Overview of topics
1.Anatomy and Physiology Of Respiratory
System.
2. Introduction About Mechanical Ventilation
3. History
4. Meaning of Mechanical Ventilation
5. Indications for use
6. Types or Forms Of Mechanical Ventilation
3.
8. Settings
9. Modes.
10.Advantages and disadvantages between
modes.
11. Guidelines in the initiation of mechanical
ventilation.
12. Common trouble shooting examples with
mechanical ventilation
Anatomy and Physiology
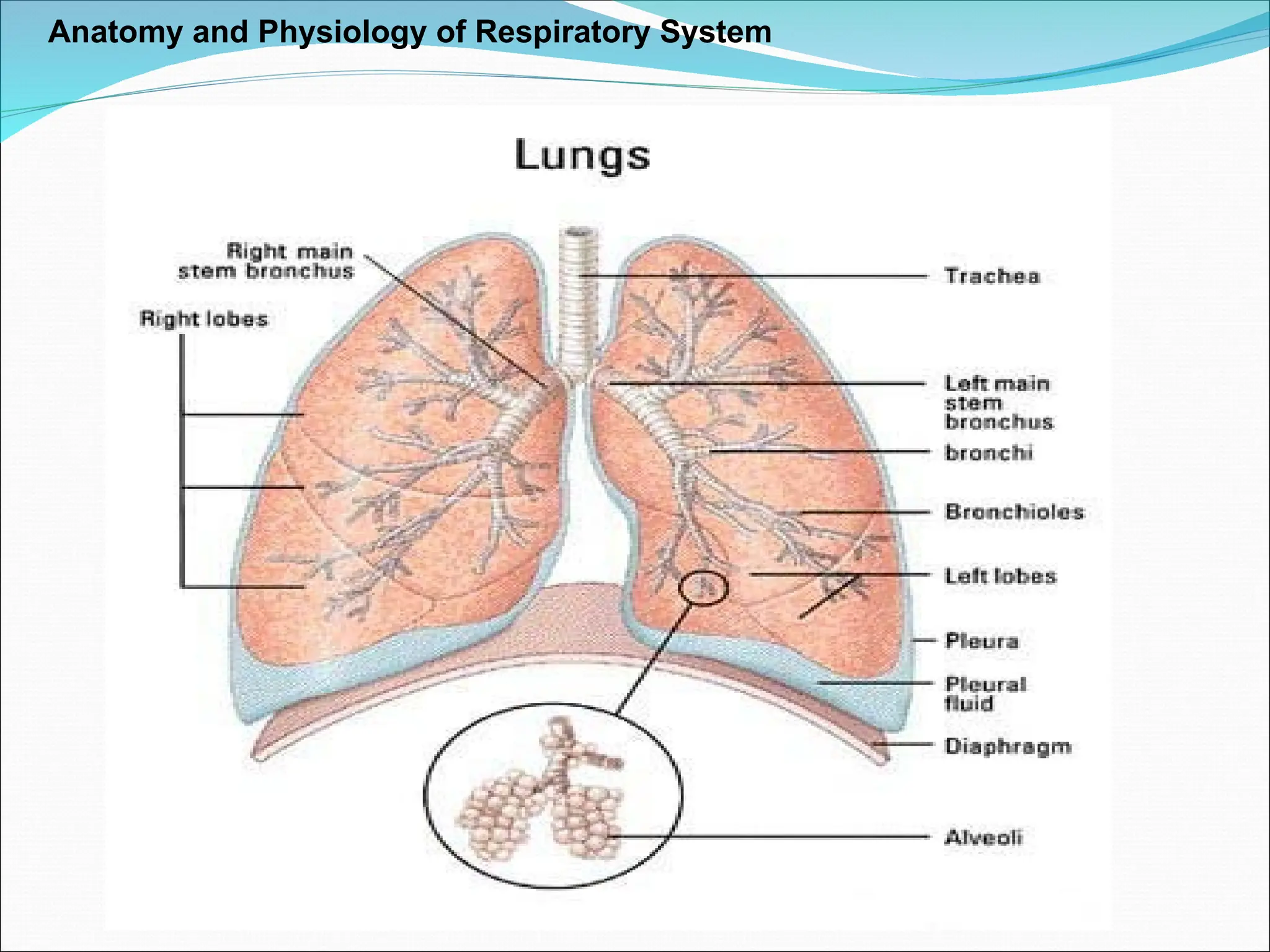
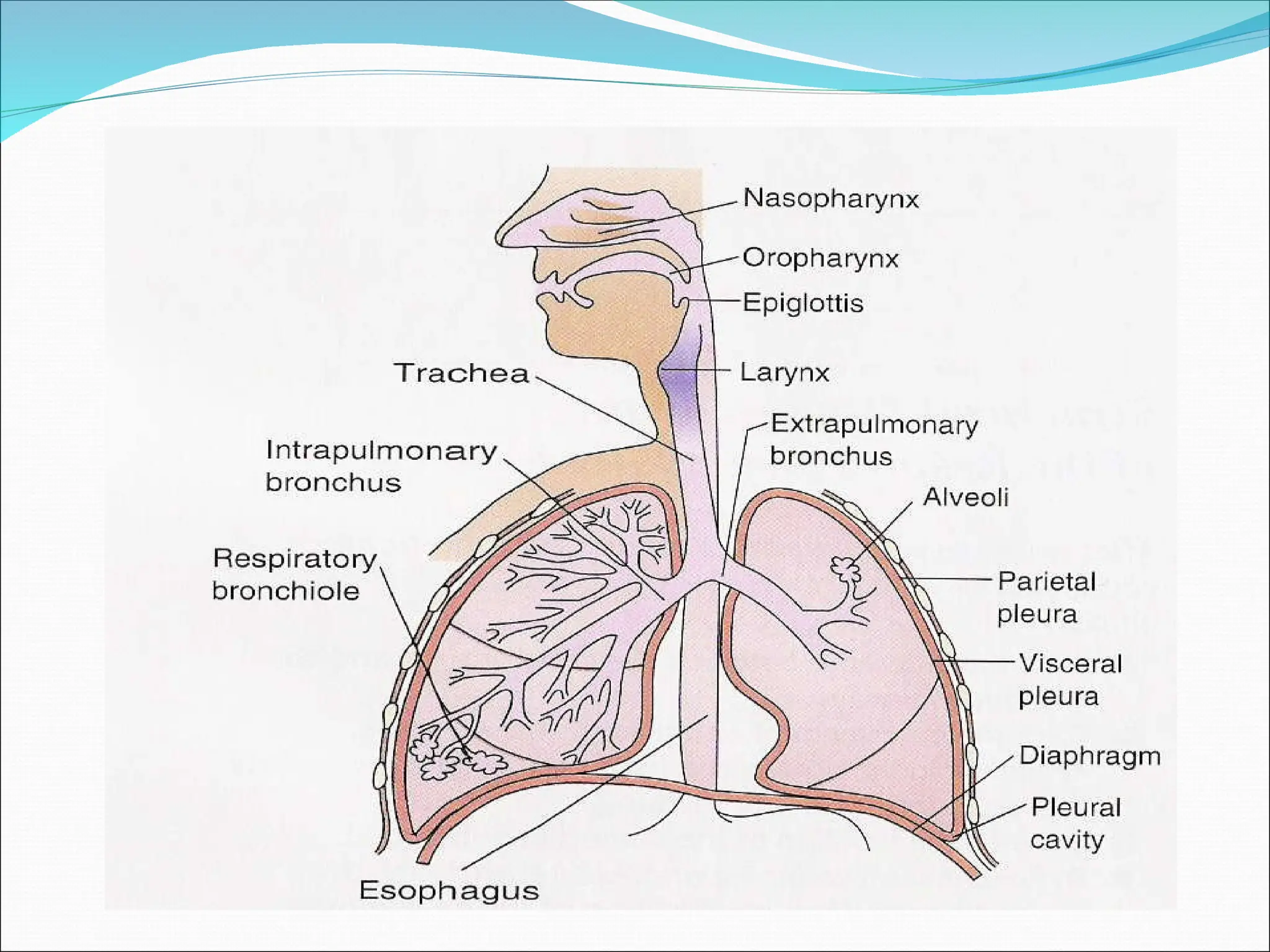
Respiratory Structures
Respiratory Zones
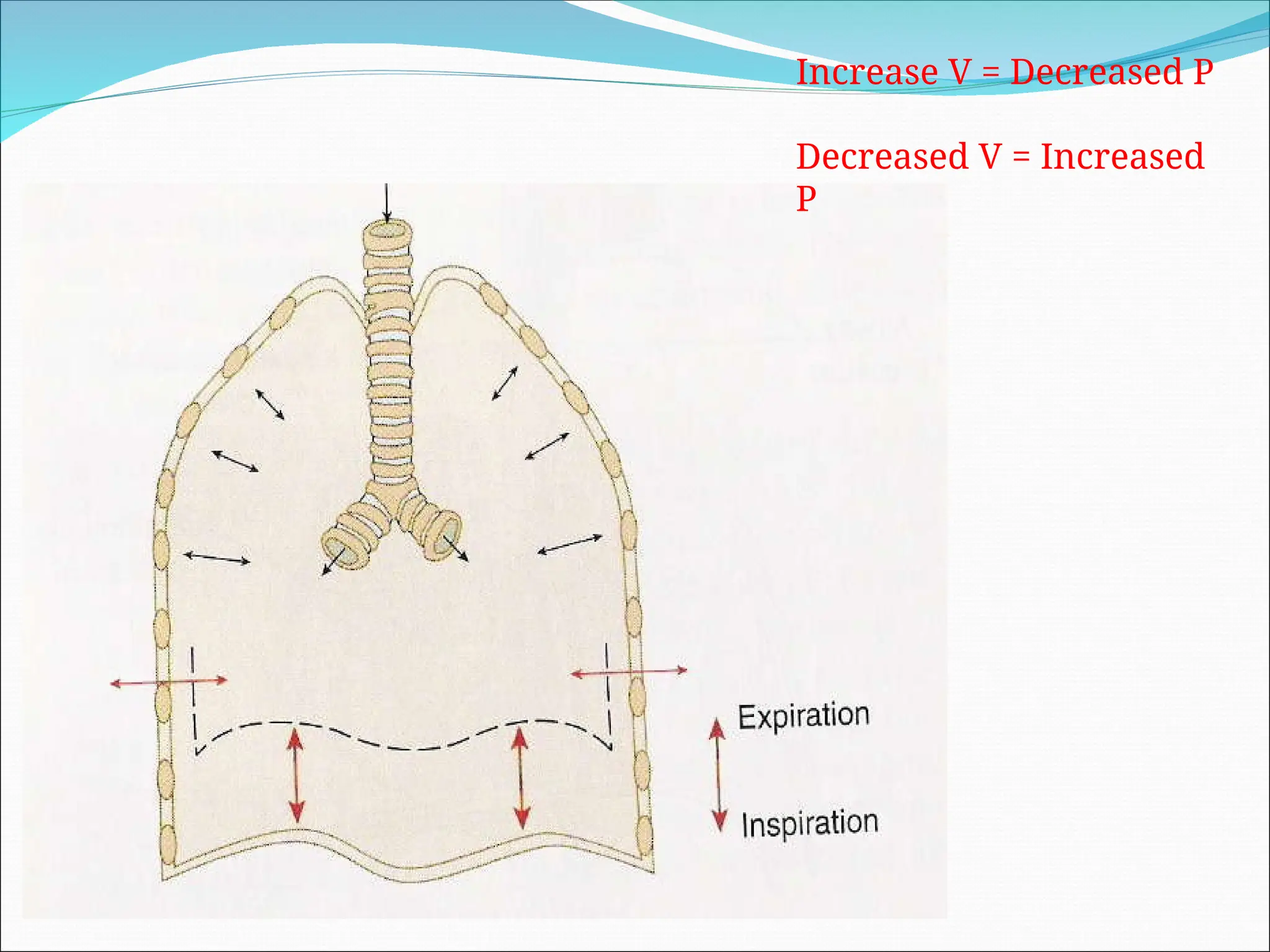
Partitioning of Respiratory Pressures
Boyles Law
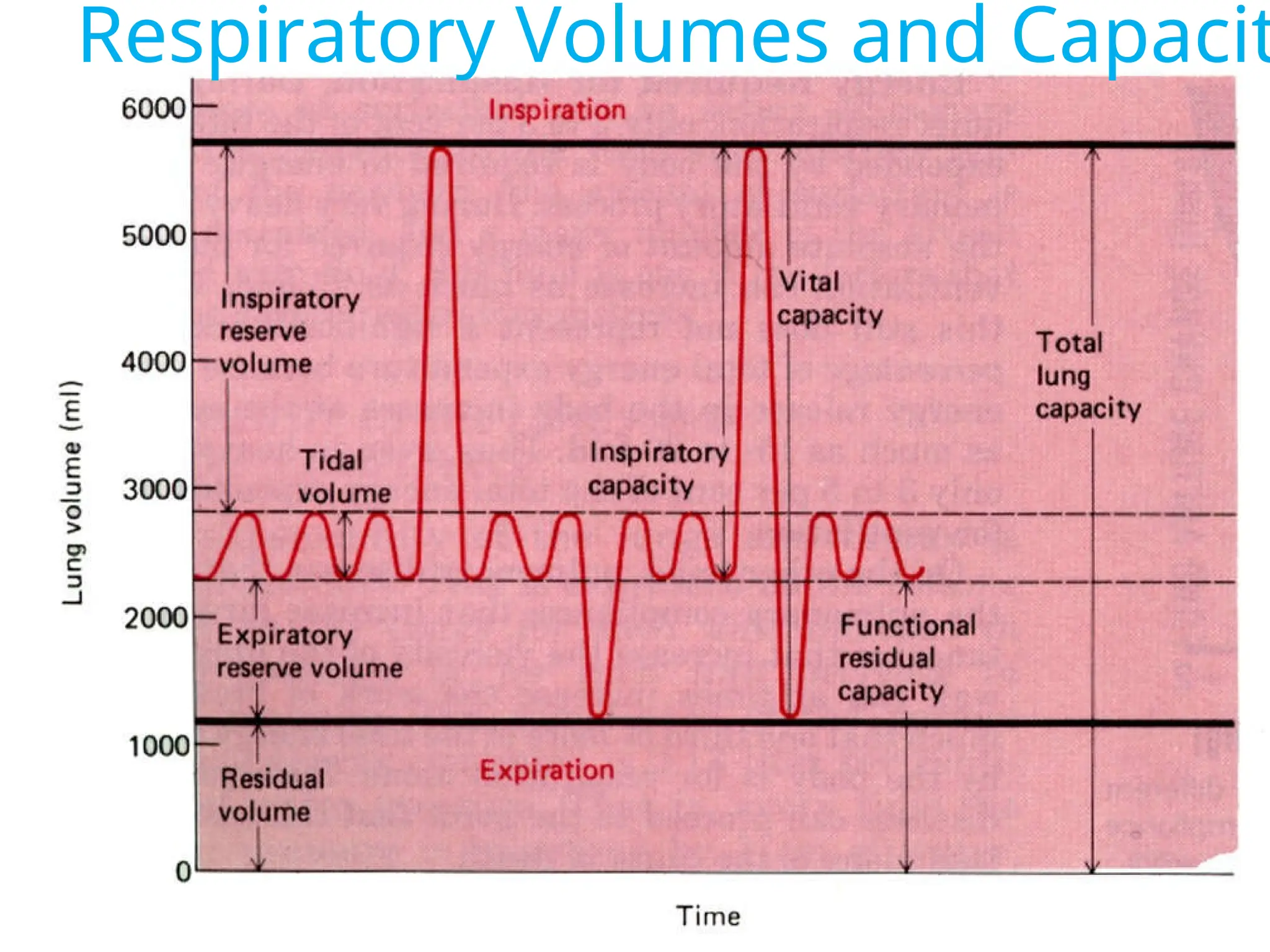
