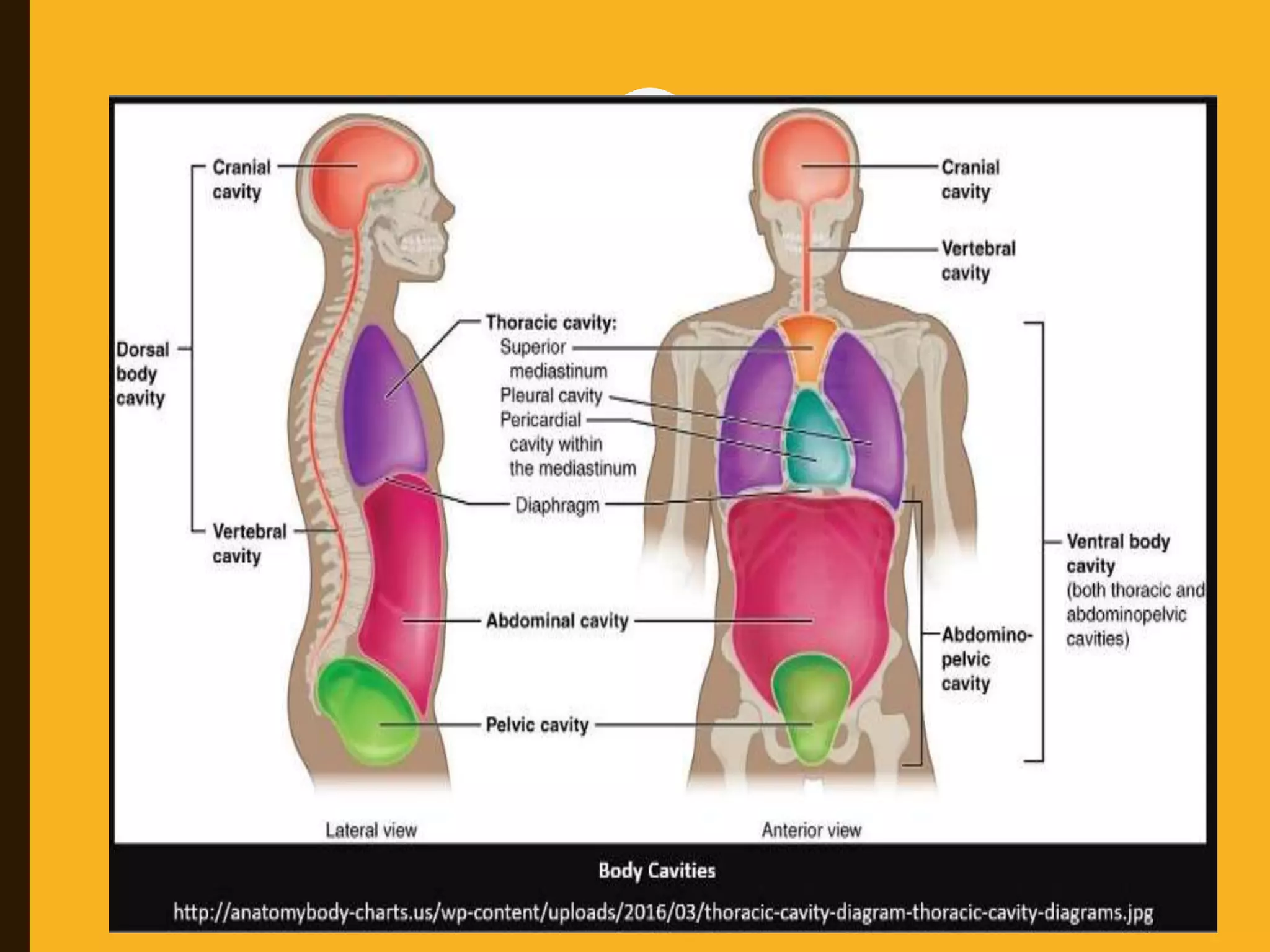
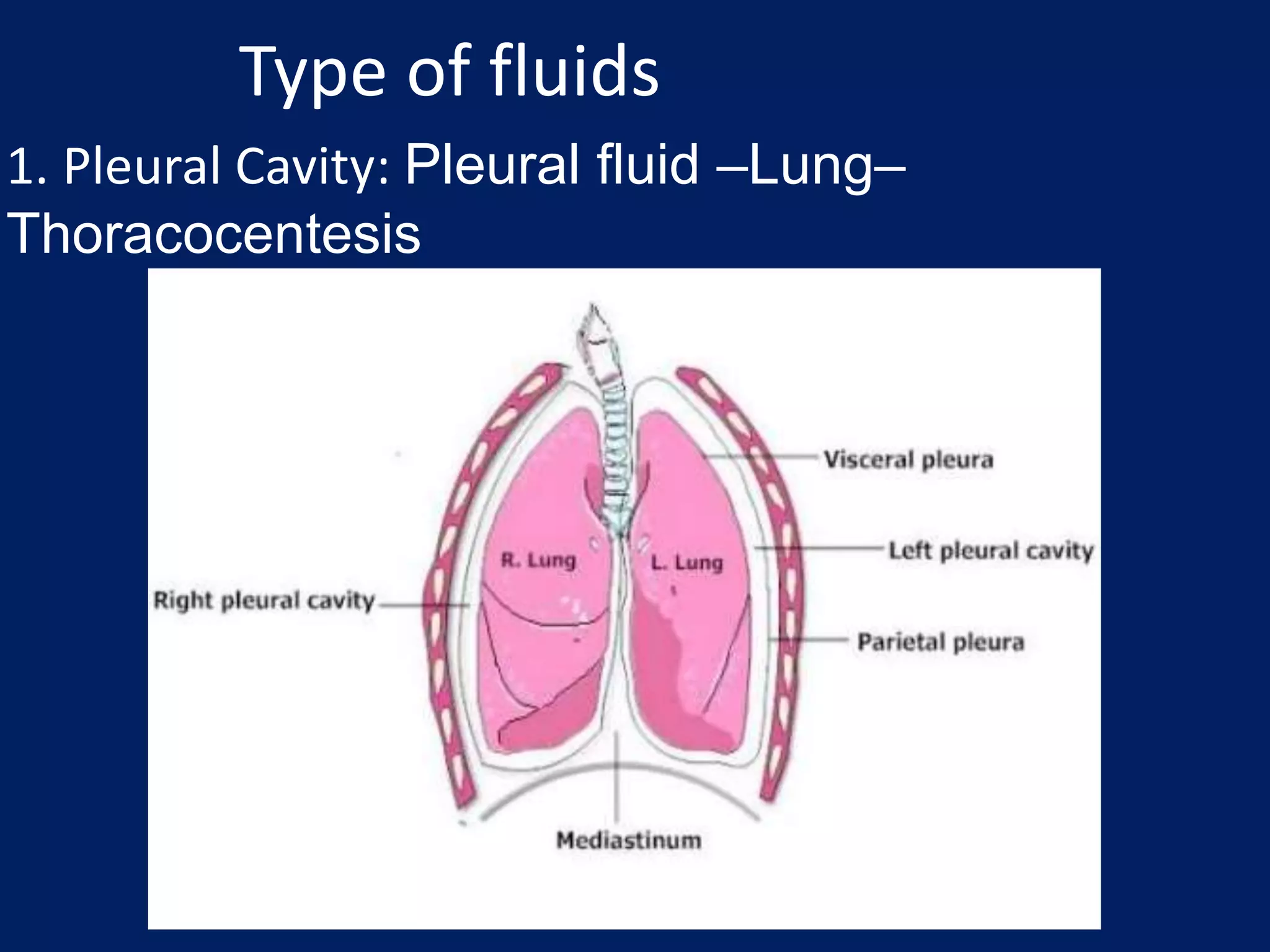
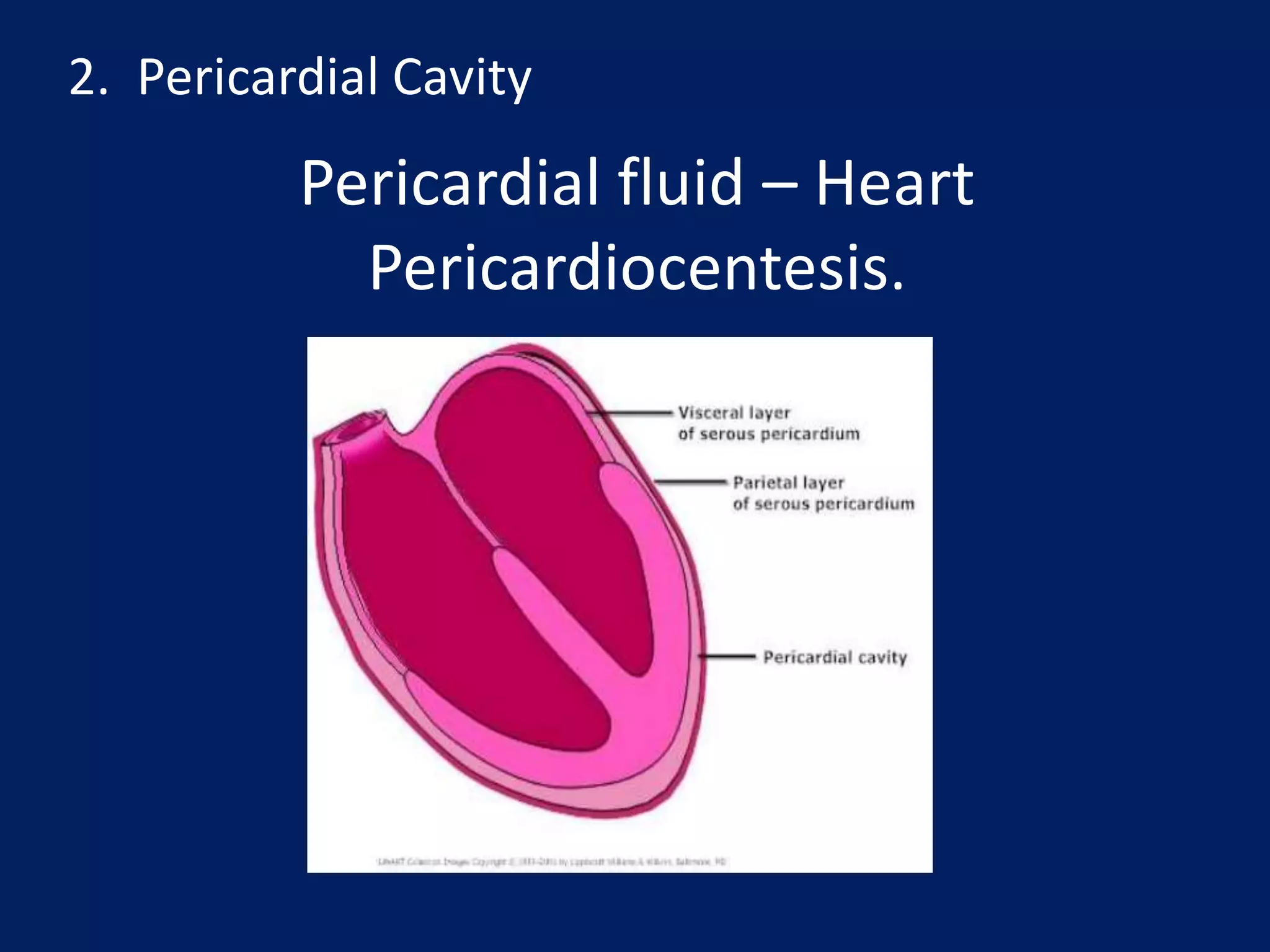
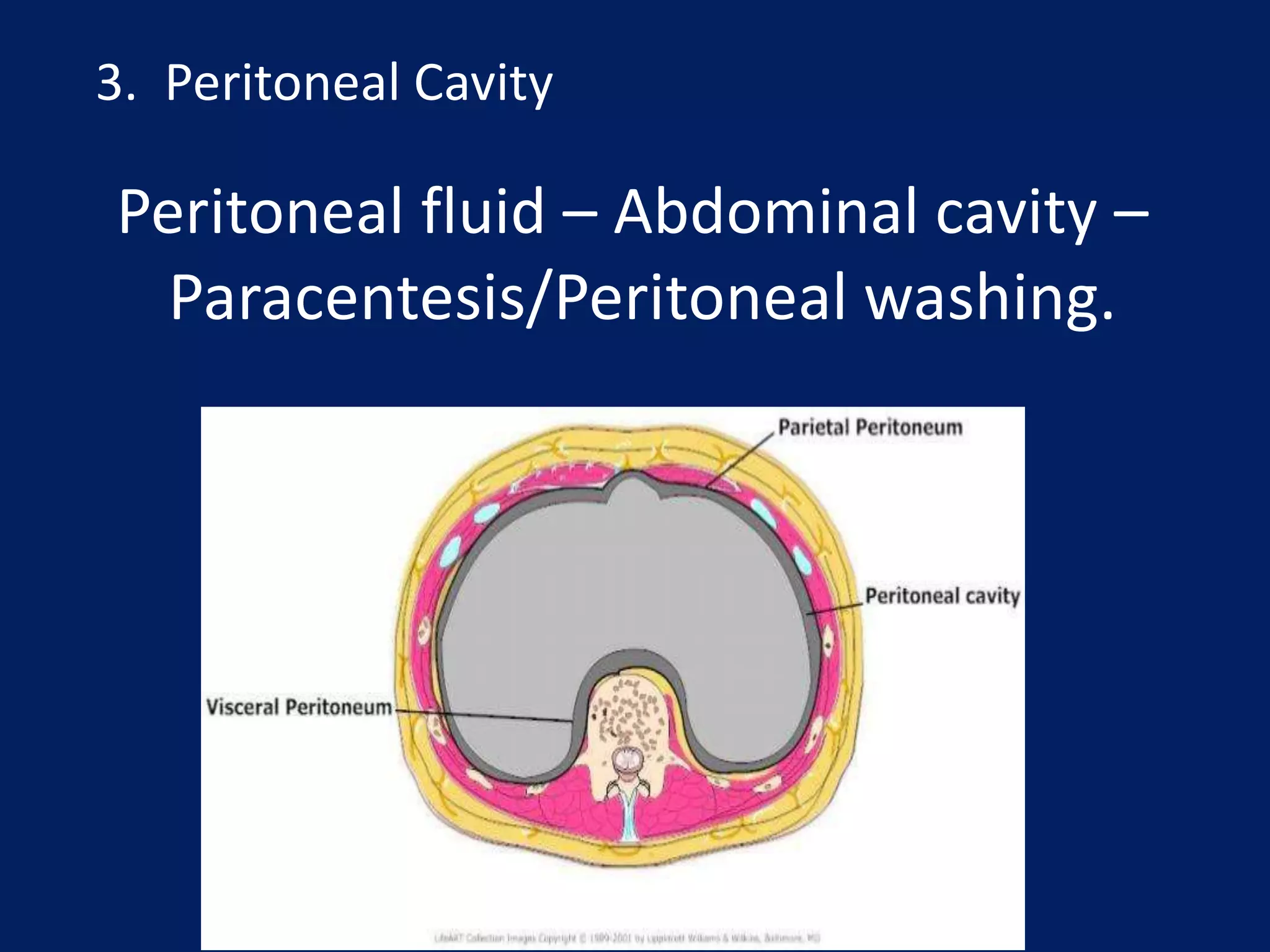
