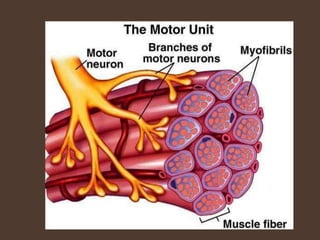
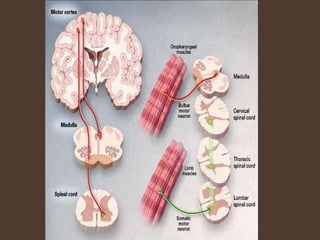
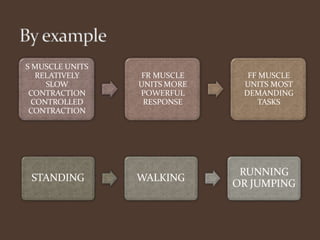
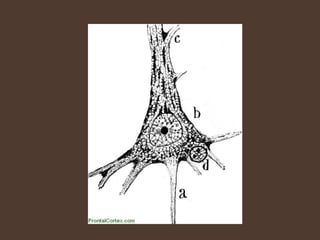
A motor unit consists of a single motor neuron and the muscle fibers it innervates. The number of muscle fibers in a motor unit varies between different muscles, from 3-6 fibers in small muscles like those controlling eye movement, to around 600 fibers in larger leg muscles. Motor units are classified as slow, fast-resistant, or fast-fatigable based on the type and duration of contraction of the muscle fibers they innervate. In amyotrophic lateral sclerosis (ALS), there is a progressive degeneration and death of both upper and lower motor neurons, leading to muscle weakness, atrophy, and eventual paralysis.