More Related Content

PDF

PDF
Voice Therapy: Management Of Benign Voice Disorders 
PPT
Vocal cord paralysis current concepts 
PDF
Tens en mujer con disfonia 
PPTX

PPTX
TRADITIONAL APPROACHES.pptx 
PPTX
puberphonia voice disorder management and assessment 
PPTX
VOICE REHABilitation after surgery final.pptx Similar to Multimodal_Voice_Therapy.pptx ahfrjjhrtk

PDF
Bilateral TVC paralysis Dr. M. Erami 
PDF
UNILATERAL VOCAL FOLD PARALYSIS - powerpoint presentation 
PPT
![784cdysphonia[1]](https://cdn.slidesharecdn.com/ss_thumbnails/784cdysphonia1-1234158878157310-2-thumbnail.jpg?width=640&height=640&fit=bounds)
PPT

PPTX
Disorders of voice for undergraduates including Hoarseness 
PPT
Rehabilitation after treatment of cancer larynx sujay susikar 
PPTX
APPROACH TO A PATIENT WITH VOCAL CORD PARALYSIS 
PPTX

PPTX
Voice therapy to treat voice disorders 
PPTX
STRUCTURAL DISORDERS of the vocal cords.pptx 
PPTX

DOC

PPT
F081 Coclia 75 Phonosurgery 
PPTX
DISORDERS OF VOICE final .pptx 
PPT
Rehabilitation after laryngectomy 
PPTX
Vocal fold paralysis/ Paresis full 
PPTX

PPTX
Vocal cord paralysis and evaluation of hoarseness 
PPTX
16. vocal cord paralysis and evaluation of hoarseness kk 
PPTX
Neurological conditions of larynx ashly Recently uploaded

PPTX
LOW DOSE RADIATHERAPY (LDRT) IN OSTEOARTHRITIS 
PPTX
THE STUDY OF MIND content intro and basics.pptx 
PPTX
Anatomy of temporal & infratemporal fossa.pptx 
PPTX
1.-Dr.-Ajay-Khera- Anemia Mukt Bharat.pptx 
PDF
COLLOIDAL DISPERSION PPTx. S.Y B-PHARM . 
DOCX
Pharmacotherapeutics - II Practical Record with Clinical Examination (20 cases) 
PPTX
Atrial Fibrillation and difference with Atrial flutter 
PPTX
Infectious diseases of the head and neck 2.pptx ![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
PPTX
PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx 
PDF
Medicinal &Toilet Preparation Act T.Y.B-PHARM 
PDF
Best Sexologist Unit in Araria, Bihar @dubeyclinicpatna 
PDF
Police Officer Mental Health & Wellness Programs | MyOmnia 
PPTX
Venous cutdown for Surgery Viva, MBBS Students 
PPTX
sinusitis.....................................pptx 
PDF
Vitamin K works in conjunction with D to the Knesset .pdf 
PPT
Managemant of Mutilated Vital Teeth presentation ![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
PPTX
CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k... 
PDF
Code of Ehics PPT, T.Y. B-PHARM ,5TH SEM 
PDF
A beginner-friendly introduction to gym training 
PDF
Seminario biología molecula - EBV-miR-BART5-3p Multimodal_Voice_Therapy.pptx ahfrjjhrtk
- 1.
- 2.
Background
• • Benignvocal fold lesions (nodules, polyps,
cysts) cause dysphonia and fatigue.
• • Standard care: voice therapy, vocal hygiene,
surgery if needed.
• • Physiotherapy-based modalities remain
underexplored in voice rehabilitation.
• • Novel approach: Ultrasound + TENS +
Incentive Spirometry.
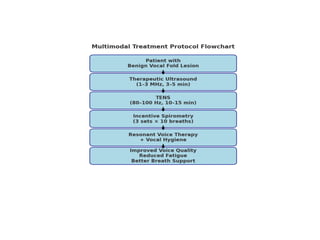
- 3.
Intervention Protocol
• 1.Therapeutic Ultrasound
• - 1–3 MHz, pulsed mode, 3–5 min
• 2. TENS (Neuromuscular Stimulation)
• - 80–100 Hz, 10–15 min, peri-laryngeal
placement
• 3. Incentive Spirometry
• - 3 sets × 10 breaths, diaphragmatic
- 4.
Outcomes
• • Improvedvocal quality (GRBAS scale).
• • Reduced jitter, shimmer, increased HNR.
• • Decreased patient-reported vocal fatigue.
• • Improved respiratory control and phonation.
• • Enhanced vocal endurance.