Routine administration of magnesium in cardiac arrest does not appear to improve outcomes of return of spontaneous circulation or survival to hospital discharge. However, magnesium may have a neuroprotective effect and some studies have found a trend toward improved neurological function in survivors who received magnesium. Due to insufficient trial size and study power, a small benefit has not been definitively ruled out. Magnesium administration may be considered when arrhythmias are caused by magnesium deficiency or Torsade de Pointes. The evidence does not support routine use of magnesium for cardiac arrest but additional research is still needed.
![101e729e-a9d6-4076-907b-08acaebdd695-150710180423-lva1-app6892.doc Page 1 of
13
REMEMBER TO SAVE THE BLANK WORKSHEET TEMPLATE USING THE FILENAME FORMAT
WORKSHEET for PROPOSED Evidence-Based GUIDELINE RECOMMENDATIONS
NOTE: Save worksheet using the following filename format: Taskforce.Topic.Author.Date.Doc where Taskforce is a=ACLS,
b=BLS, p=Pediatric, n=neonatal and i=Interdisciplinary. Use 2 or 3 letter abbreviation for author’s name and 30Jul03 as
sample date format.
Worksheet Author:
Ross Berringer
Taskforce/Subcommittee: __BLS _x_ACLS __PEDS __ID __PROAD
__Other:
Author’s Home Resuscitation Council:
__AHA __ANZCOR __CLAR __ERC __HSFC
_x_HSFC __RCSA ___IAHF ___Other:
Date Submitted to Subcommittee:
October 25,2004, Revised 25 Nov 2004 Dec 5 2004
STEP 1: STATE THE PROPOSAL. State if this is a proposed new guideline; revision to current guideline; or deletion of current guideline.
Existing guideline, practice or training activity, or new guideline:
Current routine administration of magnesium in resuscitation does not affect outcome and may be associated with a higher incidence of hypotension
despite a potential for improved neurological function in survivors. Magnesium is not recommended in cardiac arrest except when arrythmias are
suspected to be caused by Magnesium deficiency or when Torsade de Pointes is diagnosed. (IIb)
Step 1A: Refine the question; state the question as a positive (or negative) hypothesis. State proposed guideline recommendation as a specific,
positive hypothesis. Use single sentence if possible. Include type of patients; setting (in- /out-of-hospital); specific interventions (dose, route); specific
outcomes (ROSC vs. hospital discharge).
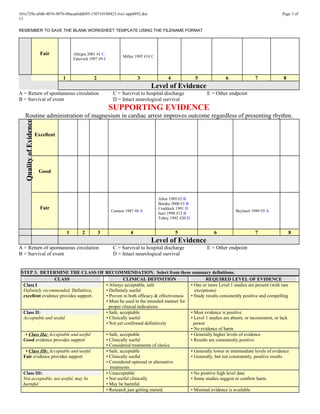
Routine administration of magnesium in cardiac arrest improves outcome regardless of presenting rhythm.
Step 1B: Gather the Evidence; define your search strategy. Describe search results; describe best sources for evidence.
Medline, AHA Endnote, EMBASE, and Cochrane searched using MeSH terms <heart arrest> not <heart arrest induced> and <magnesium>,
<ventricular fibrillation> and <magnesium>, free text search cardiac arrest and magnesium, ventricular fibrillation and magnesium, in hospital
cardiac arrest and magnesium, out of hospital cardiac arrest and magnesium.
List electronic databases searched (at least AHA EndNote 7 Master library [http://ecc.heart.org/], Cochrane database for systematic reviews and Central Register
of Controlled Trials [http://www.cochrane.org/], MEDLINE [http://www.ncbi.nlm.nih.gov/PubMed/ ], and Embase), and hand searches of journals, review articles,
and books.
Medline (1966 – 06/04), Embase 06/04, AHA Endnote Database 07/04, Cochrane Database of Systematic Reviews, and Cochrane Controlled Trials
Registry. Medline 200 free text/ related articles and 62 MeSH, EMBASE 84 MeSH, Cochrane Central Register 35 MeSH, Cochrane Database of
Systematic Reviews 0, AHA End Note 59 free text.
• State major criteria you used to limit your search; state inclusion or exclusion criteria (e.g., only human studies with control group? no animal studies? N subjects
> minimal number? type of methodology? peer-reviewed manuscripts only? no abstract-only studies?)
No limits applied to any search.
Excluded: animal studies, cardioplegic/anaesthetic studies, letters, guidelines, editorials, conference proceedings, and opinions.
