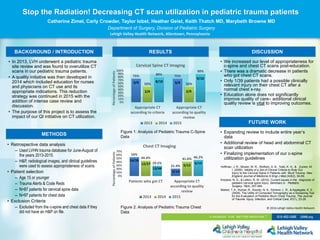
This document summarizes a quality initiative at Lehigh Valley Health Network to decrease CT scan utilization for pediatric trauma patients. The initiative included educating nurses and doctors on appropriate CT usage and indications, as well as intensive case review. Data was analyzed from 2013-2015 on pediatric trauma patients who received cervical spine or chest CT scans. Results showed that after education and review, the percentage of appropriate CT scans increased, with a dramatic decrease in chest CT scans. While education improved care, additional clinical review was needed. Future work includes expanding the study and implementing cervical spine guidelines.