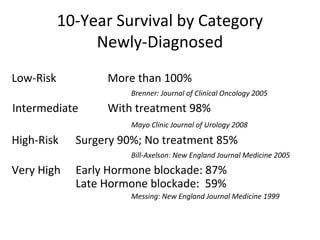
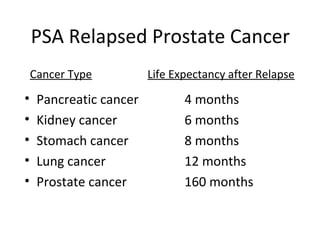
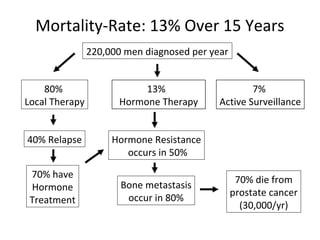
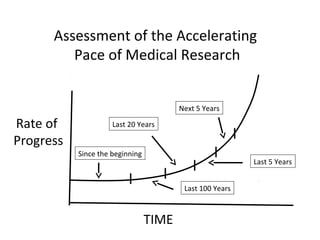
This document discusses the numerous variables involved in prostate cancer treatment decisions. It covers factors like risk level, treatment options for newly diagnosed, recurrent, and advanced prostate cancer. It also addresses how patient characteristics, relationships, personality, and understanding of statistics can influence decisions. Additionally, it outlines the many uncertainties in prostate cancer like rapid technology changes, limitations of studies and doctors, and potential profit motives. The conclusion is that prostate cancer requires considering a man's overall health, relationships, and quality of life when determining the often complex management options.