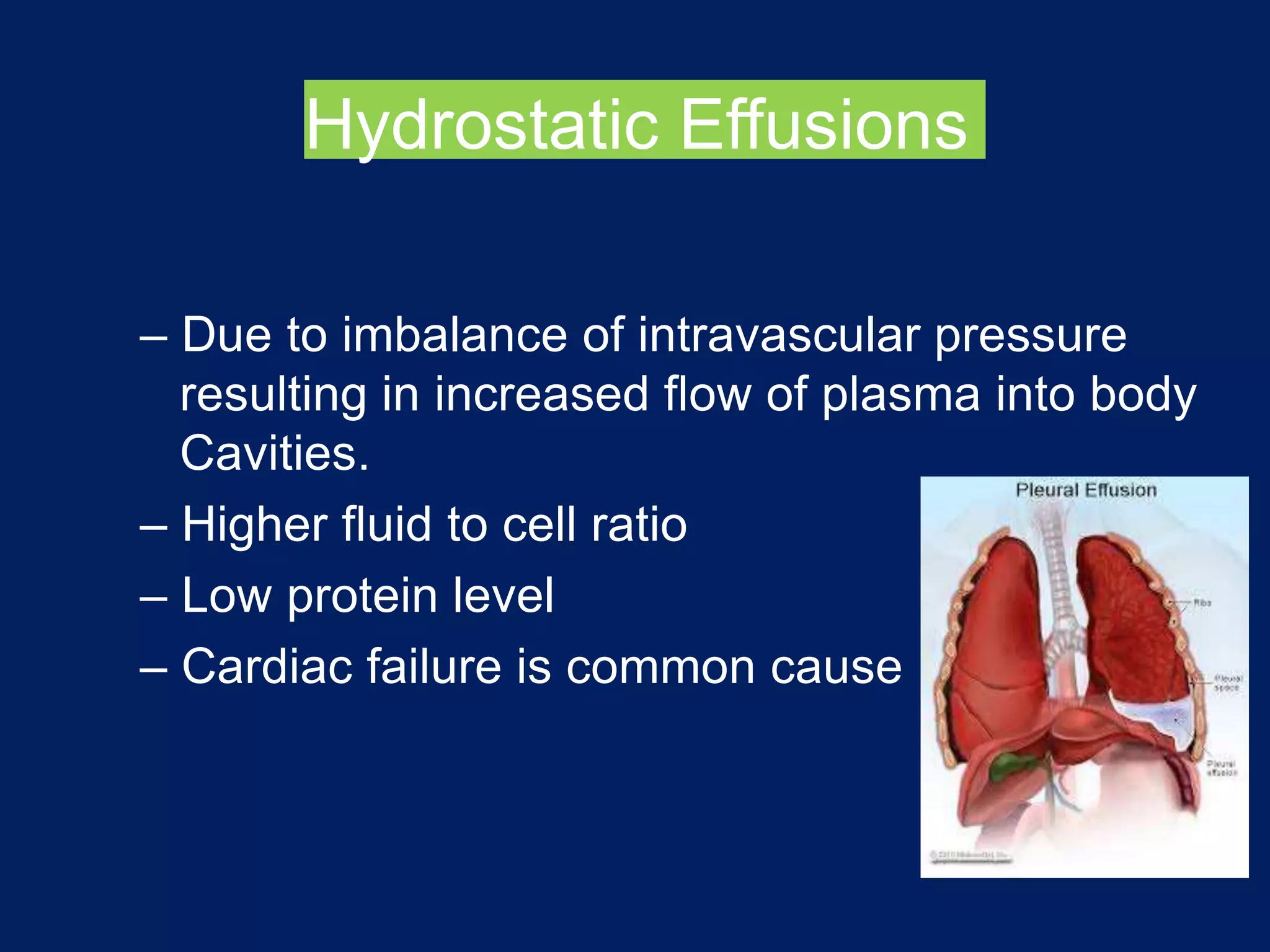
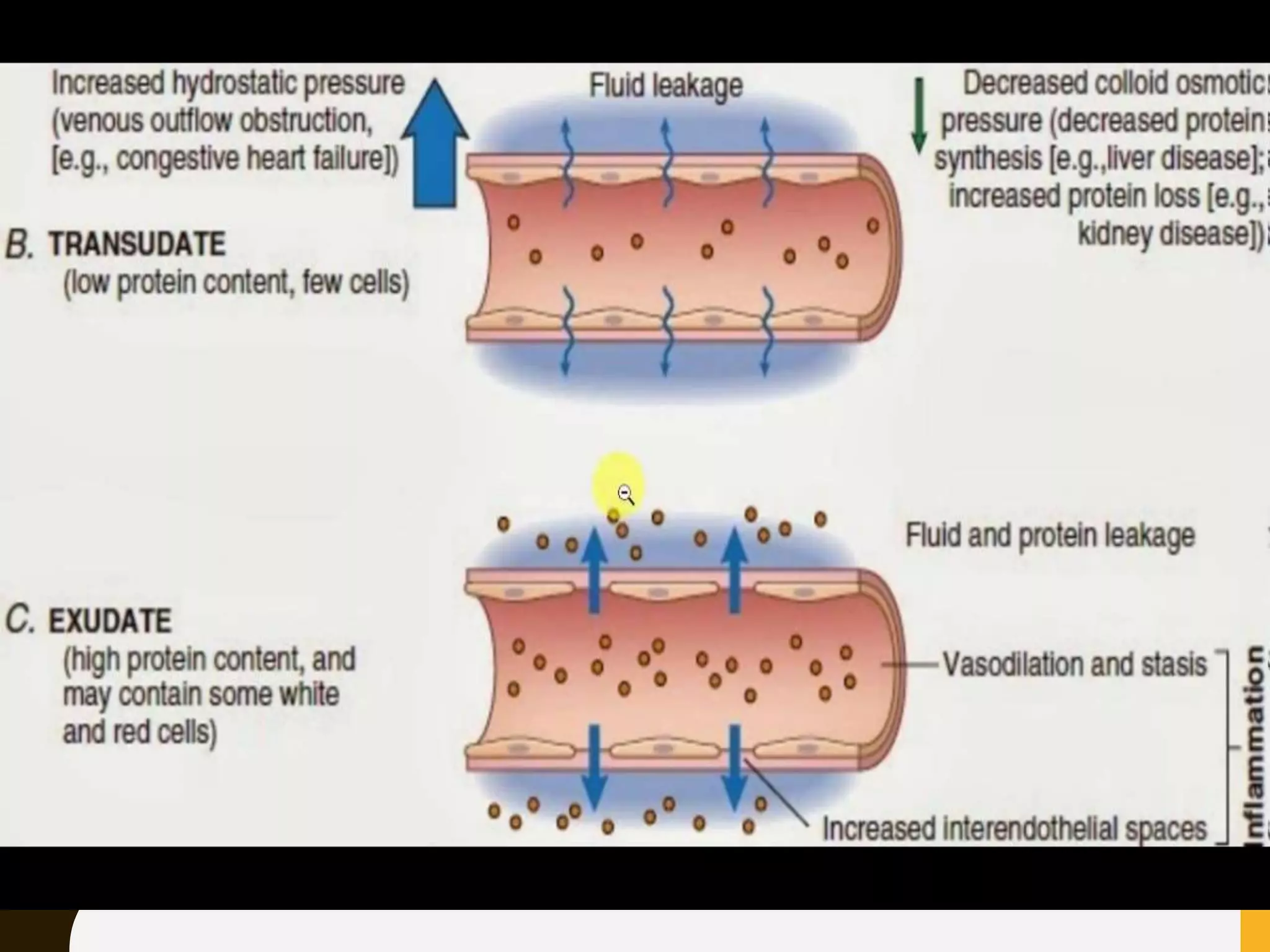
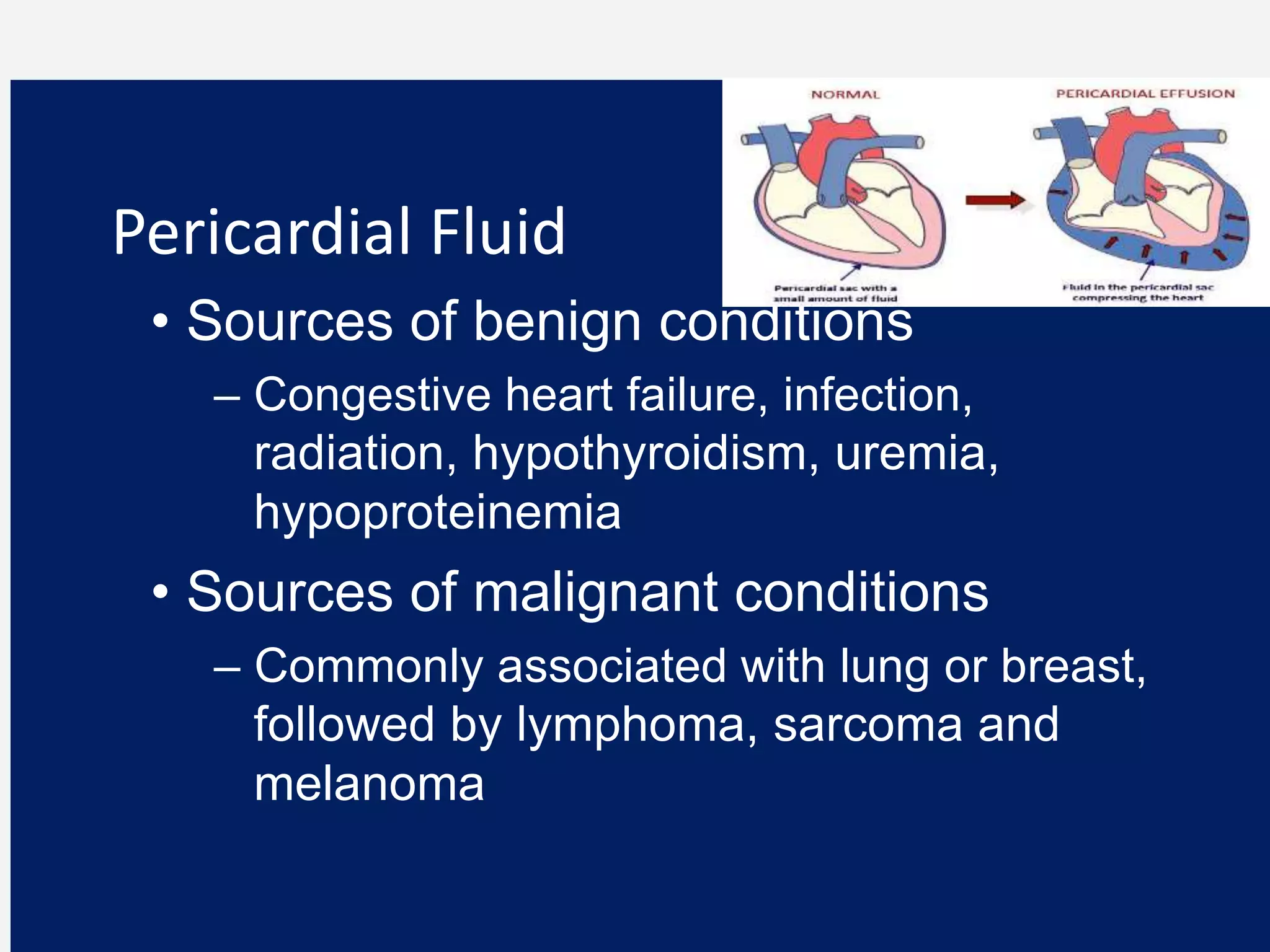
The document discusses serous body fluids, which lubricate the pleural, pericardial, and peritoneal cavities. Serous fluid is formed from an ultrafiltrate of plasma and provides lubrication between the parietal and visceral membranes lining each cavity. An accumulation of fluid in these cavities, called an effusion, can result from abnormal fluid production or reabsorption. Effusions are classified as transudative or exudative based on their protein content and cause. Common causes of effusions include congestive heart failure, infection, inflammation, and malignancy. Analysis of pleural, pericardial, and peritoneal fluid can provide diagnostic information about underlying conditions.





































![serous fluid Dr shweta [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/serousfluiddrshwetaautosaved-221213040107-a9b2a766-thumbnail.jpg?width=640&height=640&fit=bounds)

















































