
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (13)
Similar to Susan Schwabe Hourly Rounding 2014
Similar to Susan Schwabe Hourly Rounding 2014 (20)
Susan Schwabe Hourly Rounding 2014
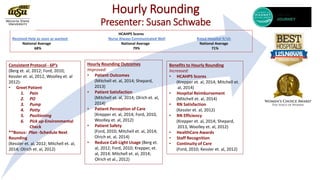
- 1. Hourly Rounding Presenter: Susan Schwabe HCAHPS Scores Received Help as soon as wanted: Nurse Always Communicated Well Rated Hospital 9/10: National Average National Average National Average 68% 79% 71% Hourly Rounding Outcomes Improved: • Patient Outcomes (Mitchell et. al, 2014; Shepard, 2013) • Patient Satisfaction (Mitchell et. al, 2014; Olrich et. al, 2014) • Patient Perception of Care (Krepper et. al, 2014; Ford, 2010, Woolley et. al, 2012) • Patient Safety (Ford, 2010; Mitchell et. al, 2014; Olrich et. al, 2014) • Reduce Call-Light Usage (Berg et. al, 2012; Ford, 2010; Krepper, et. al, 2014; Mitchell et. al, 2014; Olrich et al., 2012) Consistent Protocol - 6P’s (Berg et. al, 2012; Ford, 2010; Kessler et. al, 2012, Woolley et. al 2012): • Greet Patient 1. Pain 2. PO 3. Pump 4. Potty 5. Positioning 6. Pick up-Environmental Check **Bonus: Plan -Schedule Next Rounding (Kessler et. al, 2012; Mitchell et. al, 2014; Olrich et. al, 2012) Benefits to Hourly Rounding Increased: • HCAHPS Scores (Krepper et. al, 2014; Mitchell et. al, 2014) • Hospital Reimbursement (Mitchell et. al, 2014) • RN Satisfaction (Kessler et. al, 2012) • RN Efficiency (Krepper et. al, 2014; Shepard, 2013, Woolley et. al, 2012) • HealthCare Awards • Staff Recognition • Continuity of Care (Ford, 2010; Kessler et. al, 2012)
- 2. Hourly Rounding Presenter: Susan Schwabe Accountable Care Facts. (2012). Retrieved from http://www.accountablecarefacts.org/ Berg, K., Sailors, C., Reimer, R., O’Brien, Y., Ward-Smith, P. (2012). Hourly Rounding With a Purpose. The Iowa Nurse Reporter, 12-14. Brewer, J., Shoulders, A., Emmons, K. (2010). Mind Your Mommies! Our Hospital’s Story of Hourly Rounding on the Obstetric Patient. Journal of Obstetrics and Gynecological Nursing, 39(1), S49-S50. Centers for Medicare and Medicaid Services. (2014). Hospital Compare. Retrieved from http://www.Medicare.gov Ford, B. (2010).Hourly Rounding: A Strategy to Improve Patient Satisfaction Scores. MedSurg Nursing, 19(3), 188-191. Kessler, B., Claude-Gutekunst, M., Donchez, A., Dries, R. & Snyder, M. (2012). The Merry-Go-Round of Patient Rounding: Assure Your Patients Get The Brass Ring. MedSurg Nursing, 21(4),240-245. Krepper, R., Vallejo, B., Smith, C., Lindy, C., Fullmer, C., Messimer, S., Xing, Y., & Meyers, K. (2014, March/April). Evaluation of a Standardized Hourly Rounding Process (SHaRP). Journal for Healthcare Quality, 36(2), 62-69. Mitchell, M., Lavenberg, J., Trotta, R., & Umscheid, C. (2014, September). Hourly Rounding to Improve Nursing Responsiveness A Systematic Review. The Journal of Nursing Administration, 44(9), 462-472. Olrich, T., Kalman, M. & Nigolian, C. (2012). Hourly Rounding: A Replication Study. MedSurg Nursing, 21(1), 23-36. Shepard, L. (2013, February). Stop Going in Circles! Break the Barriers to Hourly Rounding. Nursing Management, 13-15. Retrieved from http://www.nursingmanagement.com University of Kansas Hospital. (2014). Magnet Redesignation. Retrieved from http://www.kumed.com U.S. News & World Report. (2014). U.S. News Best Hospitals 2014-2015. Retrieved from http://health.usnews.com/best-hospitals/rankings Woolley, J., Perkins, R., Laird, P., Palmer, J., Schitter, M.B., Tarter, K., George, M., Atkinson, G., McKinney, K., & Woolsey, M. (2012, May-June). Relationship-Based Care: Implementing a Caring, Healing Environment. MedSurge Nursing, 21(3), 179-184. WomenCertified Inc. (2014).Women’s choice award America’s Best Hospitals for Obstetrics Award methodology. Retrieved from http://www.Womenschoiceaward.com
Editor's Notes
- Introduction: Welcome to my P-Party (popcorn, Pretzels, Punch) (Woolley et. al, 2012). How does your Hourly Rounding Effect the Big Picture? Direct Correlation between Hourly Rounding Rates and HCAHPS Scores and Hospital Reimbursement. Lets Start with Hospital Reimbursement: Our current climate in healthcare reimbursement is value-based reimbursement directly tied to HCAHPS(hospital consumer assessment of healthcare providers and systems survey) patient satisfaction scores (Mitchell et. al, 2014). The Affordable Care Act’s most significant contribution is a provision that allows Medicare to reward HC organizations with a share of the savings that would result from improving care quality and reducing cost for Medicare populations. In order to participate in this “shared savings program” a hospital must become an Accountable Care Organization. The true value of ACOs is determined by assessing improvements in quality while being cost effective. This means, ACOs are rewarded for outcomes, not volume of services. Outcomes are based on HCAHPS Scores. ACOs also receives reduced reimbursement due to HCAHPS scores below the national average. (Accountable Care Facts, 2012). HCAHPS Scores: Patients in the hospital are under a great deal of stress with new medical conditions an unfamiliar environment in which they are unaware of hospital routines and access the one mechanism at their