- The document discusses a study that examined the effects of a 2-hour cycling exercise protocol on right ventricular structure and function in competitive cyclists.
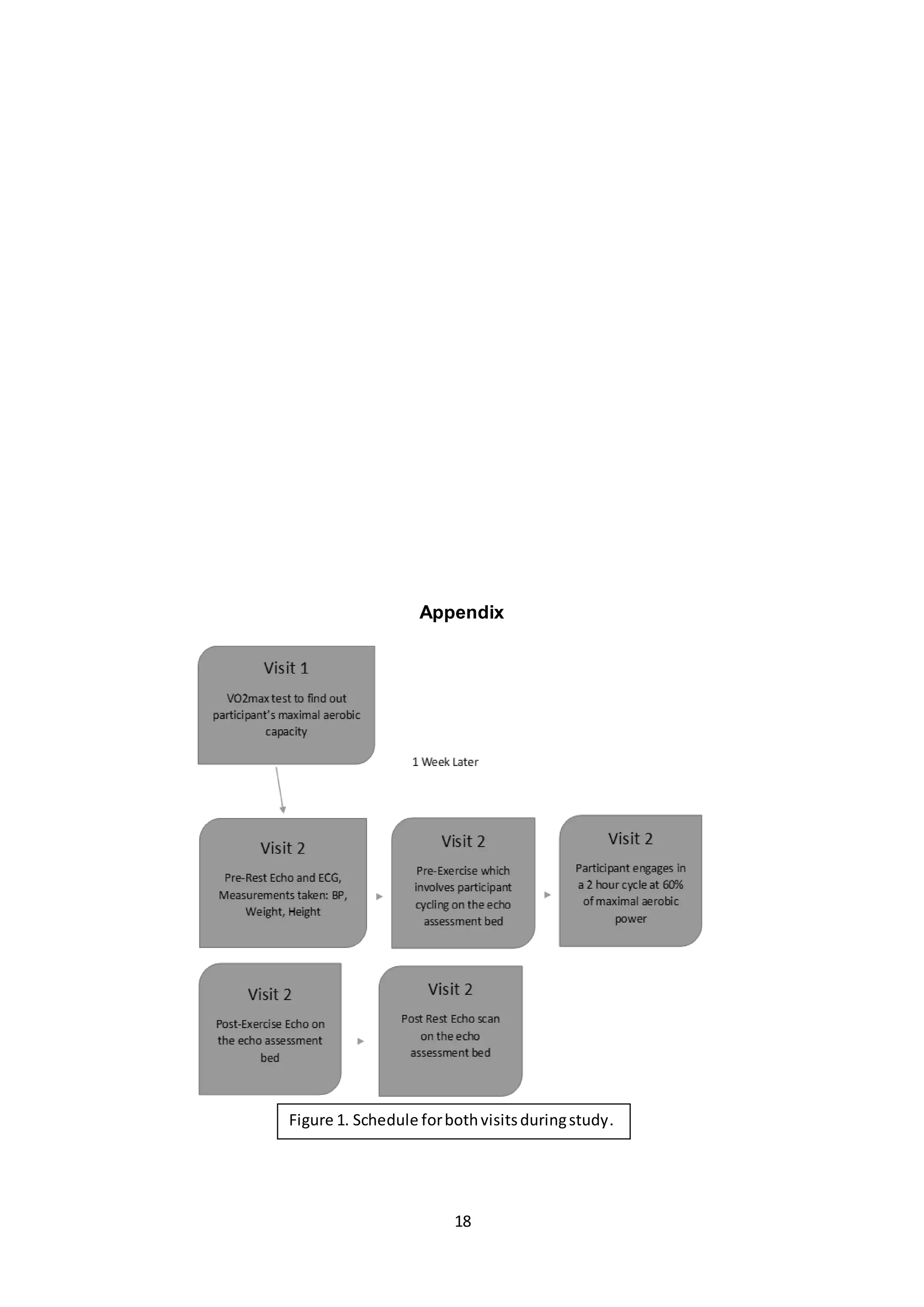
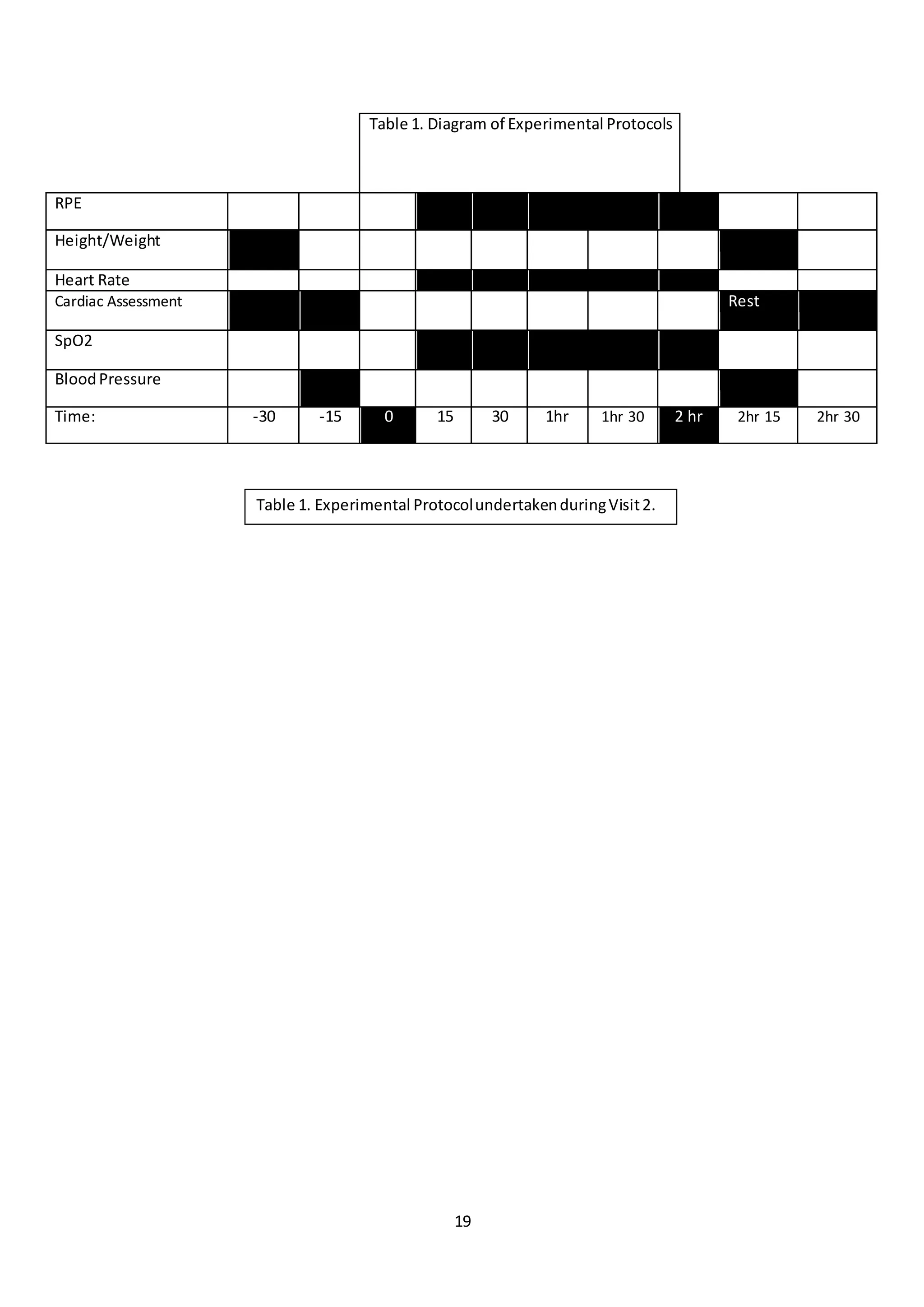