Respiratory Volumes and Capacity
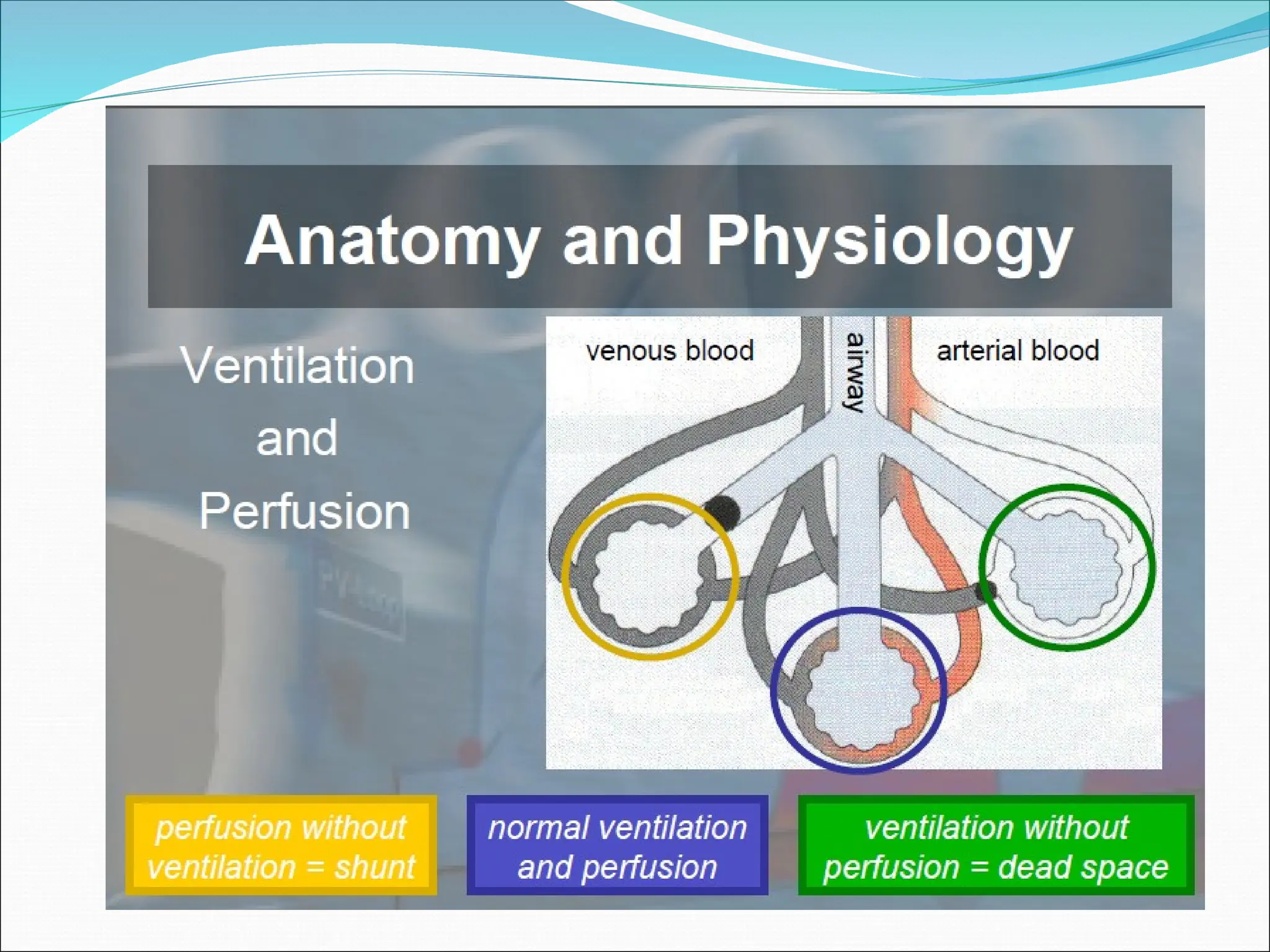
Ventilation and Perfusion
Boyles Law
Airflows from a region of higher pressure to a
region of lower pressure.
To initiate a breath, airflow into the lungs must
be precipitated by a drop in alveolar pressures.
Introduction about Mechanical
Ventilation
Mechanical ventilation is typically used after an
invasive intubation, a procedure wherein an
endotracheal or tracheostomy tube is inserted into
the airway.
It is used in acute settings such as in the ICU for a
short period of time during a serious illness. It may
be used at home or in a nursing or rehabilitation
institution if patients have chronic illnesses that
