The document provides a comprehensive overview of maternal health, midwifery, and relevant legislation in India, outlining the historical evolution of midwifery and the development of maternal health care practices. It details definitions of maternal morbidity and mortality, maternity benefits, and the Medical Termination of Pregnancy (MTP) Act aimed at enhancing maternal health outcomes. Additionally, it presents current practices, interventions, and incentives related to family planning and maternal well-being in the context of health service delivery.


![• ELIGIBILITY FOR MATERNITY BENEFIT:
• A women shall be entitled to maternity benefit only
if she has actually worked in an establishment of the
employer for a period of not less then eighty days in
the twelve months immediately proceeding the date
of her expected delivery (section-5[2])](https://image.slidesharecdn.com/1stunit-210418085921/85/maternal-health-nursing-introduction-unit-20-320.jpg)
![• MAXIMUM PERIOD OF MATERNITY BENEFIT:
• Maximum twelve weeks of which not more then six weeks shall proceed
the date of her expected delivery (section- 5[5])
• • OTHER BENEFITS: Act also provides provisions for leave for miscarriage,
leave for illness arising out of pregnancy or delivery, premature birth of
child or miscarriage and nursing breaks for nursing the child until the child
attained the age of 15 months
• • DISMISSAL, DEDUCTION WAGES, ETC: No employer shall discharge or
dismiss a women for her absence form work in accordance with the
provisions of this Act and no deduction shall be made from the normal;
and usual daily wages of a women entitled to maternity benefits.](https://image.slidesharecdn.com/1stunit-210418085921/85/maternal-health-nursing-introduction-unit-21-320.jpg)
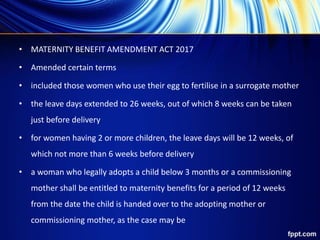
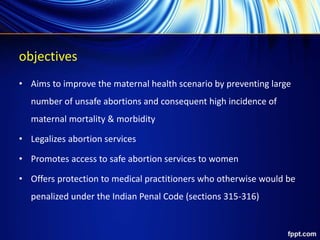
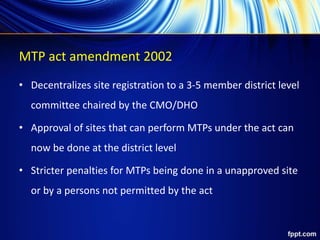

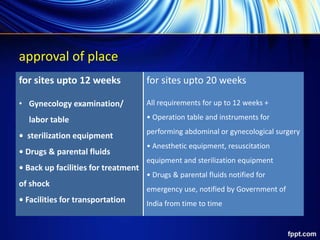
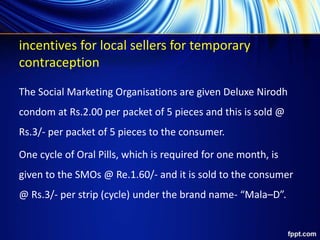
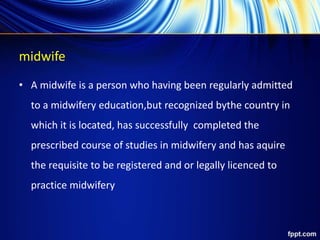
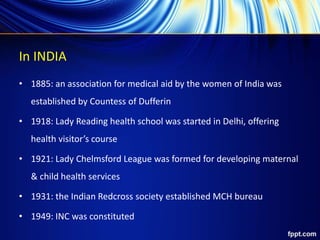
![compensation schemes for permanent method -
public facilities
states type of operation acceptor ASHA/ health
worker
others total
11 High Focus States
(UP, BH, MP,
RJ, CG, JH, OD, UK, AS,
HR, GJ)
vasectomy 2000 300 400 2700
tubectomy 1400 200 400 2000
Other High Focus
States (NE States,
J&K, HP)
vasectomy 1100 200 200 1500
tubectomy 600 150 250 1000
Non High Focus States vasectomy 1100 200 200 1500
tubectomy
[BPL+SC/ST only]
600 150 250 1000
tubectomy [APL] 250 150 250 650](https://image.slidesharecdn.com/1stunit-210418085921/85/maternal-health-nursing-introduction-unit-41-320.jpg)
















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







