to remember to take medicines is to get directly-
observed therapy. If following the DOTS regimen, the patient will meet with a health care worker
every day or several times a week.
30.
Epidemiology of Mycobacteriumtuberculosis
• According to the World Health Organization (WHO), in 2022 estimated 10.6 million new cases of TB
globally, with 1.6 million deaths. TB became second leading infectious killer after COVID-19. TB is
concentrated in low- and middle-income countries, with the highest burden in Southeast Asia,
Africa, and the Western Pacific regions. The top eight countries (India, China, Indonesia, the
Philippines, Pakistan, Nigeria, Bangladesh, and South Africa) accounted for two-thirds of the global
TB cases in 2022.
• In 2022, an estimated 450,000 new cases of rifampicin-resistant TB were reported globally.
Multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB) are growing concerns.
• The National Tuberculosis Prevalence Survey (TBPS) 2018-19, Nepal's first nationally representative
TB survey, estimated that approximately 117,000 people were living with TB, with around 69,000
new cases developing in 2018. The survey also revealed that TB prevalence is higher among men
and the elderly, and more prevalent in the hills and Terai regions compared to the mountains and
Kathmandu Valley. Despite efforts, a significant gap exists between estimated TB cases and actual
notifications; in 2018, only 32,474 cases were reported, indicating that about 54% of cases were
missed for diagnosis and treatment.
• Drug-resistant TB poses an additional challenge, with only one in three affected individuals having
access to necessary treatment. In 2079/80, the National TB program reported 37,447 TB
notifications, including 694 drug-resistant cases. The concurrent spread of HIV/AIDS, along with the
emergence of multidrug-resistant TB (MDR-TB) and extensively drug-resistant TB (XDR-TB), has
exacerbated the impact of the disease.