2. A 7-year-old boy presents with progressive
weakness of both legs for 4 years.
3.
4.
5. Definition
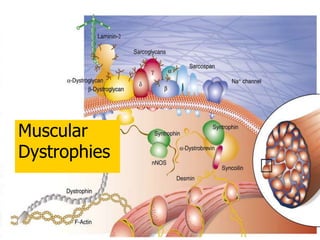
A group of
noninflammation
inherited distroders
progressive
degeneration and
weakness of skeletal
muscles
without cause in
peripheral / central
nervous system
9. DUCHENNE MUSCULAR
DYSTROPHY:
First described in 1881- dystrophin gene
discovered in the early 1980's
Cause: deficiency of dystrophin, resulting in
progressive loss of muscle fibers
X-chromosome linked
Asymptomatic carrier
1 in 3500 live births, occurs in boys, girls are
carriers.
MUSCULAR DYSTROPHY 9
16. DMD: Epidemiology
Most common in male
1:3500 live male birth
1/3 new mutation
65% family history
17. DUCHENNE MUSCULAR DYSTROPHY
Commonest muscular dystrophy
Incidence 1 in 3500 live births
Prevalence 3 in one lakh
X-Linked recessive
Predominantly affects boys
Presents with proximal
muscleweakness
18. DMD: Clinical manifestation
Onset : age 3-6 years
Progressive weakness
Pseudohypertrophy of
calf muscles
Spinal deformity
Cardiopulmonary
involvement
23. Symptoms start by 3 yrs age
Weakness : proximal more than
distal,symmetric
Muscles involved Add.magnus, tendoachilis,
quadriceps shoulders girdles
Course : reduced motor function by 2-3
years
24. CONTRACTURES: Hips, Knees.
SCOLIOSIS: Occurs after loss of ambulation.
CARDIOMYOPATHY: Dilated.After 15 yrs. Age.
MENTAL RETARDATION: 1/3rd have slow
mentation.10-20% have IQ of less than 70.
NIGHT BLINDNESS: Dystrophin in outer
plexiform layer is involved.
MUSCULOSKELETAL:
26. Shows ‘a valley between the two mounts’ behind each
shoulder. The infraspinatus and deltoid muscles (arrow
heads) are enlarged like two mounts and in between
them, all
the muscles forming the posterior axillary fold are
wasted
forming an oval valley (arrrow).
VALLEY’S (or) PRADHAN SIGN (or)
POLY HILL’S SIGN
27. DMD: Diagnosis
Gait
Ober test
Thomas test
shoulder abdction
range is decreased
Macroglossia- large
tongue
IQ ~ 80
Increase CPK (200x)-
creatine phosphokinase
Myopathic change in
EMG
Bx: m. degeneration
Immunoblotting: Absence
dystrophin
DNA mutation analysis
30. MUSCLE BIOPSY IN DMD:
• Lack of immunostaining of dystrophin in muscle biopsy
specimen
• Demonstration of deletion in the dystrophin gene
MUSCULAR DYSTROPHY 30
Normal Duchene dystrophy
40. Duchenne muscular dystrophy rapidly
progressive.
Death usually occurs by age 25.
Typically from respiratory or cardiac failure.
Mechanical ventilation and steroids have
increased
life span.
PROGNOSIS:
42. BECKER MUSCULAR DYSTROPHY
BECKER and KEINER described
in1955.
Other end of the spectrum of DMD.
Dystrophin is reduced in
quantity/quality.
Clinical features are same but mild and
late.
43. Age of onset 12yrs.
By 25yrs.unable to walk.
Death in 5th decade.