disposal for getting their needs met, the call button (Mitchell et. al, 2014). A few Key HCAHPS Scores that point to patient satisfaction are did the patient feel “they receied help as soon as they wanted,” did the “nurse always communicate well,” and would they “rate this hospital a 9/10” (CMM, 2014). Research tells us that relationship based care based on hourly rounding improved patient satisfaction through a reduction in call light by 52%, increased efficiency of nurses by 20%, decrease in patient falls by 12%. Patients reported their pain was better managed and nurses reported more time for documentation and patient education. Hourly rounding hitting the 6 P’s. Over 2 years, HCAHPS scores increased: Patients reported Nurses treated with with courtesy and respect 100%; nurses listed to me carefully 86%; nurses explained in a way I understood 86%; communication with nurses good 90%. Problem: Nurses, typically have a 1:6 ratio, weighted with prioritizing complexity of care for pts with different levels of acuity and safety needs sometimes requiring an extended period of time in one patient’s room while another patient believes their own need is urgent as well resulting in a delay in response to the call light. Consistent Protocol- The 6 P’s: Pain-Pain Assessment, TCDB, Diversion PO-Medications Pump-Check, Plan Potty-Toileting, Reassuring Presence of RN Positioning-Comfort, Skin/Sheets/Pillows Pick up-Environmental Check, Call light/water/phone, Bedside Table, Tissues Any Other needs, I have time right now. I’ll be back in an hour. Extra Info: Mitchell et. al 2014: Structured Hourly Rounding can address the Top 5 reasons for pressing call light and help the RN provide uninterrupted, more responsive care:: Pain mgmt., personal assistance, bathroom assistance, equipment/alarms. Olrich et. al (2012): The following items will be checked for each patient: 1. Nursing staff enter room, greet patient, and say, “Hi, Mrs./Mr. Jones, I am here to do my rounds to check on your comfort.” 2. Pain assessment using a pain intensity scale (if staff other than RNs are rounding and the patient is in pain, RNs will be contacted immediately by the person rounding so the patient does not have to use the call light for analgesia). 3. An hour prior to analgesia is due, the patient will be asked if she/he is starting to feel pain. If the answer is “yes,” the RN will schedule analgesia administration. 4. Toileting assistance will be offered. 5. A patient positioning and comfort assessment will occur, including covering the patient if needed. 6. Environmental check • Call light within reach • Telephone within reach • TV control and bed light switch within reach • Bedside table close to bed • Tissue box and water within reach 7. Prior to leaving the room, each staff member asks, “Is there anything I can do for you before I leave? I have time to do it.” 8. Staff also will tell the patient when rounding next will be conducted (in 1 hour). Consistent actions during hourly rounding: Lehigh Valley Hospital-Muhlenberg Campus, Bethlehemn PA“Is there anything I can do for you before I leave? Right now I have the time. We’ll be back in an hour to check on you.” 6T at LVHMC researched hourly rounding for 6 years and found working together to determine the tailored protocol that worked best for their floor to improve patient satisfaction and nurse indicators. Now, they hold staff meetings on their floor for other units implementing hourly rounding and have made an overarching impact on HCAHPS Scores for the hospital on the whole (Kessler et. al, 2012). Hourly Rounding Outcomes Based on the equivalent of 10 year of studies (Mitchell et. al, 2014): Patient Outcomes/ Patient Satisfaction: More than 16 published studies found statistically significant evidence that hourly rounding has beneficial effects on patient outcomes and satisfaction scores on HCAHPS and NDNQI Nursing Indicators. (Mitchell et. al, 2014, Shepard, 2013, Olrich et al, 2014, Woolley et al, 2012, Krepper et al, 2014 and Ford, 2010). Brewer et. al(2010) provided the only information pertaining to hourly rounding on the Obstetric patient and found benefits of hourly rounding in that the patients received the time and attention in clustering care, which allowed them to rest or bond with their infant. Areas of focus were pain, anticipating needs and improved patient experience, as well as receive needed education regarding self care, baby, lactation and bonding as a family unit. Patient Perception: : Patient value RN relationship, continuity of care, trust, compassion, respect, safety, understandable instructions, service quality, reliability, responsiveness and effective communication. Hourly rounding is a key component to impacting the patient perception of quality services and satisfaction.