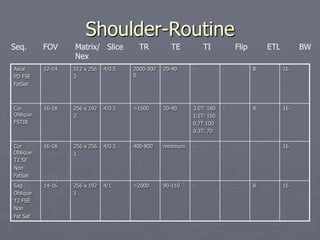
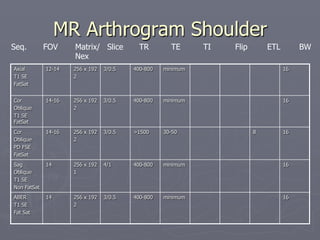
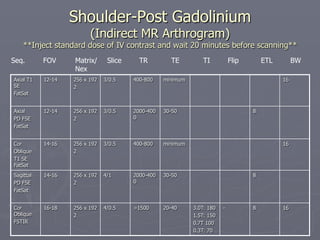
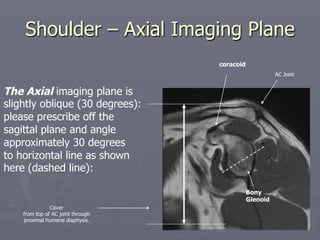
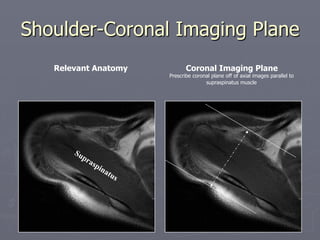
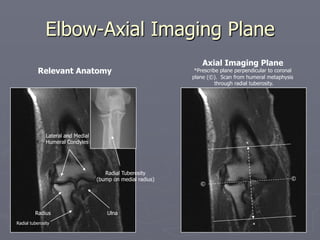
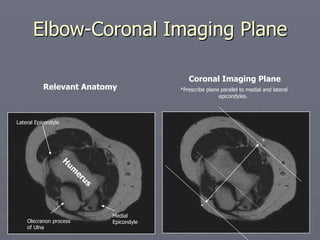
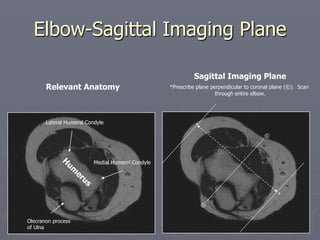
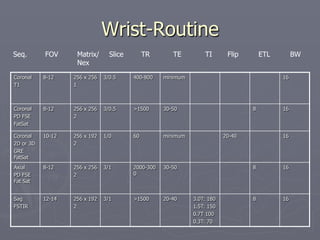
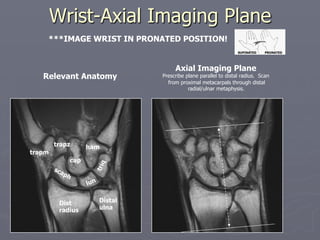
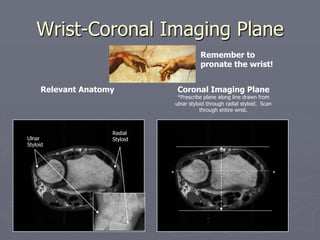
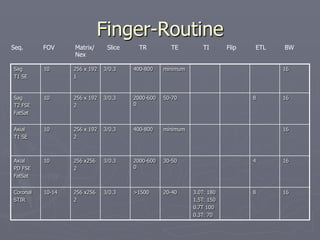
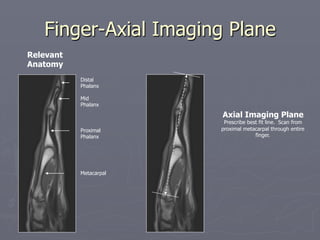
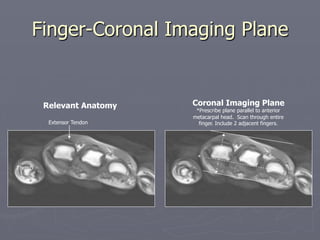
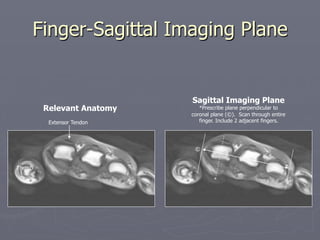
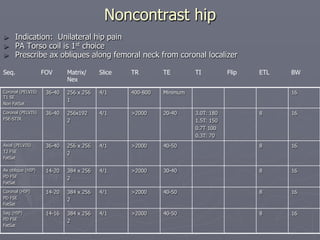
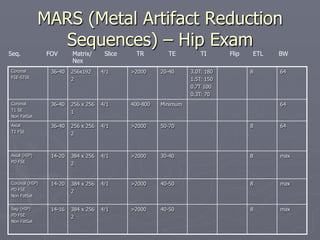
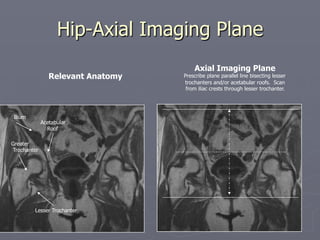
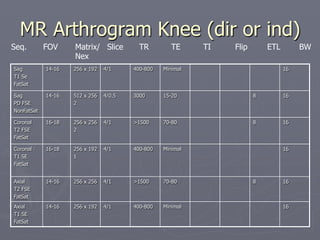
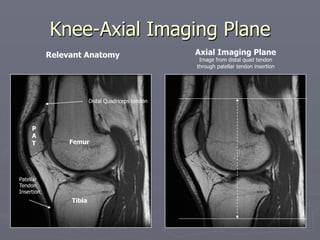
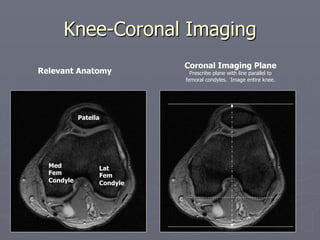
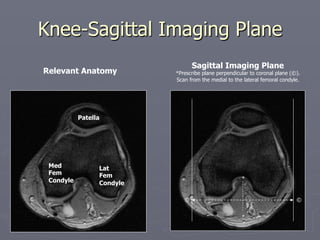