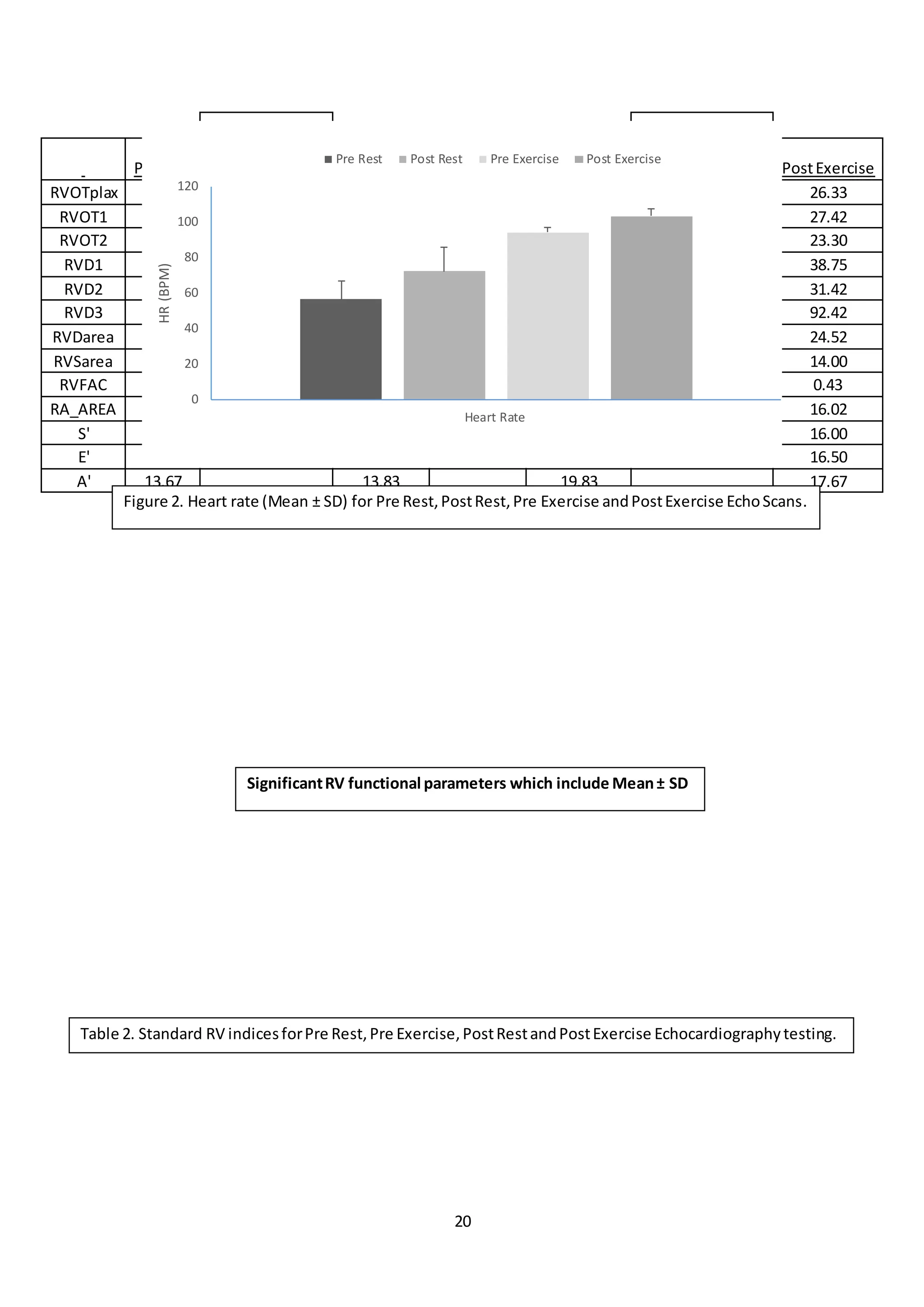
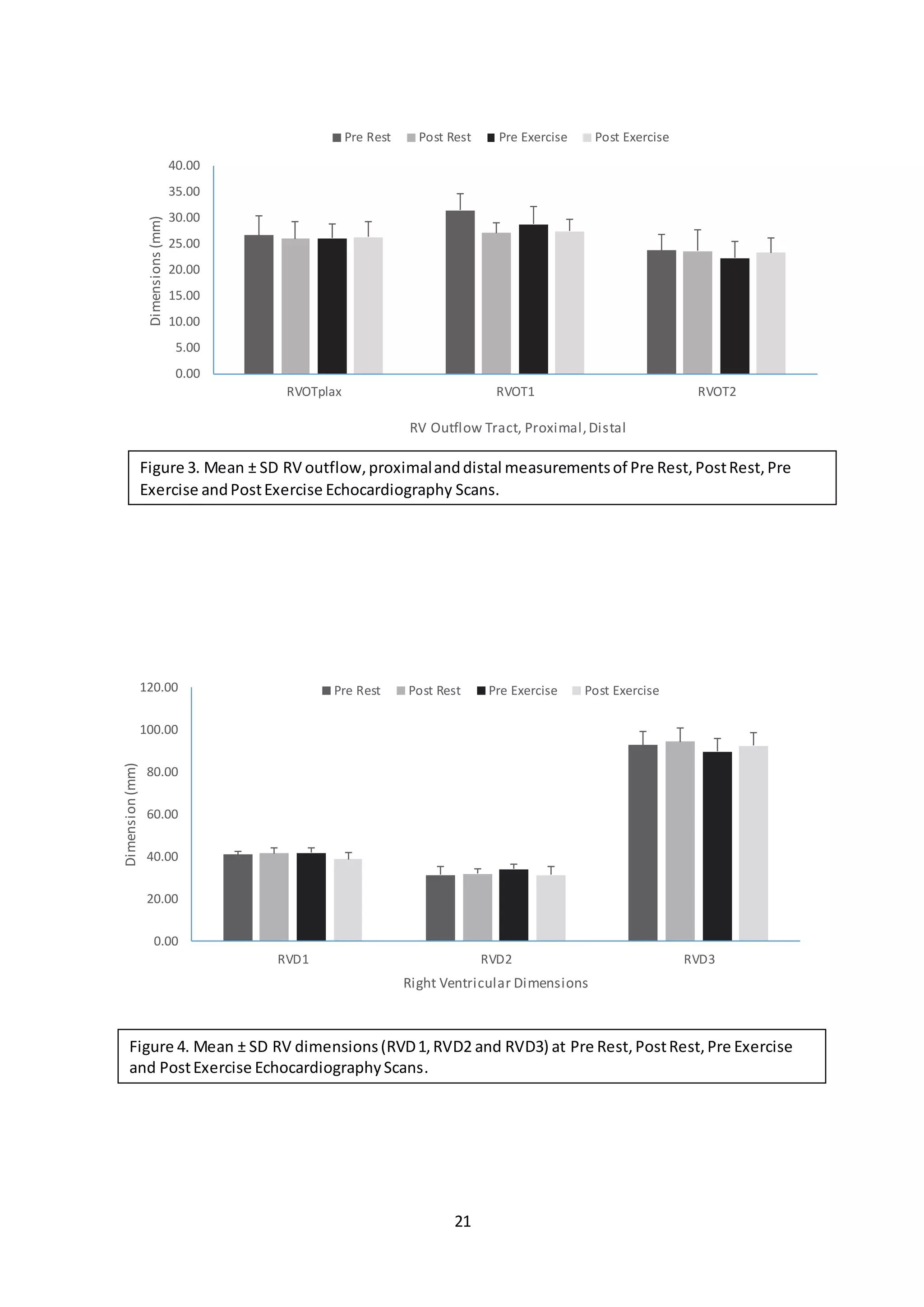
- 6 cyclists underwent cardiac assessments before, during, immediately after, and during recovery from the exercise using echocardiography to measure 13 cardiac parameters.