require long-term ventilation assistance.
14.
Objective of Ventilation
Support though illness
Reversal of hypoxemia
Reversal of acute respiratory acidosis
Relief of respiratory distress
Resting of the ventilatory muscles
Decrease in oxygen consumption
Reduction in intracranial pressures
Stabilisation of the chest wall
15.
History
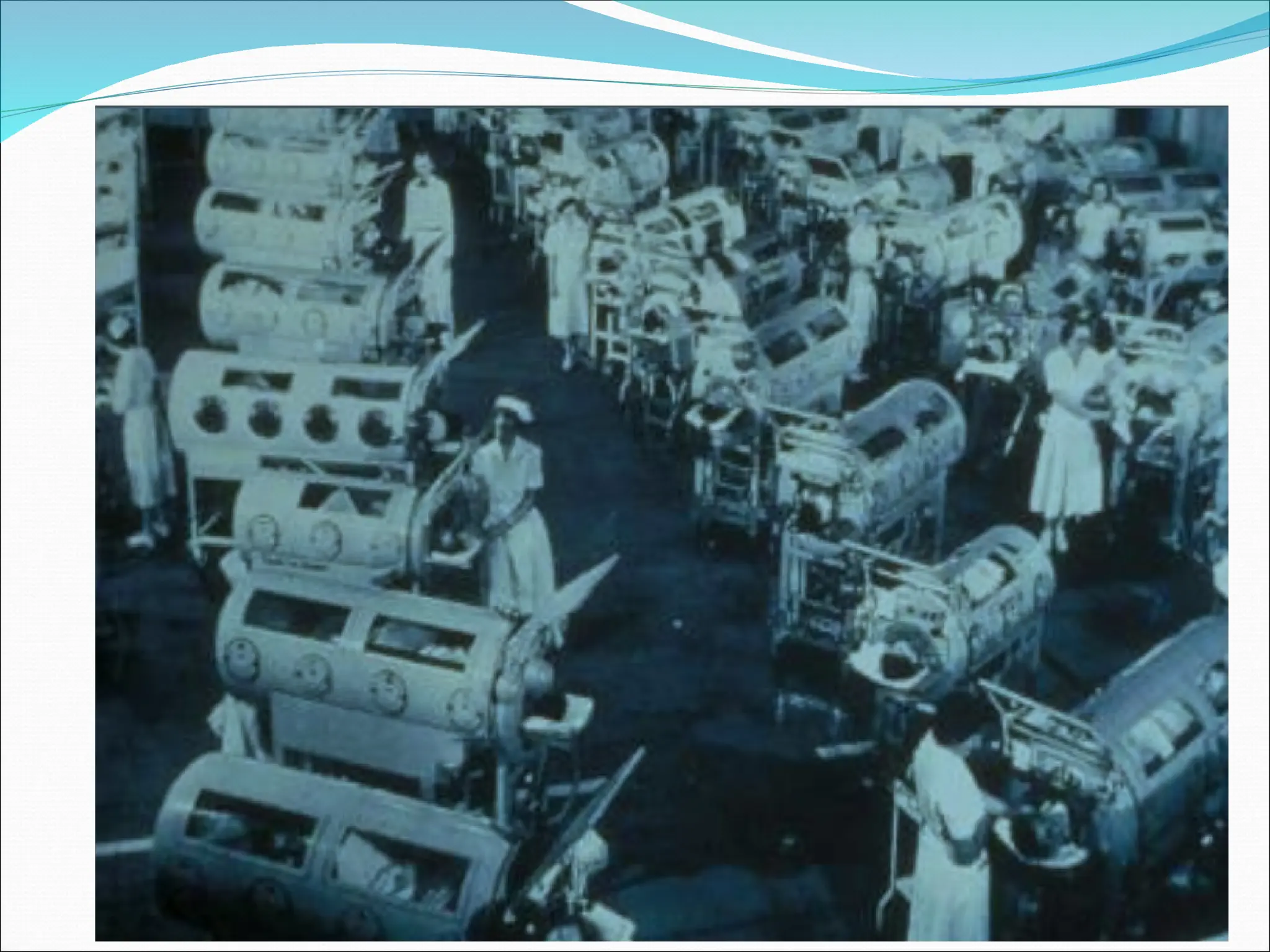
Andreas Vesalius(1555)
Vesalius is credited with the first description of
positive pressure ventilation, but it took 400
years to apply his concept to patient care. The
occasion was the polio epidemic of 1955, when
the demand for assisted ventilation outgrew the
supply of negative-pressure tank ventilators
(known as iron lungs).
