Matrix metalloproteinases (MMPs) are a family of zinc-dependent endopeptidases that degrade extracellular matrix components. MMPs play important roles in tissue remodeling during processes like wound healing and organ development by breaking down collagen, elastin, fibronectin and other matrix proteins. Their activity is regulated by tissue inhibitors of metalloproteinases (TIMPs). Abnormal MMP activity is associated with diseases like cancer, atherosclerosis, and rheumatoid arthritis by facilitating tissue invasion or destruction.
![MOLECULAR CONTROL
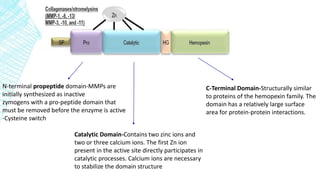
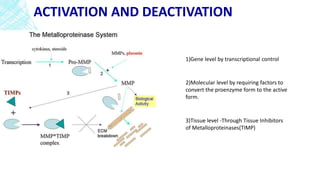
▪ MMPs are synthesized as inactive zymogens and require activation.
▪ The cysteine in the propeptide interacts with a Zn2+ ion in the enzyme’s active site.
▪ This interaction, [Zn2+-cysteine], keeps the proMMP inactive
▪ Activation can occur by physical or chemical means by disturbing the cysteine –zinc
interaction of the cysteine switch .](https://image.slidesharecdn.com/matrixmetalloproteinasesinhealthanddisease-170311082125/85/Matrix-metalloproteinases-18-320.jpg)



































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