BMD Cont,
44. Becker muscular dystrophy
Milder version of
DMD
Etiology
single gene defect
short arm X
chromosome
altered size &
decreased amount of
dystrophin
46. BMD: Epidemiology
Less common
1: 30000 live male birth
Less severe
Family history: atypical MD
47. BMD: Clinical manifestation
Similar & less severe than DMD
Onset: age > 7 years
Pseudohypertrophy of calf
Equinous and varus foot
High rate of scoliosis
Less frequent cardiac involvement
48. BMD: Diagnosis
The same as DMD
Increase CPK
(<200x)
Decrease dystrophin
and/or altered size
49. BMD
Natural history
Slower progression
longer life expectancy
Treatment
the same as in DMD
forefoot equinous:
plantar release,
midfoot dorsal-
wedge osteotomy
50. DIFFERENCES B/W DMD &
BMD
Dystrophin absent
Frameshift mutation
1/3rd new mutations
Onset 2-4yr
Loss of ambulation
10yrs
Death by 20 yr
Cardiomyopathy
common
Dystrophin partially
present
In-frame mutations
New mutations rare
Onset 12 yr
Non ambulant 25-
30yrs
5th decade
Less common
56. Limb-girdle muscular dystrophy
Eitology
Autosomal recessive at chromosome 15q
Autosomal dominant at 5q
Epidemiology
Common
57. Limb-girdle muscular dystrophy
Clinical manifestation
Age of onset: 3rd
decade
Initial: pelvic/shoulder
m. (proximal to distal)
Similar distribution as
DMD
58. LGMD
Classification
Pelvic girdle type
common
Scapulohumeral type
rare
Diagnosis
Same clinical as
DMD/BMD carriers
Moderately elevated
CPK
Normal dystrophin
59. LGMD
Natural history
Slow progression
After onset > 20 y:
contracture &
disability
Rarely significant
scoliosis
Treatment
Similar to DMD
Scoliosis: mild, no
Rx.
60. Fascioscapulohumeral muscular dystrophy
Etilogy
Autosomal dominant
Gene defect (FRG1)
Chromosome 4q35
Epidemiology
Female > male
Clinical
manifestation
Age of onset: late
childhood/ early
adult
No cardiac, CNS
involvement
71. Infantile fascioscapulohumeral
muscular dystrophy
Etiology
Autosomal recessive
Unidentified gene
Clinical manifestation
Facial diplegia
hearing loss
facial weakness
Walk with hands and
forearms folded across
upper buttocks
**Marked & progressive
lumbar lordosis
Less common equinous,
scoliosis
72. IFSMD
Natural history
Infancy: facial
diplegia
Childhood: hearing
loss
2nd decade of life:
wheelchair bound,
severely
compromised
pulmonary function
Treatment
Flexible
equinous/equinovarus foot:
AFO
Hip flextion contracture: no
Rx in ambulate pt.
Spinal deformity in
wheelchai ambulator:
orthosis+ post spinal fusion
with instrumentation
Scapulothoracic
stabilization: not necessary
73. Ocular muscular dystrophy
Rare
Age of onset: adolescence
Extraocular muscle weakness
diplopia limit ocular movement
May involve proximal upper extremities
Slowly progressive
76. Summary
Clinical DMD LGMD FSMD DD CMD
Incidence common less Not
common
Rare Rare
Age of onset 3-6 y 2nd decade 2nd decade 20-77 y At/ after
birth
Sex Male Either sex M = F Either sex Both
Inheritance Sex-linked
recessive
AR, rare AD AD AD Unknown
Muscle
involve.
Proximal to
distal
Proximal to
distal
Face &
shoulder to
pelvic
Distal Generalized
Muscle
spread until
late
Leg, hand,
arm, face,
larynx,eye
Upper ex,
calf
Back ext,
hip abd,
quad
Proximal -
77. Summary
Clinical DMD LGMD FSMD DD CMD
Pseudo
hypertrophy
80%
calf
< 33% Rare no No
Contracture Common Late Mild, late Mild, late Severe
Scoliosis
Kyphoscoliosis
Common,
late
Late - - ?
Heart Hypertrophy
tachycardia
Very rare Very rare Very rare Not
observed
Intellectual decrease Normal Normal Normal ?
Course Stead, rapid Slow Insidious benign Steady