16.
History
The romanphysician Galen may have been the
first to describe mechanical ventilation: "If you
take a dead animal and blow air through its
larynx [through a reed], you will fill its bronchi
and watch its lungs attain the greatest
distention.”
Vesalius too describes ventilation by inserting a
reed or cane into the trachea of animals.
In 1908 George Poe demonstrated his mechanical
respirator by asphyxiating dogs and seemingly
bringing them back to life.
17.
In Sweden,all medical schools shut down and
medical students worked in 8-hour shifts as
human ventilators, manually inflating the lungs
of afflicted patients.
Invasive ventilation first used at Massachusetts
General Hospital in 1955.
Thus began the era of positive-pressure
mechanical
ventilation (and the era of intensive care
medicine).
Types or FormsOf Mechanical
Ventilation
The two major types of
Mechanical Ventilation are
Negative pressure and
positive Pressure ventilation
The main form of
mechanical ventilation is
positive pressure
ventilation, which works by
increasing the pressure in
the patient's airway and thus
forcing air into the lungs.
21.
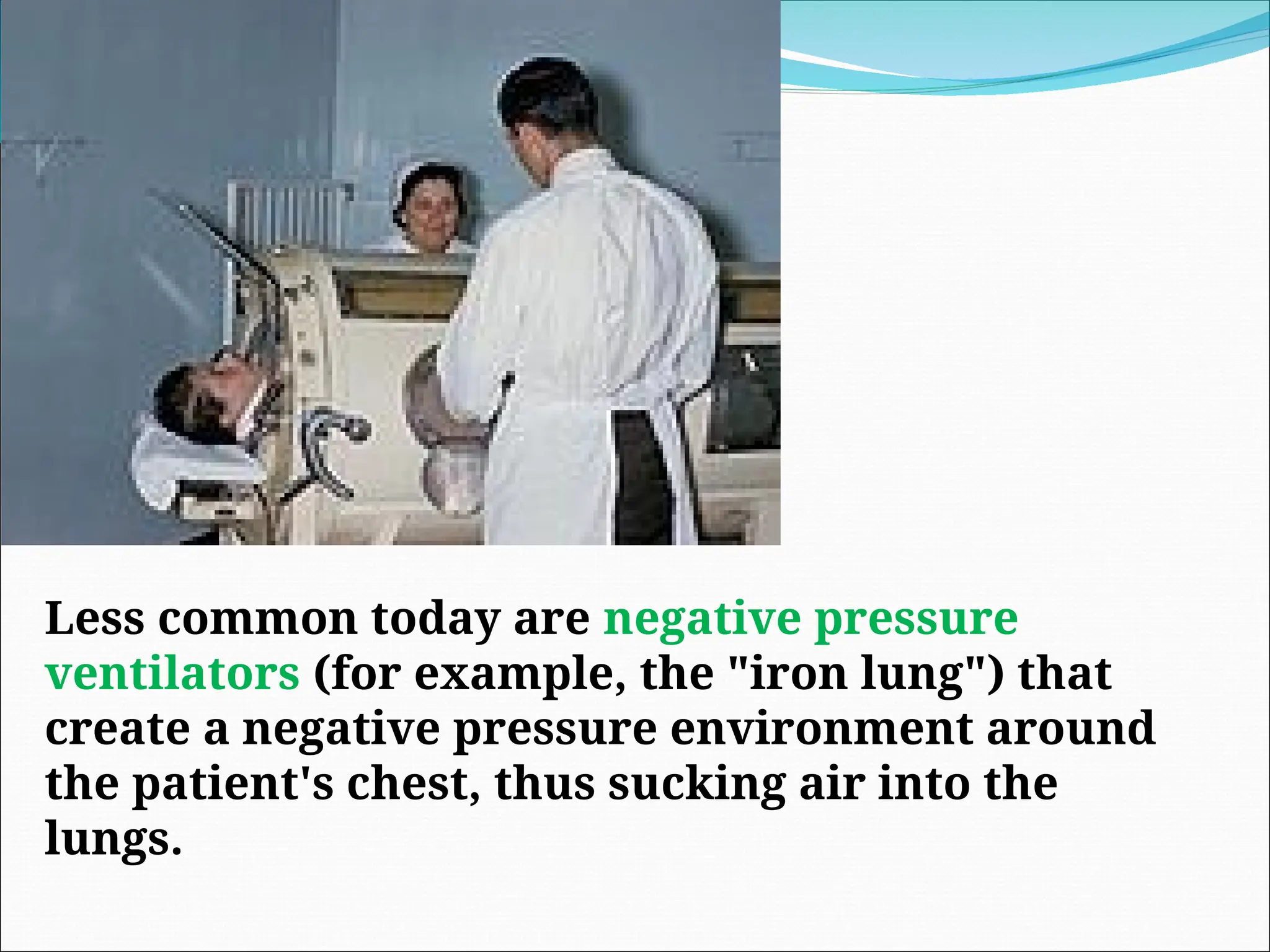
Less common todayare negative pressure
ventilators (for example, the "iron lung") that
create a negative pressure environment around
the patient's chest, thus sucking air into the
lungs.
22.