Additional references were excluded after review of the abstract or article as not relevant or meeting exclusionary criteria above
Hand searching of bibliographies of published reviews yielded only occasional case reports.
• Number of articles/sources meeting criteria for further review: Create a citation marker for each study (use the author initials and date or Arabic numeral, e.g.,
“Cummins-1”). . If possible, please supply file of best references; EndNote 6+ required as reference manager using the ECC reference library.
17 articles were selected for further detailed review
STEP 2: ASSESS THE QUALITY OF EACH STUDY
Step 2A: Determine the Level of Evidence. For each article/source from step 1, assign a level of evidence—based on study design
and methodology.
Level of
Evidence
Definitions
(See manuscript for full details)
Level 1 Randomized clinical trials or meta-analyses of multiple clinical trials with substantial treatment effects
Level 2 Randomized clinical trials with smaller or less significant treatment effects
Level 3 Prospective, controlled, non-randomized, cohort studies
Level 4 Historic, non-randomized, cohort or case-control studies
Level 5 Case series: patients compiled in serial fashion, lacking a control group
Level 6 Animal studies or mechanical model studies
Level 7 Extrapolations from existing data collected for other purposes, theoretical analyses
Level 8 Rational conjecture (common sense); common practices accepted before evidence-based guidelines](https://image.slidesharecdn.com/101e729e-a9d6-4076-907b-08acaebdd695-150710180423-lva1-app6892/85/magnesium-cardiac-arrest-1-320.jpg)









![101e729e-a9d6-4076-907b-08acaebdd695-150710180423-lva1-app6892.doc Page 12
of 13
REMEMBER TO SAVE THE BLANK WORKSHEET TEMPLATE USING THE FILENAME FORMAT
Sarkozy 2003 #18
Thel 1997 #19
M+S (P = 0.21). A temporal association between M administration and first return of spontaneous
circulation (ROSC) was also documented in 4 of 10 M+S patients (pulseless electrical activity
(3)/pulseless VT (1)), who had first ROSC/R occur within 0.5-2.25 min following first i.v. M bolus
delivery, after 11-30 min (mean = 20 min) of continuous pulseless rhythm refractory to standard
ACLS. All M+S resuscitations occurred within the dose range 2.5-5 g (i.v. push): 3/6 (50%) and
7/13 (54%) R occurred with 1-3 g and 4-5 g MgSO4, respectively (at least 11/13 patients had
peripheral i.v. delivery with 4-5 g M). Analyzing post-ROSC hypotension proved important, as 50%
of pts with first recorded systolic BP post-ROSC < 90 mmHg were resuscitated vs. 83% with > 90
mmHg (P = 0.10). A trend toward increased post-ROSC hypotension was evidenced with i.v.
MgSO4: Recorded first or second systolic BP < 90 mmHg post-ROSC occurred in 66% of M+S vs.
42% of SA patients. All 3 M+S patients having a wide open i.v. levophed infusion as vasopressor
support, started immediately post-ROSC/i.v. MgSO4 with systolic BP < 90 mmHg and continued at
least 15 min (titrating to a systolic BP approximately 110 mmHg), had a temporal association
between M delivery and R after 14-30 min of continuous pulselessness refractory to S.
CONCLUSION: Human research determining whether i.v. MgSO4 increases long-term survival
from refractory cardiac arrest should be vigorously pursued, as it is safe to proceed given the above
described considerations.
Quality of evidence: Poor
Level of evidence: 3
Type of evidence: Neutral/Opposing
Setting: In hospital cardiac arrests
Comments: Non randomized open label in hospital treatment at MD discretion
Non standardized endpoints
Neurological endpoints poorly defined
Almost unreadable due to convoluted prose
Sarkozy, A. and P. Dorian (2003). "Strategies for reversing shock-resistant ventricular fibrillation." Curr Opin
Crit Care 9(3): 189-93.
PURPOSE OF REVIEW: Shock-resistant ventricular fibrillation is defined as ventricular fibrillation
persisting after three defibrillation attempts. In approximately 10 to 25% of all cardiac arrests,
shock-resistant ventricular fibrillation develops, and 87 to 98% of these patients die. RECENT
FINDINGS: In the treatment of shock-resistant ventricular fibrillation, defibrillation using biphasic
waveforms is considered as an intervention of choice. Intravenous amiodarone is also acceptable,
safe, and useful, based on evidence from two randomized clinical trials. Intravenous vasopressin is
acceptable and probably safe and useful, but the evidence supporting this recommendation is coming
from a small, randomized clinical trial. Procainamide is acceptable but not recommended. In the
presence of acute myocardial infarction and recurrent ventricular fibrillation, if all other therapies
fail, beta-blockers can be considered. Magnesium, lidocaine, and bretylium are not recommended in
the treatment of shock-resistant ventricular fibrillation. SUMMARY: Biphasic defibrillation and
intravenous amiodarone are useful in shock-resistant ventricular fibrillation.
