Objectives of theSeminar
• To understand the role of liver examination in autopsy
• To learn standard grossing technique
• To recognize normal and abnormal gross appearances
• To know correct tissue sampling
• To correlate liver pathology with clinical findings
3.
The stages thatfollow shortly after death are:
•Corneal opacity, "clouding" in the eyes
•Pallor mortis, paleness which happens in the first 15–
120 minutes after death
•Livor mortis, or dependent lividity, a settling of the
blood in the lower (dependent) portion of the body
•Algor mortis, the reduction in body temperature
following death. This is generally a steady decline
until matching ambient temperature
•Rigor mortis, the limbs of the corpse becoming stiff
(Latin rigor) and difficult to move or manipulate
•Putrefaction, the beginning signs of decomposition
11.
Liver specimens maybe taken as isolated organs or as part of a multiple-viscera
examination.
Percutaneous core biopsies can also be performed postmortem to obtain diagnostic
tissue, especially when a full autopsy is not possible due to religious objections or
other constraints.
12.
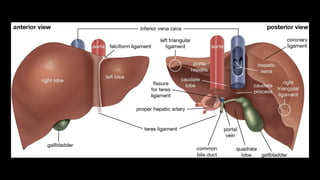
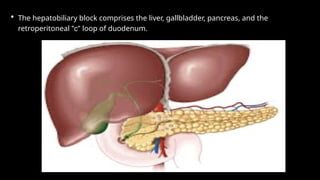
• The hepatobiliaryblock comprises the liver, gallbladder, pancreas, and the
retroperitoneal "c" loop of duodenum.
13.
This block isapproached from its posterior surface.
Extraneous fat is removed as well as the mesentery of the small intestine.
irm, sustained pressure on the gallbladder should express bile through the bile duct and ampu
The inferior vena cava is examined and removed.
14.
• Next, asuperficial transverse incision across the hepatoduodenal ligament is
made with the intent of entering the portal vein.
• Using scissors, open the portal vein toward and away from the liver to establish
its patency. If it is free of pathology, then it may be transected.
• Then, a deeper transverse incision into the hepatoduodenal ligament uncovers
the hepatic artery, on the left side. This vessel should also be opened to
determine its patency.
15.
• Finally, thecommon bile duct will be encountered to the right of the hepatic
artery, with a third and deeper transverse incision.
• It is opened along its entire length, from porta hepatis to its entry into the
duodenum.
• If stones are present, the prosector should document the degree of duct
dilation, if any, proximal to the stone.
17.
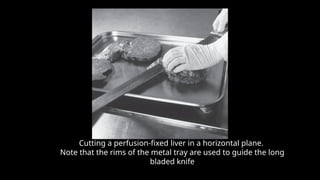
Cutting a perfusion-fixedliver in a horizontal plane.
Note that the rims of the metal tray are used to guide the long
bladed knife
18.
• The livermay be sliced in the coronal or the transverse planes.
• The latter approach yields the most recognizable shape of the liver, with both
lobes well seen and with the porta hepatis clearly shown in at least one slice.
• The best demonstration of a pathologic process must remain the primary goal
when choosing the plane of sectioning.
• It is best to section liver in slices that are no more than 2cm thick.
no more than 2 cm thick.
19.
• This willensure adequate examination and proper fixation of the slices that are
reserved for demonstration.
• To avoid leaving telltale marks of the knife, the prosector should use a long, sharp
knife, with as minimal downward force as possible.
• The knife should be drawn in long sweeps, using the entire length of the blade.
20.
• Push thetip of her index finger through a slice of unfixed liver in every autopsy
to roughly assess the degree of fibrosis.
• Normally with this maneuver, the liver will tear easily. This so called "finger test"
can be applied to fresh slices of liver only, no more than 2-2.5 cm thick.
• With consistent use of this test, the pathologist may be able to recognize early
hepatic fibrosis grossly.
21.
• In situationsof a tumor involving the porta-hepatis or of cirrhosis with a
portosystemic shunt, the prosector must use ingenuity to choose the
dissection approach that will best demonstrate the relationships between
the pathologic process and the adjacent organs.