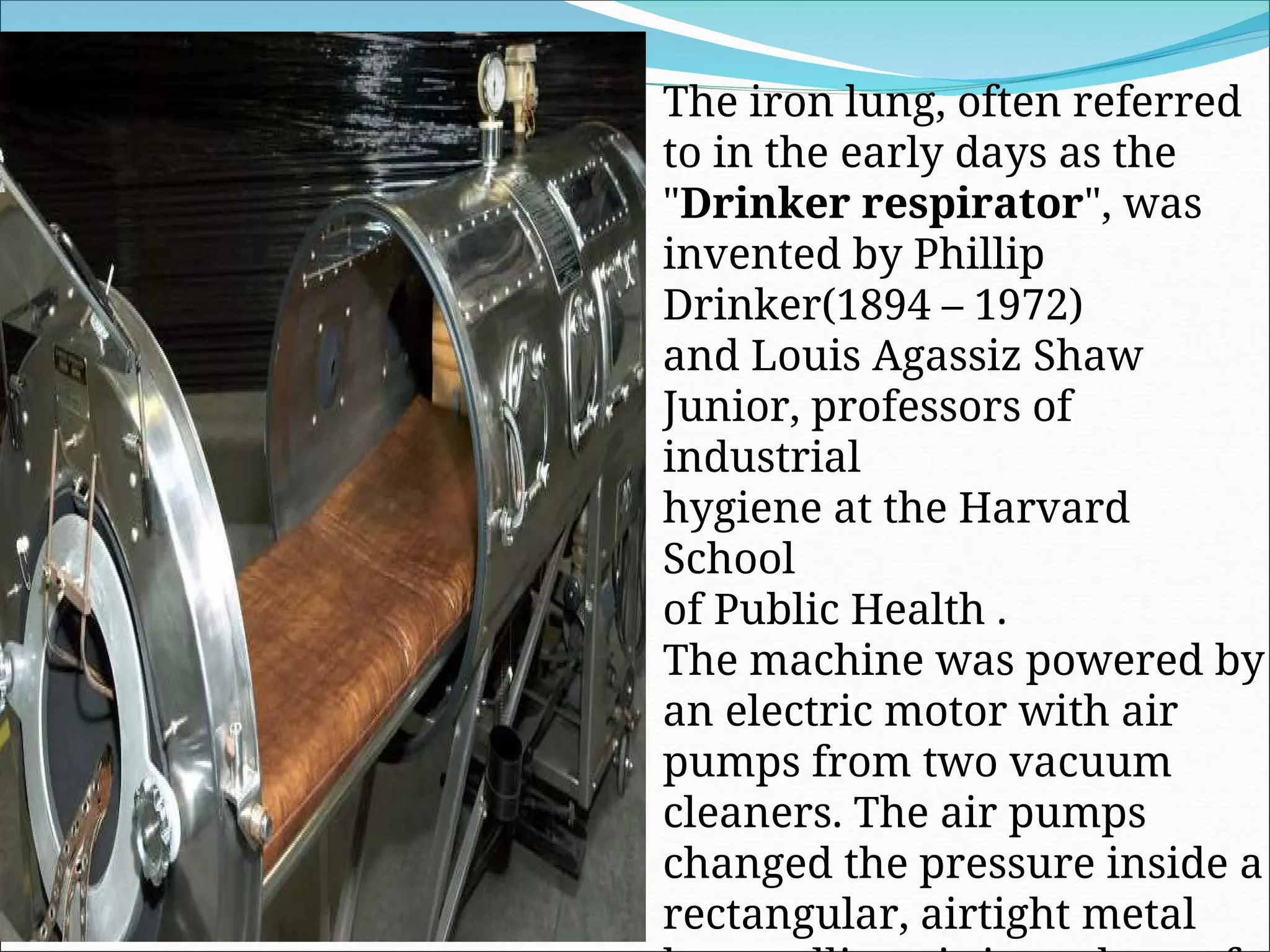
The iron lung,often referred
to in the early days as the
"Drinker respirator", was
invented by Phillip
Drinker(1894 – 1972)
and Louis Agassiz Shaw
Junior, professors of
industrial
hygiene at the Harvard
School
of Public Health .
The machine was powered by
an electric motor with air
pumps from two vacuum
cleaners. The air pumps
changed the pressure inside a
rectangular, airtight metal
23.
Positive pressure ventilators
Inflate the lungs by exerting positive pressure
on the airway, similar to a bellows
mechanism, forcing the alveoli to expand
during inspiration
Expiration occurs passively.
modern ventilators are mainly PPV s and are
classified based on related features,
principles and engineering.
24.
Settings of Mechanical
Ventilation
MechanicalVentilator Settings
regulates the rate, depth and other
characteristics of ventilation.
Settings are based on the patient’s
status (ABGs, Body weight, level of
consciousness and muscle strength)
Trigger
There aretwo ways to initiate a ventilator-delivered breath:
pressure triggering or flow-by triggering
When pressure triggering is used, a ventilator-delivered
breath is initiated if the demand valve senses a negative
airway pressure deflection (generated by the patient trying
to initiate a breath) greater than the trigger sensitivity.
When flow-by triggering is used, a continuous flow of gas
through the ventilator circuit is monitored. A ventilator-
delivered breath is initiated when the return flow is less
than the delivered flow, a consequence of the patient's
effort to initiate a breath
28.
Tidal Volume
Thetidal volume is the amount of air delivered
with each breath. The appropriate initial tidal
volume depends on numerous factors, most
notably the disease for which the patient
requires mechanical ventilation.
29.
Respiratory Rate
Anoptimal method for setting the respiratory
rate has not been established. For most patients,
an initial respiratory rate between 12 and 16
breaths per minute is reasonable
30.
Positive End-Expiratory Pressure
(PEEP)
Applied PEEP is generally added to mitigate end-
expiratory alveolar collapse. A typical initial
applied PEEP is 5 cmH2O. However, up to 20
cmH2O may be used in patients undergoing low
tidal volume ventilation for acute respiratory
distress syndrome (ARDS)
31.
Flow Rate
Thepeak flow rate is the maximum flow
delivered by the ventilator during inspiration.
Peak flow rates of 60 L per minute may be
sufficient, although higher rates are frequently
necessary. An insufficient peak flow rate is
characterized by dyspnea, spuriously low peak
inspiratory pressures, and scalloping of the
inspiratory pressure tracing
32.
Inspiratory Time: ExpiratoryTime
Relationship (I:E Ratio)
During spontaneous breathing, the normal I:E
ratio is 1:2, indicating that for normal patients
the exhalation time is about twice as long as
inhalation time.
If exhalation time is too short “breath stacking”
occurs resulting in an increase in end-expiratory
pressure also called auto-PEEP.
Depending on the disease process, such as in
ARDS, the I:E ratio can be changed to improve
ventilation
33.
Fraction of InspiredOxygen
The lowest possible fraction of inspired oxygen
(FiO2) necessary to meet oxygenation goals
should be used. This will decrease the likelihood
that adverse consequences of supplemental
oxygen will develop, such as absorption
atelectasis, accentuation of hypercapnia, airway
injury, and parenchymal injury
Controlled Mandatory
Ventilation (CMV)
ControlledMechanical Ventilation (CMV).
In this mode the ventilator provides a
mechanical breath on a preset timing. Patient
respiratory efforts are ignored.
This is generally uncomfortable for children and
adults who are conscious and is usually only used
in an unconscious patient. It may also be used in
infants who often quickly adapt their breathing
pattern to the ventilator timing
37.
Asst-Control Mandatory
Ventilation (ACV)
Assist Control (AC). In this mode the ventilator
provides a mechanical breath with either a pre-
set tidal volume or peak pressure every time the
patient initiates a breath.
Traditional assist control used only a pre-set tidal
volume--when a preset peak pressure is used this is
also sometimes termed Intermittent Positive
Pressure Ventilation or IPPV.
However, the initiation timing is the same--both
provide a ventilator breath with every patient
effort.
38.
Assist Control Ventilation
A set tidal volume (if set to volume control) or a
set pressure and time (if set to pressure control)
is delivered at a minimum rate
Additional ventilator breaths are given if
triggered by the patient
39.
In mostventilators a back-up minimum breath
rate can be set in the event that the patient
becomes apnoeic. Although a maximum rate is
not usually set, an alarm can be set if the
ventilator cycles too frequently.
This can alert that the patient is tachypneic or
that the ventilator may be auto-cycling (a
problem that results when the ventilator
interprets fluctuations in the circuit due to the
last breath termination as a new breath
initiation attempt)
40.
Synchronized Intermittent
Mandatory Ventilation(SIMV)
SynchronizedIntermittent Mandatory
Ventilation (SIMV). In this mode the ventilator
provides a pre-set mechanical breath (pressure
or volume limited) every specified number of
seconds (determined by dividing the respiratory
rate into 60 - thus a respiratory rate of 12 results in
a 5 second cycle time).
41.
Within thatcycle time the ventilator waits for
the patient to initiate a breath using either a
pressure or flow sensor. When the ventilator
senses the first patient breathing attempt within
the cycle, it delivers the preset ventilator breath
42.
