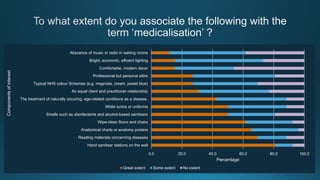
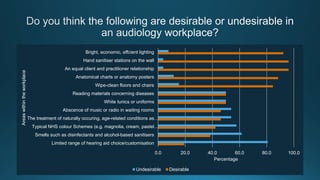
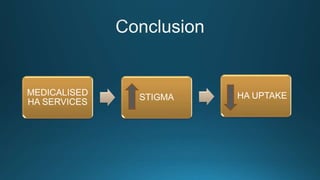
The document discusses audiologists' views on the medicalization of NHS hearing aid services and its impact on stigma and uptake of hearing aids. It reports on a pilot study that surveyed audiologists about desirable and undesirable aspects of medicalization. Results showed that while some medicalized elements like disease information and anatomical charts were considered desirable, other aspects like limited hearing aid choice and typical NHS color schemes were viewed as undesirable. The relationship between medicalization, stigma, and hearing aid use is complex. Further research is needed to better understand how to modify medicalized aspects of services to reduce stigma and improve uptake of hearing aids.








![Brooke R; Killan EC; Morrall P. NHS hearing-aid services: some ideas to modify medicalisation and decrease stigma. Audacity. 2014; (4):50-52.
Brooke, R.E. et al. 2015. Moderate-medicalisation and an age-neutral NHS hearing aid service. British Journal of Healthcare Management. 21(3), pp.117-122.
Chisolm, T.H. et al. 2007. A systematic review of health-related quality of life and hearing aids: final report of the American Academy of Audiology Task Force On the Health-Related Quality of Life Benefits
of Amplification in Adults. J Am Acad Audiol. 18(2), pp.151-83.
Conrad, P. 2007. The medicalization of society : on the transformation of human conditions into treatable disorders. Baltimore: Johns Hopkins University Press.
Crocker, J. 1999. Social stigma and self-esteem: Situational construction of self-worth. Journal of Experimental Social Psychology. 35(1), pp.89-107.
Davis, A. et al. 2007. Acceptability, benefit and costs of early screening for hearing disability: a study of potential screening tests and models. Health Technol Assess. 11(42), pp.1-294..
Dawes, P. et al. 2014. Hearing in middle age: a population snapshot of 40- to 69-year olds in the United Kingdom. Ear Hear. 35(3), pp.e44-51.
Erler, S.F. and Garstecki, D.C. 2002. Hearing loss- and hearing aid-related stigma: perceptions of women with age-normal hearing. Am J Audiol. 11(2), pp.83-91.
Garstecki, D.C. and Erler, S.F. 1998. Hearing loss, control, and demographic factors influencing hearing aid use among older adults. J Speech Lang Hear Res. 41(3), pp.527-37.
Hetu, R. 1996. The stigma attached to hearing impairment. Scand Audiol Suppl. 43, pp.12-24.
Hosford-Dunn, H. and Halpern, J. 2001. Clinical application of the SADL scale in private practice II: predictive validity of fitting variables. Satisfaction with Amplification in Daily Life. J Am Acad Audiol. 12(1),
pp.15-36.
International Longevity Centre UK. 2014. Commission on Hearing Loss: Final report. [Online]. [Accessed 15 March 2015] Available from: http://www.ilcuk.org.uk/.
Knudsen, L.V. et al. 2010. Factors influencing help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: a review of the literature. Trends Amplif. 14(3), pp.127-54..
Lin, F.R. et al. 2013. Hearing loss and cognitive decline in older adults. JAMA Intern Med. 173(4), pp.293-9.
McCormack, A. and Fortnum, H. 2013. Why do people fitted with hearing aids not wear them? International Journal of Audiology. 52(5), pp.360-368.
Meister, H. et al. 2008. The relationship between pre-fitting expectations and willingness to use hearing aids. Int J Audiol. 47(4), pp.153-9.
Morgan-Jones, R.A. 2001. Hearing differently : the impact of hearing impairment on family life. London: Whurr.
Morrall, P. 2009. Sociology and health : an introduction. 2nd ed. Abingdon, Oxon ; New York: Routledge.
Wallhagen, M.I. 2010. The stigma of hearing loss. Gerontologist. 50(1), pp.66-75.
Young, M.E. et al. 2008. The role of medical language in changing public perceptions of illness. PLoS One. 3(12), pe3875.](https://image.slidesharecdn.com/efafdd1d-75b4-4afd-a74a-59efe5ac4d9b-160619201810/85/Medicalisation-presentation-19-320.jpg)


































































