Download as PDF, PPTX



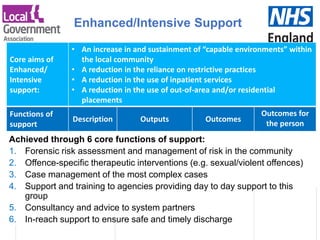
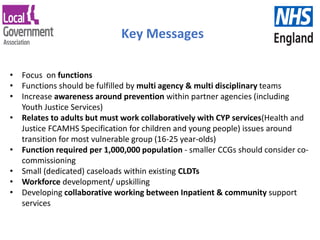


The document outlines a model service specification for community-based forensic support aimed at improving care and quality of life for individuals with learning disabilities and/or autism. It emphasizes early intervention, risk assessment, and collaborative support to prevent contact with the criminal justice system and reduce inpatient care needs. Key functions of the model include offence-specific interventions, case management, and consultancy to system partners to ensure effective support and discharge for affected individuals.





















































