If thepatient fails to initiate a breath, the
ventilator delivers a mechanical breath at the
end of the breath cycle. Additional spontaneous
breaths after the first one within the breath cycle
do not trigger another SIMV breath.
However, SIMV may be combined with pressure
support. SIMV is frequently employed as a
method of decreasing ventilatory support
(weaning) by turning down the rate, which
requires the patient to take additional breaths
beyond the SIMV triggered breath.
43.
Synchronized Intermittent
Mandatory Ventilation
Breaths are given are given at a set minimal rate,
however if the patient chooses to breath over the set rate
no additional support is given
One advantage of SIMV is that it allows patients to
assume a portion of their ventilatory drive
SIMV is usually associated with greater work of
breathing than AC ventilation and therefore is less
frequently used as the initial ventilator mode
Like AC, SIMV can deliver set tidal volumes (volume
control) or a set pressure and time (pressure control)
Negative inspiratory pressure generated by spontaneous
breathing leads to increased venous return, which
theoretically may help cardiac output and function
44.
Continuous Positive Airway
Pressure(CPAP)
(CPAP). A continuous level of elevated pressure is
provided through the patient circuit to maintain adequate
oxygenation, decrease the work of breathing, and
decrease the work of the heart (such as in left-sided heart
failure — CHF).
Note that no cycling of ventilator pressures occurs and the
patient must initiate all breaths. In addition, no additional
pressure above the CPAP pressure is provided during
those breaths. CPAP may be used invasively through an
endotracheal tube or tracheostomy or noninvasively with
a face mask or nasal prongs
45.
Positive End Expiratory
Pressure(PEEP)
(PEEP)is functionally the same as CPAP, but refers
to the use of an elevated pressure during the
expiratory phase of the ventilatory cycle.
After delivery of the set amount of breath by the
ventilator, the patient then exhales passively. The
volume of gas remaining in the lung after a
normal expiration is termed the functional residual
capacity (FRC).
46.
The FRCis primarily determined by the elastic
qualities of the lung and the chest wall. In many
lung diseases, the FRC is reduced due to collapse
of the unstable alveoli, leading to a decreased
surface area for gas exchange and
intrapulmonary shunting , with wasted oxygen
inspired.
Adding PEEP can reduce the work of breathing
(at low levels) and help preserve FRC.
47.
Pressure Support Ventilation
PressureSupport Ventilation (PSV). When a
patient attempts to breath spontaneously through
an endotracheal tube, the narrowed diameter of
the airway results in higher resistance to airflow,
and thus a higher work of breathing.
PSV was developed as a method to decrease the
work of breathing in-between ventilator
mandated breaths by providing an elevated
pressure triggered by spontaneous breathing
that "supports" ventilation during inspiration
48.
Pressure Support Ventilation
The patient controls the respiratory rate and
exerts a major influence on the duration of
inspiration, inspiratory flow rate and tidal
volume
The model provides pressure support to
overcome the increased work of breathing
imposed by the disease process, the endotracheal
tube, the inspiratory valves and other
mechanical aspects of ventilatory support.
49.
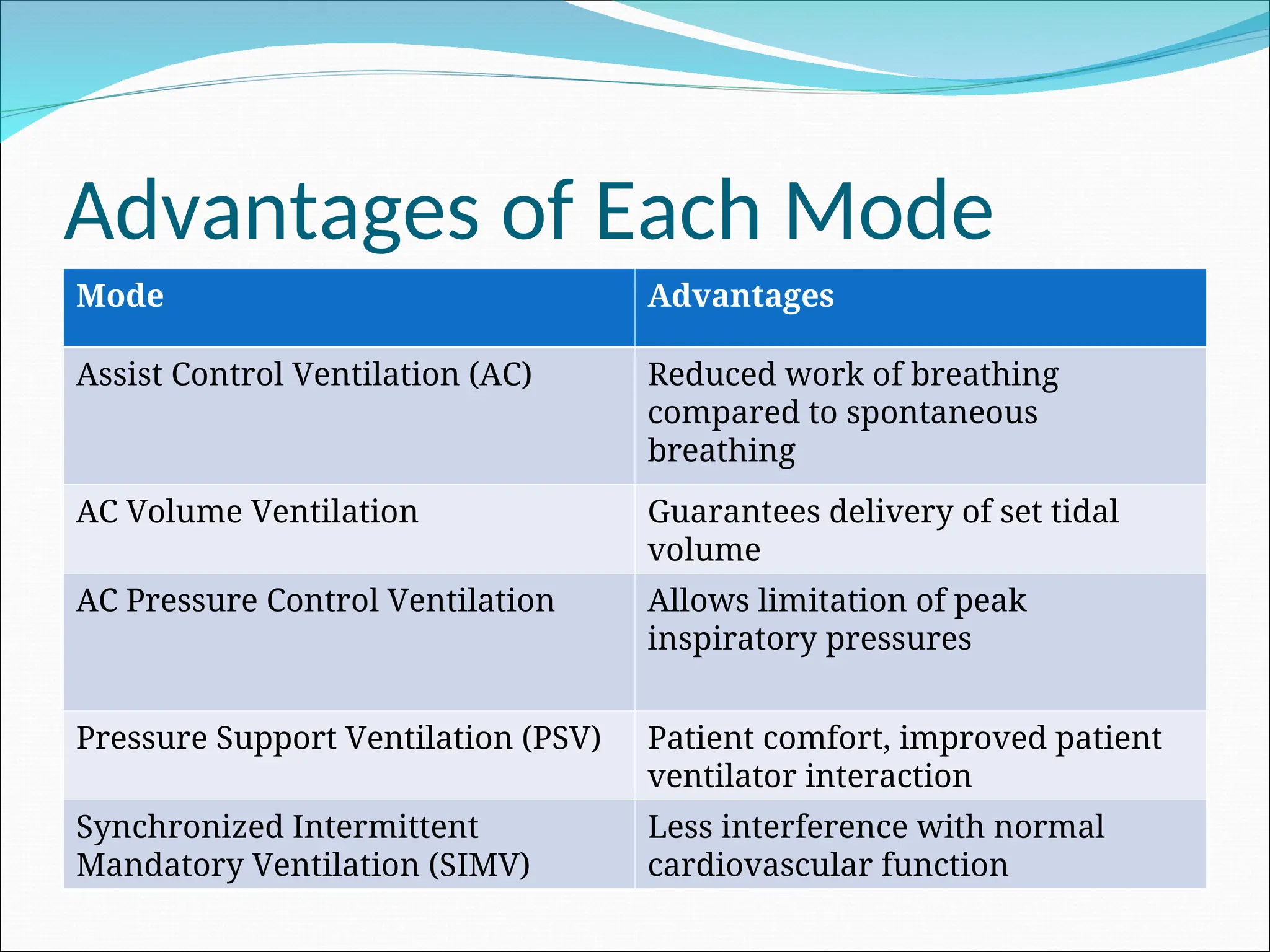
Advantages of EachMode
Mode Advantages
Assist Control Ventilation (AC) Reduced work of breathing
compared to spontaneous
breathing
AC Volume Ventilation Guarantees delivery of set tidal
volume
AC Pressure Control Ventilation Allows limitation of peak
inspiratory pressures
Pressure Support Ventilation (PSV) Patient comfort, improved patient
ventilator interaction
Synchronized Intermittent
Mandatory Ventilation (SIMV)
Less interference with normal
cardiovascular function
50.