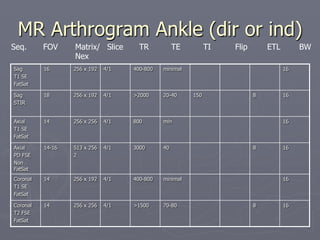
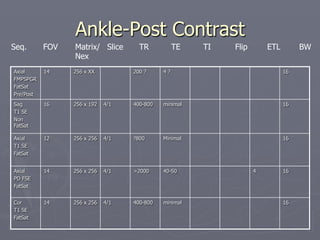
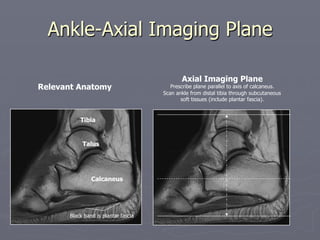
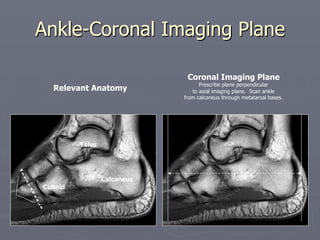
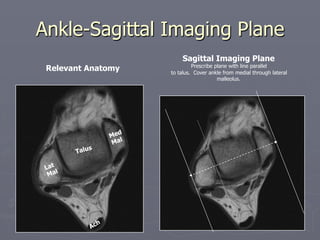
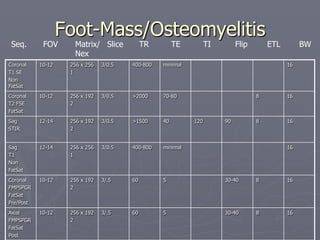
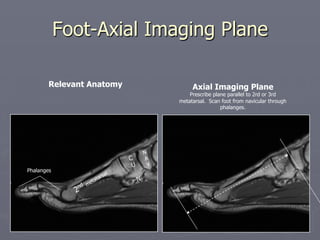
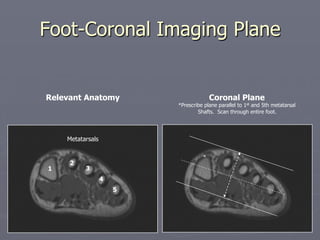
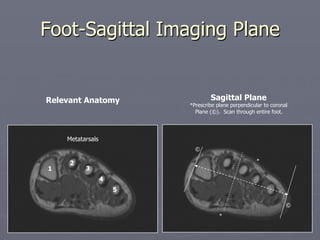
The document provides MRI protocols for various musculoskeletal regions including the chest, shoulder, elbow, wrist, and thumb. For the shoulder, it lists protocols for routine exams, MR arthrograms, and post-gadolinium exams. The elbow section outlines similar routine, arthrogram, and post-gadolinium protocols. For the wrist, it again lists routine, arthrogram, and dynamic post-gadolinium protocols and emphasizes the importance of pre- and post-gadolinium coronal images through the carpal bones. Imaging planes and relevant anatomy are also described for each region.