The document discusses theories of motor control and motor learning, emphasizing the importance of understanding movement's regulation. Key theories include reflex, hierarchical, and dynamic systems theories, each offering insights into how movements are initiated and controlled. The document also covers different forms of motor learning, including non-declarative and declarative learning, along with their clinical implications for physiotherapy practice.











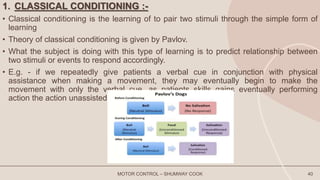













































![Share CONTROL OF BODY MOVEMENT[1]PHYSIO PRESENTATION.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/sharecontrolofbodymovement1physiopresentation-250504162954-915fb5e5-thumbnail.jpg?width=640&height=640&fit=bounds)


























