Downloaded 289 times

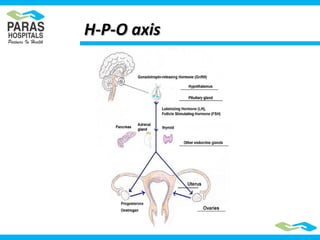
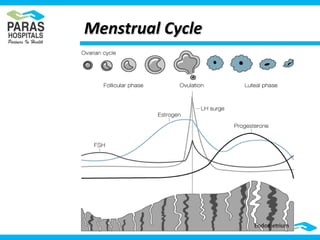
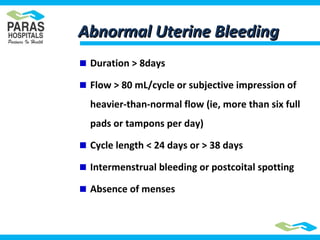
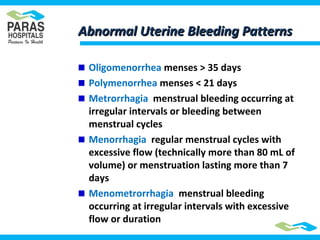
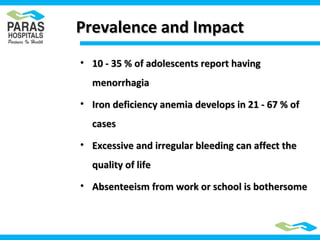
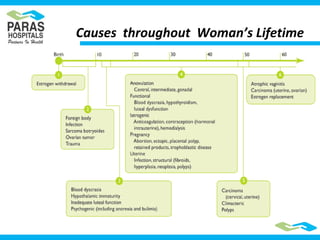
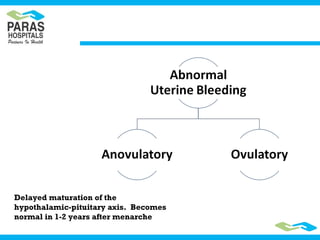
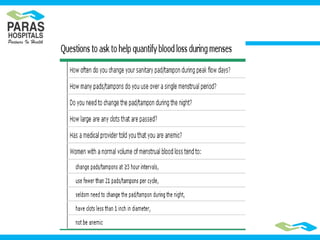


Menstrual disorders are common in adolescents. Normal menstrual cycles typically involve the release of an egg each month under control of the hypothalamic-pituitary-ovarian axis. Abnormal uterine bleeding can include heavy or irregular bleeding. Common causes of menstrual problems include polycystic ovarian syndrome, bleeding disorders, and anovulation. Treatment depends on the underlying cause but may include birth control pills, NSAIDs, or surgery.































































![Vitamin D and Women's Health [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/vitamindwomenhealthautosaved-191231021803-thumbnail.jpg?width=640&height=640&fit=bounds)