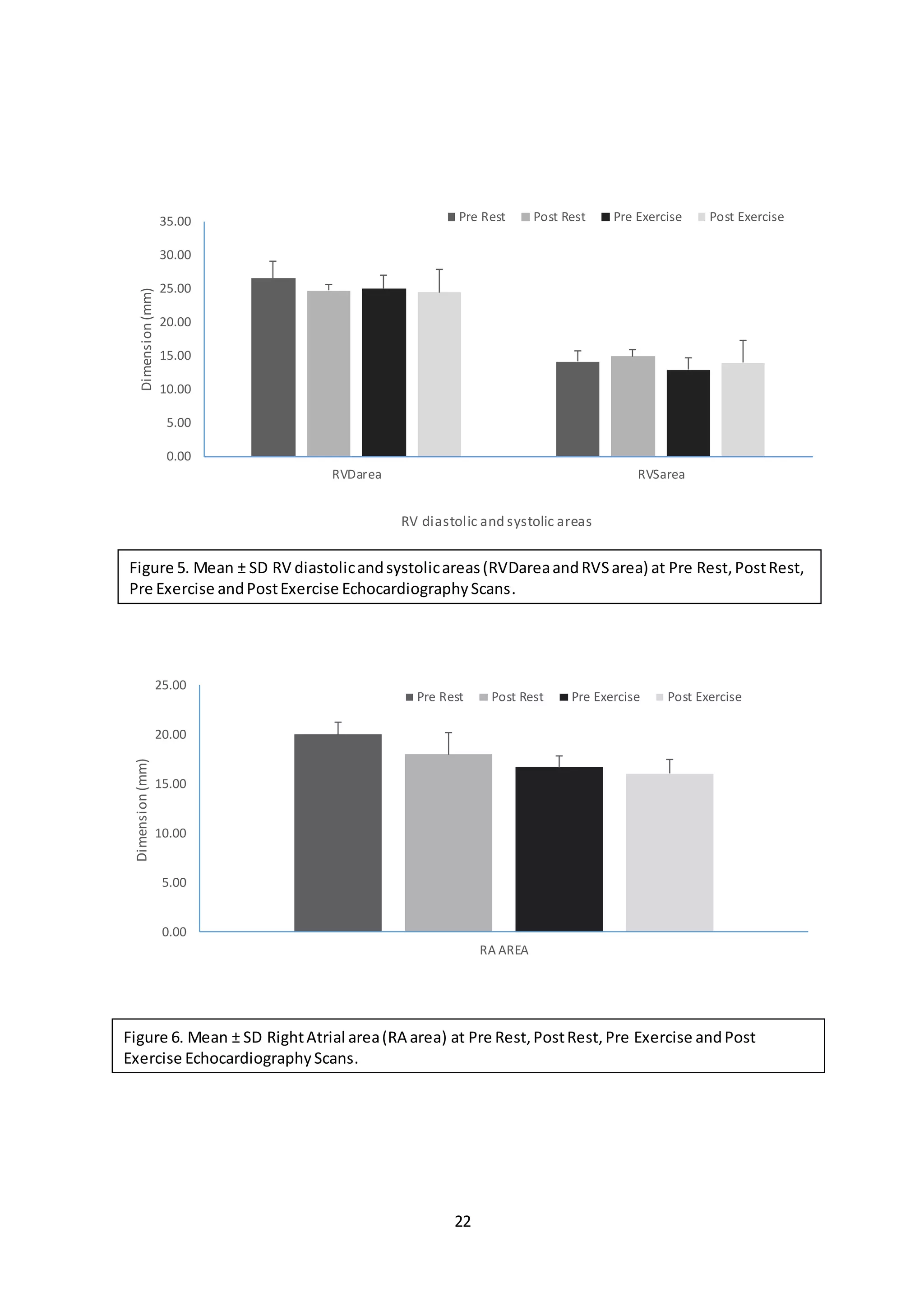
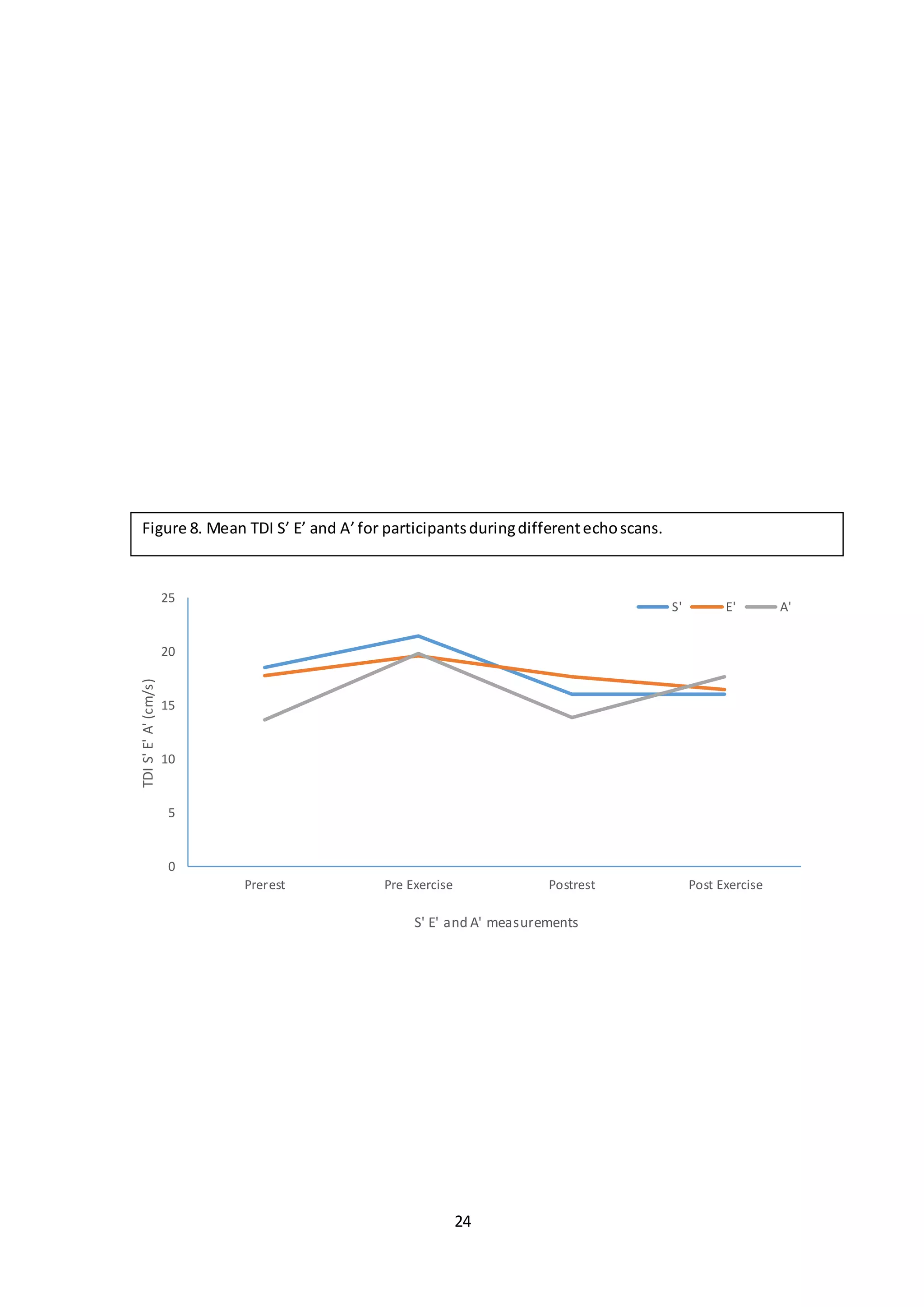
- Significant differences were seen pre- and post-exercise for right ventricular fractional area change, right atrial area, and S', indicating symptoms of exercise-induced cardiac fatigue.