Comment: Review article
Thel, M. C., A. L. Armstrong, et al. (1997). "Randomised trial of magnesium in in-hospital cardiac arrest.
Duke Internal Medicine Housestaff." Lancet 350(9087): 1272-6.
BACKGROUND: The apparent benefit of magnesium in acute myocardial infarction, and the
persistently poor outcome after cardiac arrest, have led to use of magnesium in cardiopulmonary
resuscitation. Because few data on its use in cardiac arrest were available, we undertook a
randomised placebo-controlled trial (MAGIC trial). METHODS: Patients treated for cardiac arrest
by the Duke Hospital code team were randomly assigned intravenous magnesium (2 g [8 mmoles]
bolus, followed by 8 g [32 mmoles] over 24 h; 76 patients) or placebo (80 patients). Only patients in
intensive care or general wards were eligible; those whose cardiac arrest occurred in emergency,
operating, or recovery rooms were excluded. The primary endpoint was return of spontaneous
circulation, defined as attainment of any measurable blood pressure or palpable pulse for at least 1 h
after cardiac arrest. The secondary endpoints were survival to 24 h, survival to hospital discharge,
and neurological outcome. Analysis was by intention to treat. FINDINGS: There were no significant
differences between the magnesium and placebo groups in the proportion with return of spontaneous](https://image.slidesharecdn.com/101e729e-a9d6-4076-907b-08acaebdd695-150710180423-lva1-app6892/85/magnesium-cardiac-arrest-12-320.jpg)
![101e729e-a9d6-4076-907b-08acaebdd695-150710180423-lva1-app6892.doc Page 13
of 13
REMEMBER TO SAVE THE BLANK WORKSHEET TEMPLATE USING THE FILENAME FORMAT
Tobey 1992 #20
Vincent 1997 #21
circulation (41 [54%] vs 48 [60%], p = 0.44), survival to 24 h (33 [43%] vs 40 [50%], p = 0.41),
survival to hospital discharge (16 [21%] vs 17 [21%], p = 0.98), or Glasgow coma score (median 15
in both). INTERPRETATION: Empirical magnesium supplementation did not improve the rate of
successful resuscitation, survival to 24 h, or survival to hospital discharge overall or in any
subpopulation of patients with in-hospital cardiac arrest.
Quality of evidence: Good
Level of evidence: 2
Type of evidence: Neutral/Opposing
Setting: In hospital university tertiary care institution
Comment: Neuro outcome by Karnofsky score (?) better in Mg group
Underpowered for small treatment effect, 5% improval would need 2000 pts
Different pt population than OHCA
Response times very short
40% patients admitted with pre established cvs diagnosis
Tobey, R. C., G. A. Birnbaum, et al. (1992). "Successful resuscitation and neurologic recovery from refractory
ventricular fibrillation after magnesium sulfate administration." Ann Emerg Med 21(1): 92-6.
A 46-year-old man suffered a witnessed cardiac arrest. Ventricular fibrillation persisted despite 62
minutes of basic and advanced cardiac life support measures in the field. On arrival in the
emergency department, he received 4 g magnesium sulfate IV and was defibrillated successfully to
normal sinus rhythm with the next countershock. The patient was discharged neurologically intact.
We discuss the possible mechanisms of action and clinical use of IV magnesium sulfate in cardiac
arrest.
Quality of evidence: Poor
Level of evidence: 5 (?)
Type of evidence: Supportive
Setting: Out of hospital arrest
Comment: Witnessed EHS on scene
Vincent, R. (1997). "Drugs in modern resuscitation." Br J Anaesth 79(2): 188-97.
Review article
*Type the citation marker in the first field and then paste the full citation into the second field. You can copy the full citation
from EndNote by selecting the citation, then copying the FORMATTED citation using the short cut, Ctrl-K. After you copy the
citation, go back to this document and position the cursor in the field, then paste the citation into the document (use Ctrl-V). For each
new citation press Tab to move down to start a new field.](https://image.slidesharecdn.com/101e729e-a9d6-4076-907b-08acaebdd695-150710180423-lva1-app6892/85/magnesium-cardiac-arrest-13-320.jpg)















