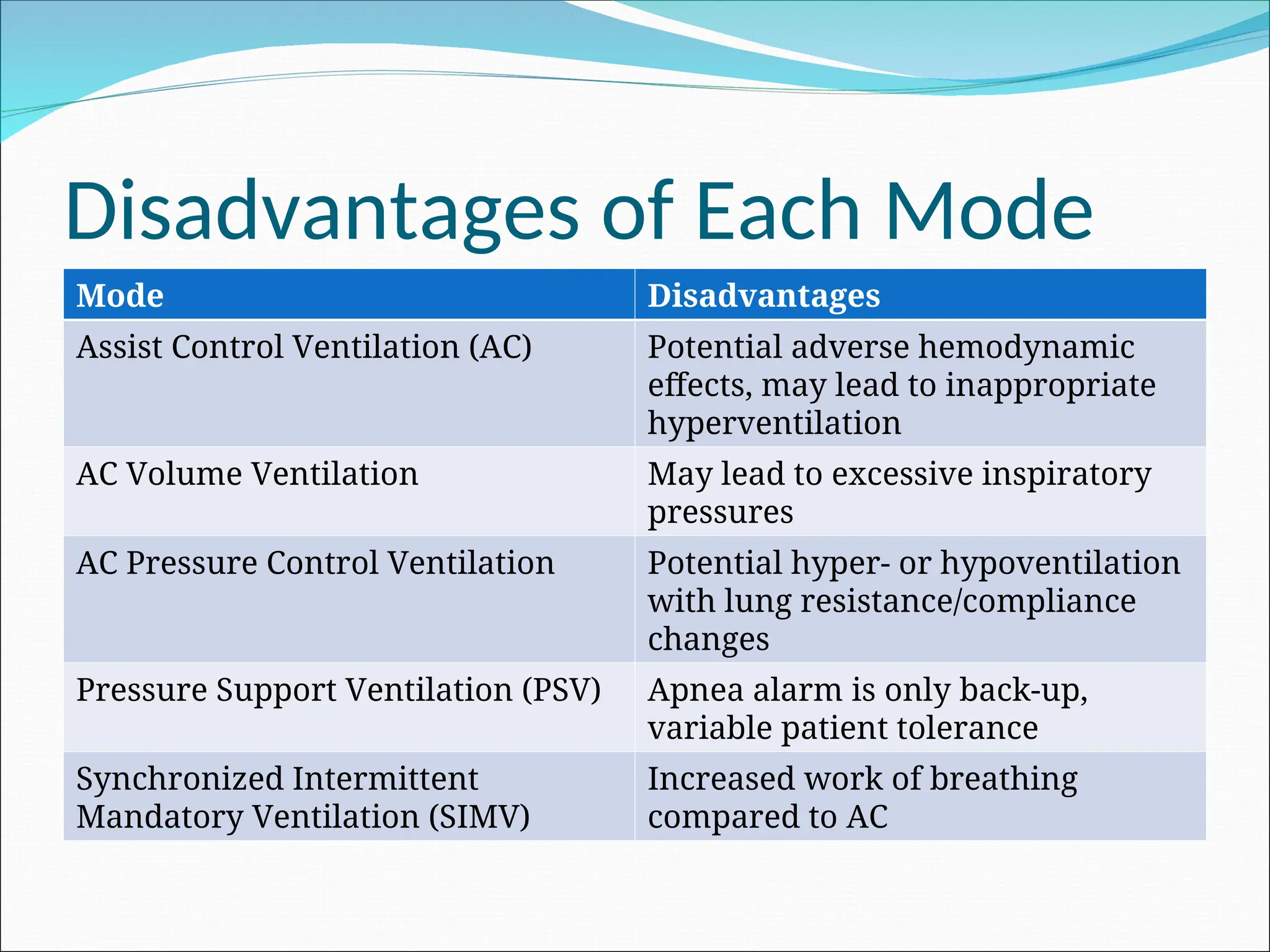
Disadvantages of EachMode
Mode Disadvantages
Assist Control Ventilation (AC) Potential adverse hemodynamic
effects, may lead to inappropriate
hyperventilation
AC Volume Ventilation May lead to excessive inspiratory
pressures
AC Pressure Control Ventilation Potential hyper- or hypoventilation
with lung resistance/compliance
changes
Pressure Support Ventilation (PSV) Apnea alarm is only back-up,
variable patient tolerance
Synchronized Intermittent
Mandatory Ventilation (SIMV)
Increased work of breathing
compared to AC
51.
Guidelines in theInitiation of
Mechanical Ventilation
Primary goals of mechanical ventilation are
adequate oxygenation/ventilation, reduced work
of breathing, synchrony of vent and patient, and
avoidance of high peak pressures
Set initial FIO2 on the high side, you can always
titrate down
Initial tidal volumes should be 8-10ml/kg,
depending on patient’s body habitus. If patient is
in ARDS consider tidal volumes between
5-8ml/kg with increase in PEEP
52.
Guidelines in theInitiation of
Mechanical Ventilation
Use PEEP in diffuse lung injury and ARDS to
support oxygenation and reduce FIO2
Avoid choosing ventilator settings that limit
expiratory time and cause or worsen auto PEEP
When facing poor oxygenation, inadequate
ventilation, or high peak pressures due to
intolerance of ventilator settings consider
sedation, analgesia or neuromuscular blockage
53.
Trouble Shooting theVent
Common problems
High peak pressures
Patient with COPD
Ventilator synchrony
ARDS
54.
Trouble Shooting theVent
If peak pressures are increasing:
Check plateau pressures by allowing for an
inspiratory pause (this gives you the pressure in
the lung itself without the addition of resistance)
If peak pressures are high and plateau pressures
are low then you have an obstruction
If both peak pressures and plateau pressures are
high then you have a lung compliance issue
55.
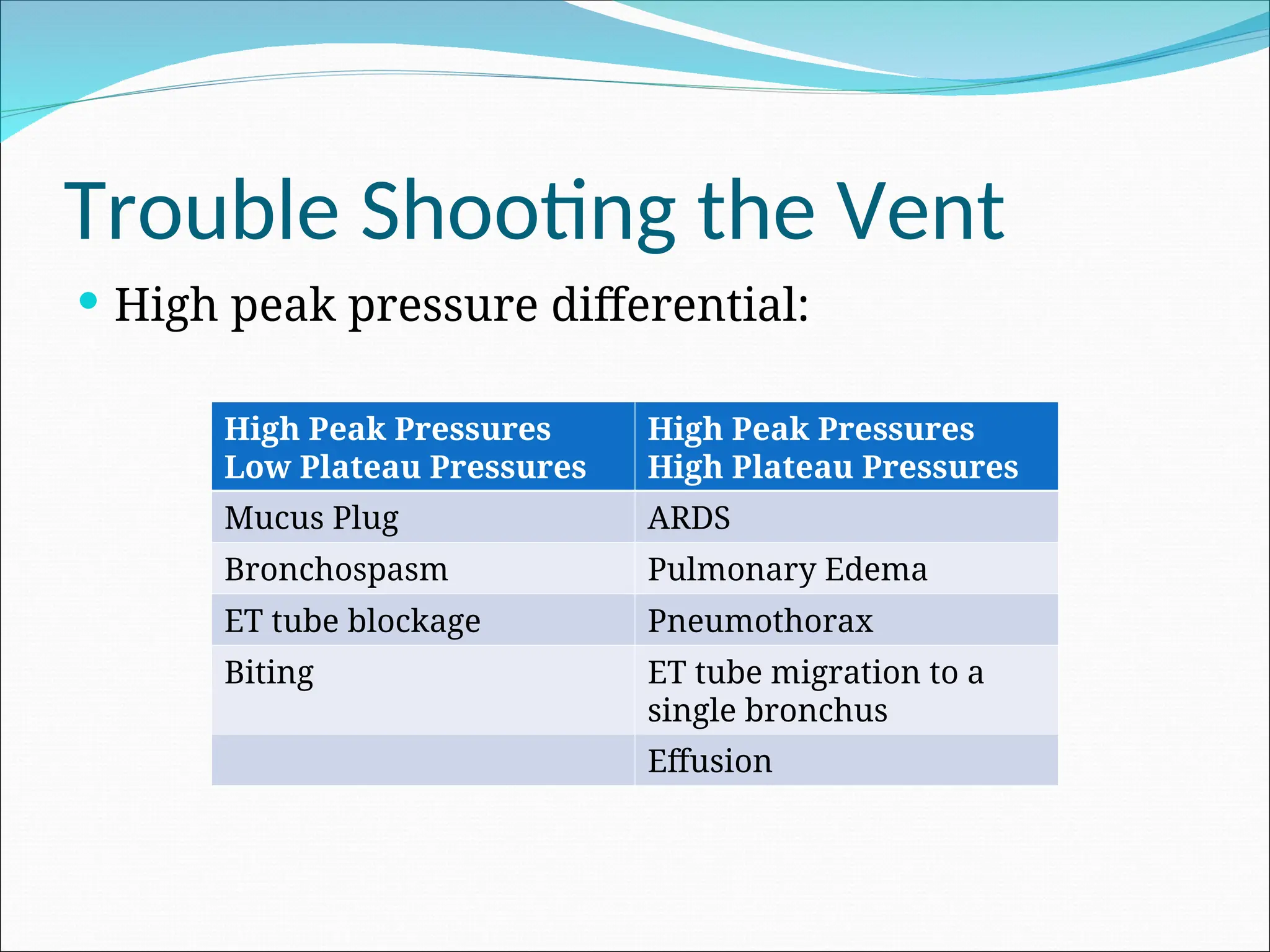
Trouble Shooting theVent
High peak pressure differential:
High Peak Pressures
Low Plateau Pressures
High Peak Pressures
High Plateau Pressures
Mucus Plug ARDS
Bronchospasm Pulmonary Edema
ET tube blockage Pneumothorax
Biting ET tube migration to a
single bronchus
Effusion
56.