(Ford, 2010). Patient Safety: Key mandate of TJC is improved patient safety (Ford 2010). Nine studies reported a reduction in falls ranging from 24%-80%. (Mitchell et. al, 2014) Reduced Call Light Usage: Ten studies of hourly rounding on effects of call light usage showed decrease in usage range from 23%-70% (Mitchell et. al, 2014). That’s an “Overall call-light usage decreased an average of 33% per patient, per day.” Specifically, patients who used the call-light to: request pain medication and toileting These results support the hypothesis that providing these activities routinely reduces unnecessary steps and decreases interruptions in work flow for RNs. Thus, implementing this activity should be considered by healthcare facilities, as an evidenced-based practice”(Berg et al., 2012). Benefits of hourly rounding: HCAHPS Scores: HCAHPS patient satisfaction scores increased almost 10 percentage points after implementation of hourly rounding (Krepper et. al, 2014). HCAHPS scores are publically reported and are linked to Medicare reimbursement levels. They highlight 2 questions pertaining to response to call button and getting expeditious help with toileting. Proactive and regular checks decrease patient anxiety, call light use, minimizes patient uncertainty (Mitchell et. al, 2014). Hospital Reimbursement: In our current HC climate of value based purchasing, reimbursements are directly tied to patient satisfaction scores and RN responsiveness is an important factor in patient perception of care which is captured in patient satisfaction surveys (Mitchell et. al 2014). Staff satisfaction: Kessler et. al six year study resulted with the Hospital Staff satisfaction with increased camaraderie, benefits of taking a proactive-timely approach, having more control over the work, identifying tasks that might have been missed. They found when rounds were not done there was chaos. Staff Efficiency: Pedometers were worn by RNs before and after implementation of hourly rounding and they found that the number of steps decreased with hourly rounding resulting from a more efficient approach to meeting patient care needs in a proactive manner (Krepper et al, 2014, Shepard, 2013, Woolley et al, 2012). Shepard, 2013: For RNs with 1:6+ ratio on high acuity medsurg units with IV pump alarms, documentation demands, new technology, have found hourly rounding was a key to time management. When a patient understands that the RN will visit their room every hour, they are less likely to request assistance between rounds. The decrease in interruptions, allows RNs to work efficiently and productively. Krepper et al (2014) assessed efficiency of delivery of care: nursing staff wore pedometers and were able to show decreased number of steps walked in a shift by doing hourly rounding. Since 2005 Research has demonstrated the benefits including saving valuable time. Address pain mgmt., elimination, nourishment, ambulation/positioning (Shepard, 2013). Staff Recognition: Unit Award, Performance Review Consistent ProtocolContinuity of Patient Care Facility Reputation: Community Recognition Awards and Designations (see below): Community Recognition/Awards: Why is it important to be seen on the radar? Patient Choice. What are patients turning to determine where they will pursue medical treatment? Research the Web….what do they find on the web rating hospitals? -Hospital Compare, HCAHPS Scores -American Nurses Credentialing Center-Magnet Designation -Women’s Choice Award -US News and World Report Best Hospitals Rankings -Word of Mouth Hospital Compare: HCAHPS Scores Magnet Recognition Program: Recognizes the important role nurses play in hospital’s ability to provide the very best in patient care and patient outcomes. University of Kansas Hospital is a Magnet hospital which attracts nurses because nurses are encouraged and appreciated, the hospital is committed to patient care and outcomes and provides higher quality care, lower mortality rates, significantly higher levels of patient satisfaction and consumer confidence as well as greater success in recruiting and retaining the best nurses. Only 393 hospitals worldwide hold Magnet designation. US News and World report Hospital Rankings in Cancer and gyn are based on hard data. Gynecology: Mayo Clinic 100/100. #1 Ranking; Brigham and Women’s 91.4/100 Ranked #2. Ranked #50th: scored a 69.7/100 score. University of Kansas Hospital Ranked #38th with score of 71.1/100 In addition to reimbursement, hospitals are publically acknowledged with Women’s Choice Awards and Ranked according to HCAHPS ratings. These ratings and Awards attract future patients/clients of the medical center which impact job security, ANCC magnet recognition program which recognizes quality pt care, nursing excellence and innovations in professional nursing which in turn attracts and retains nurses at a medical center. The greater Wichita, KS area Women’s Choice Award Recipients in OB 2014: Newton Medical Center and Via Christi St. Theresa. Female Recommendation Rating. Award methodology in a nut shell uses HCAHPS scores(patient satisfaction) coupled with frequency of incidence of problems(errors, infections) to the Centers for Medicare and Medicaid Services for 12 measures of quality (death, collapsed lung, blood clots, wound evisceration, cuts/tears, complications, CLABSI, CAUTI, SSI: colon, SSI: Hysterectomy, MRSA, C.diff). We cannot separate clinical performance from patient experience. Female recommendation rating based on pt feedback and low rates of infection or serious complications