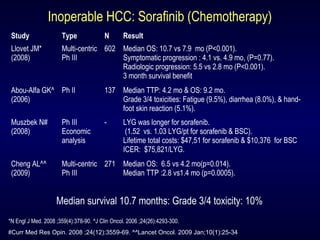
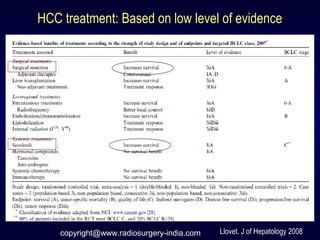
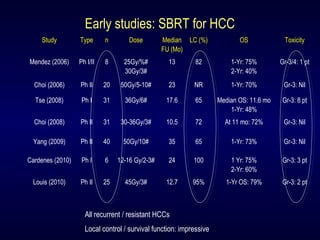
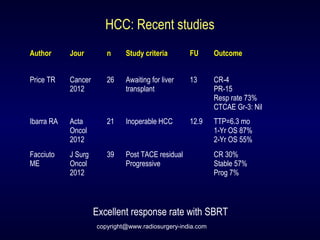
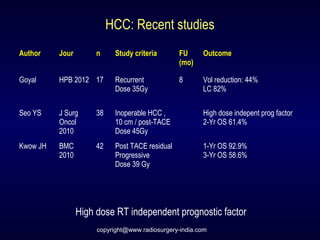
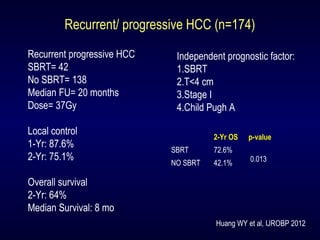
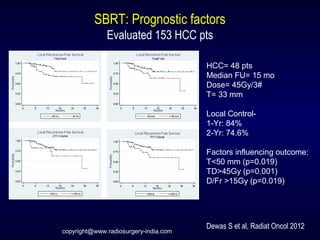
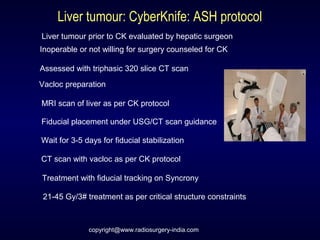
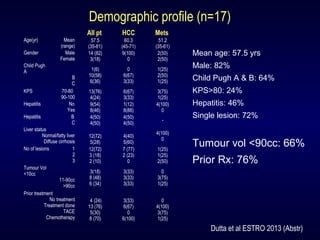
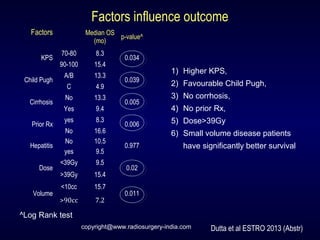
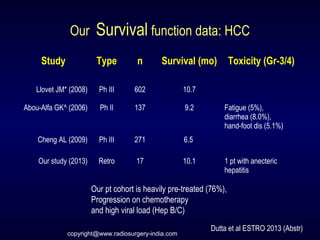
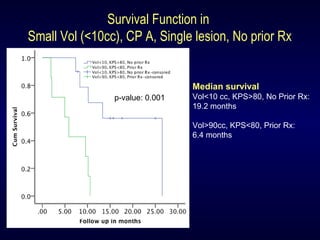
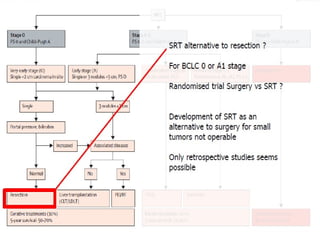
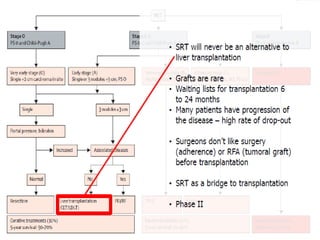
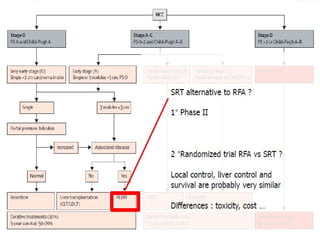
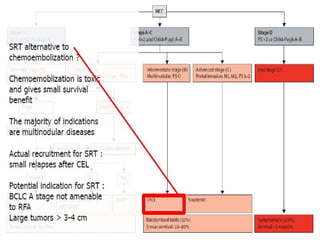
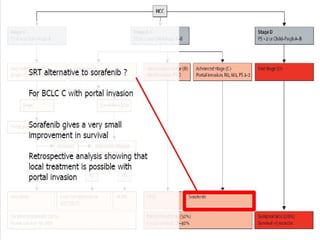
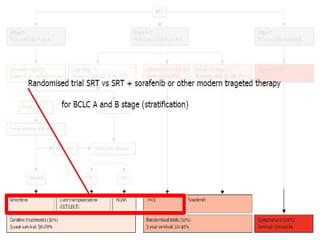
CyberKnife is a promising treatment for patients with inoperable hepatocellular carcinoma (HCC), showing low toxicity and better survival rates in small tumors. Studies suggest that high doses enhance outcomes, and combining CyberKnife with chemotherapy may improve efficacy. Factors influencing survival include performance status, tumor volume, and previous treatments.