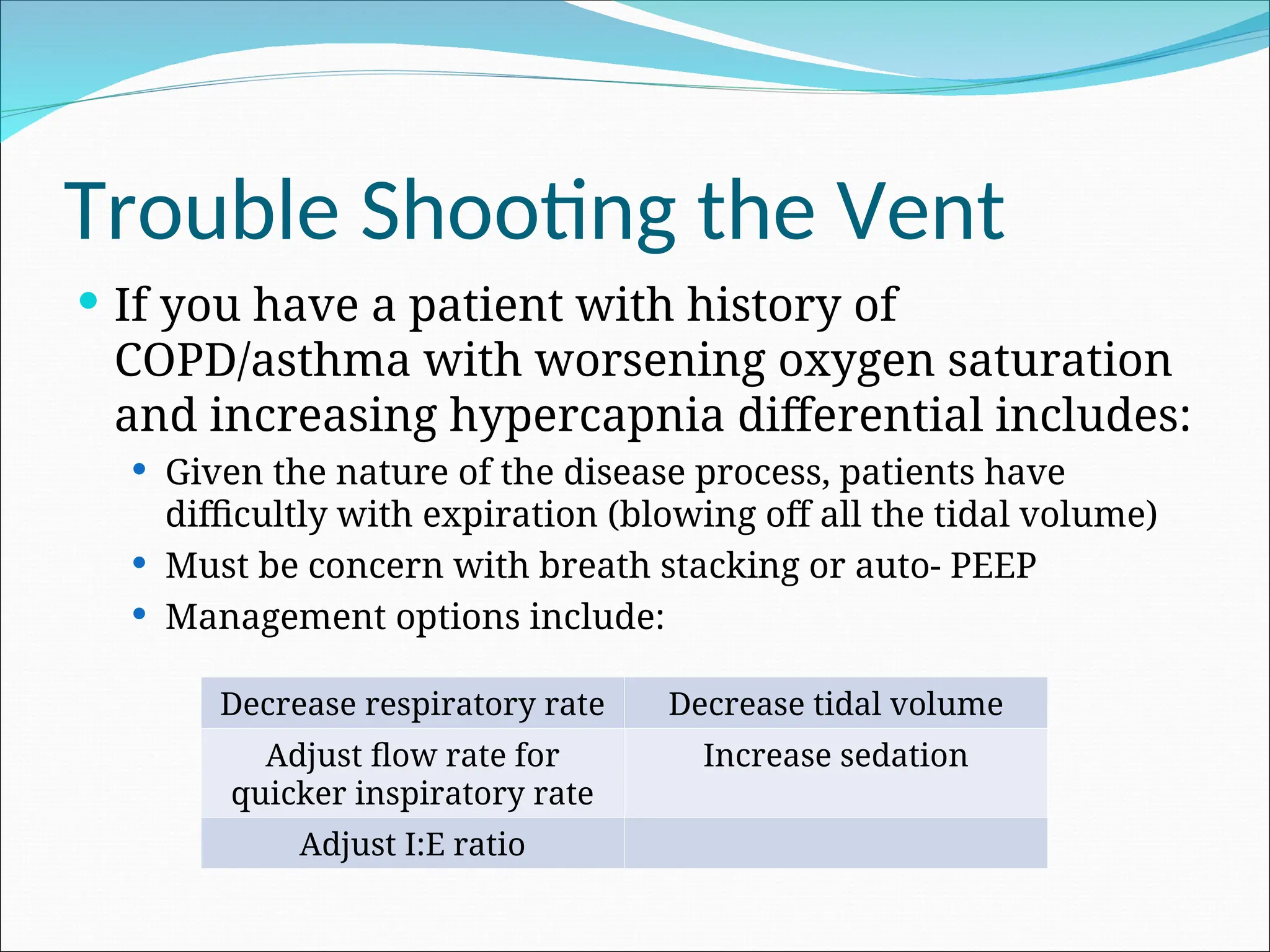
Trouble Shooting theVent
If you have a patient with history of
COPD/asthma with worsening oxygen saturation
and increasing hypercapnia differential includes:
Given the nature of the disease process, patients have
difficultly with expiration (blowing off all the tidal volume)
Must be concern with breath stacking or auto- PEEP
Management options include:
Decrease respiratory rate Decrease tidal volume
Adjust flow rate for
quicker inspiratory rate
Increase sedation
Adjust I:E ratio
57.
Trouble Shooting theVent
Increase in patient agitation and dis-synchrony
on the ventilator:
Could be secondary to overall discomfort
Increase sedation
Could be secondary to feelings of air hunger
Options include increasing tidal volume, increasing
flow rate, adjusting I:E ratio, increasing sedation
58.
Trouble shooting thevent
If you are concern for acute respiratory distress
syndrome (ARDS)
Correlate clinically with HPI and radiologic
findings of diffuse patchy infiltrate on CXR
Obtain a PaO2/FiO2 ratio (if < 200 likely ARDS)
Begin ARDSnet protocol:
Low tidal volumes
Increase PEEP rather than FiO2
Consider increasing sedation to promote synchrony
with ventilator

![History
The roman physician Galen may have been the
first to describe mechanical ventilation: "If you
take a dead animal and blow air through its
larynx [through a reed], you will fill its bronchi
and watch its lungs attain the greatest
distention.”
Vesalius too describes ventilation by inserting a
reed or cane into the trachea of animals.
In 1908 George Poe demonstrated his mechanical
respirator by asphyxiating dogs and seemingly
bringing them back to life.](https://image.slidesharecdn.com/mechanicalvent-250220192251-0e8f8bd3/75/Maintain-medical-mechanical-ventilators-ppt-16-2048.jpg)


![Mechanical_ventilation[_fellow[1][1][1][1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/mechanicalventilationfellow1111-240923152440-d96712e3-thumbnail.jpg?width=640&height=640&fit=bounds)

![Simulation_lecture_11_mechanical_ventillation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/simulationlecture11mechanicalventillation1-240330192829-1f83f7bc-thumbnail.jpg?width=640&height=640&fit=bounds)
















































