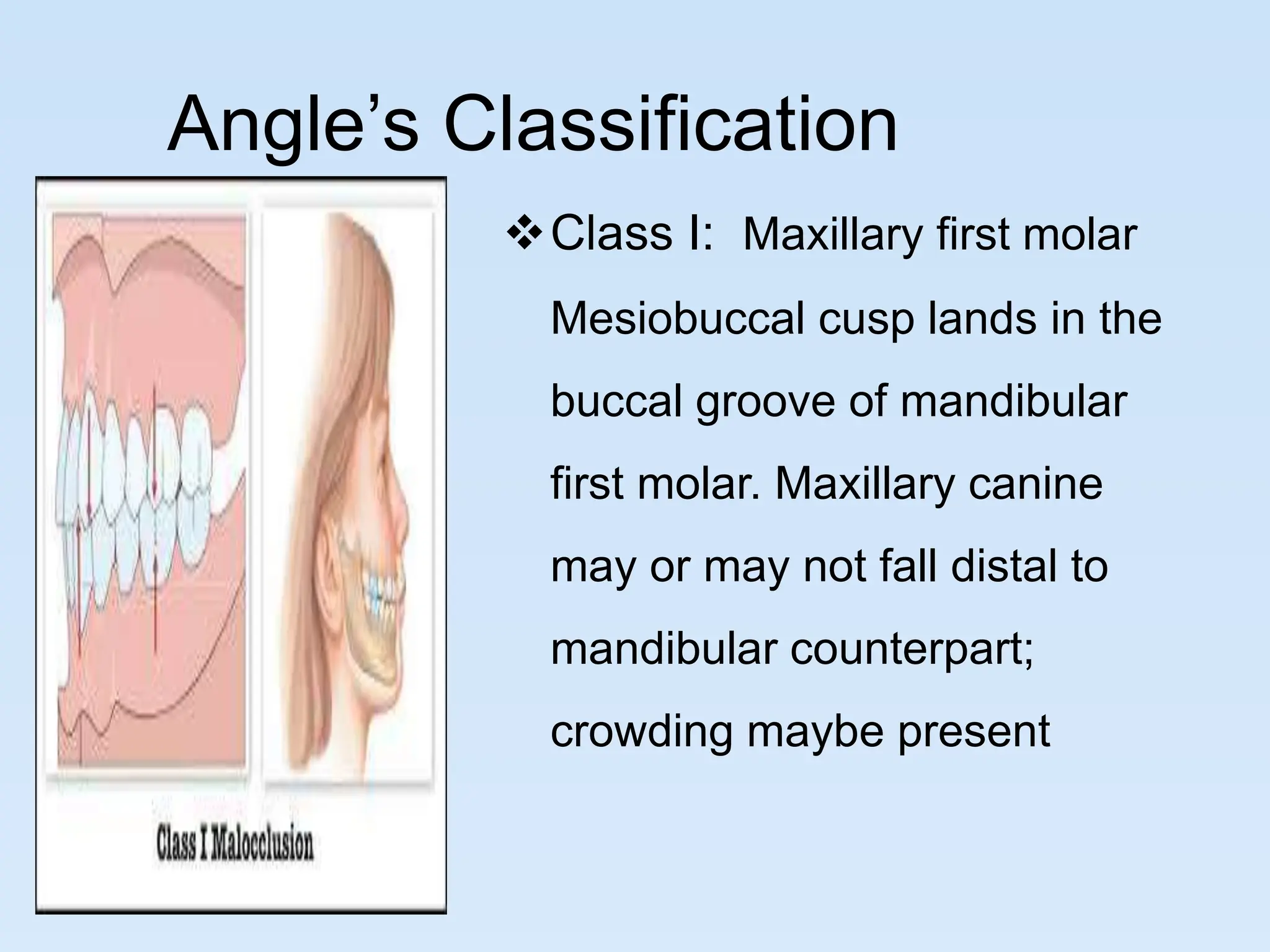
Orthodontics deals with correcting irregularities of the teeth and jaws to improve appearance and function. It has its origins in ancient practices but was recognized as a specialty in the 19th century. The goal of orthodontic treatment is to achieve structural balance, aesthetic harmony and functional efficiency as described by Edward Angle, who is considered the father of modern orthodontics. Treatment may involve appliances like braces to align the teeth or surgery to correct severe malocclusions.






















































































![Introduction [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/introductionautosaved-230711062035-39a63e5f-thumbnail.jpg?width=640&height=640&fit=bounds)

























