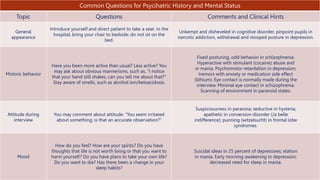
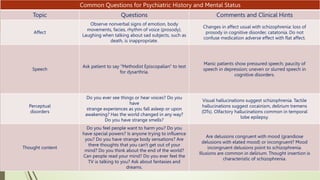
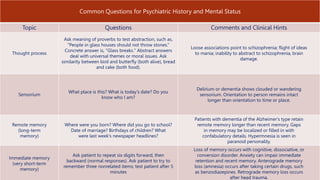
The document provides an overview of how to conduct a mental status examination. It describes the key components to assess including appearance, attitude, speech, mood, affect, thought process, thought content, perceptions, and cognition. For each component, it lists what should be evaluated and provides examples of descriptive terms. The goal of the mental status exam is to understand the patient's psychological state and how it may be impacting their presentation and symptoms.