• This may require that the biliary connections be preserved and that the
organ block be sliced in the coronal, transverse or even sagittal plane.
22.
• In situationsof a tumor involving the porta hepatis or of cirrhosis with a
portosystemic shunt, the prosector must use ingenuity to choose the
dissection approach that will best demonstrate the relationships between
the pathologic process and the adjacent organs.
• This may require that the biliary connections be preserved and that the
organ block be sliced in the coronal, transverse or even sagittal plane.
23.
Autopsy Handling ofthe Liver
• In-situ inspection before removal
• Assessment of size, congestion, adhesions
• Careful separation from diaphragm
• Preservation of vascular connections
• Documentation before slicing
24.
• Orientation: Placethe liver on the cutting board with the anterior surface facing
up.
• Serial Sectioning: Using a long knife, make serial parallel incisions at 1 cm
intervals perpendicular to the capsule.
• Evaluation: Inspect the cut surface for color consistency, focal lesions, and the
architecture of the hepatic lobules.
• Vessels: Open the portal vein, hepatic artery, and inferior vena cava
longitudinally to check for thrombi or narrowing.
25.
• Adult liver:1200–1800 g
• Increased weight: fatty liver, hepatitis, congestion
• Decreased weight: cirrhosis
• Documentation of overall dimensions
Weighing and Measurements
• Liver placedwith diaphragmatic surface down
• Serial slicing at 1–1.5 cm intervals
• Right to left lobe slicing
• Exposure of intrahepatic lesions
Sectioning Technique
28.
Internal Examination
• Assessmentof color and texture
• Identification of portal tracts
• Evaluation of bile ducts and vessels
• Detection of nodules and fibrosis
29.
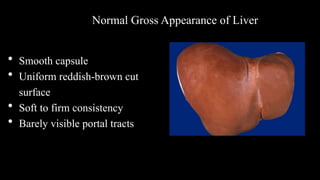
• Smooth capsule
•Uniform reddish-brown cut
surface
• Soft to firm consistency
• Barely visible portal tracts
Normal Gross Appearance of Liver
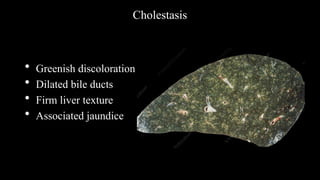
30.
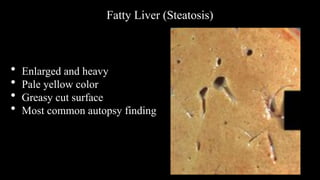
Fatty Liver (Steatosis)
•Enlarged and heavy
• Pale yellow color
• Greasy cut surface
• Most common autopsy finding
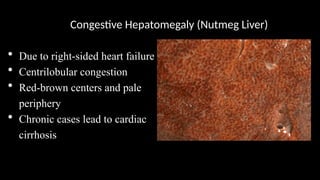
Congestive Hepatomegaly (NutmegLiver)
• Due to right-sided heart failure
• Centrilobular congestion
• Red-brown centers and pale
periphery
• Chronic cases lead to cardiac
cirrhosis
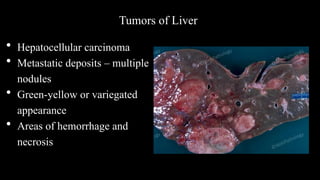
Tumors of Liver
•Hepatocellular carcinoma
• Metastatic deposits – multiple
nodules
• Green-yellow or variegated
appearance
• Areas of hemorrhage and
necrosis
36.
Sections to Submit– Routine
• Right lobe – two sections (Deep parenchyma, including capsule)
• Left lobe – one or two sections (Deep parenchyma, including
capsule)
• Hilar section with bile duct and vessels
• Any focal lesion
• Lymph nodes






























![Fundamentals of LIVER pathology [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/liverautosaved-250420183028-4673e515-thumbnail.jpg?width=640&height=640&fit=bounds)



























