Download to read offline
























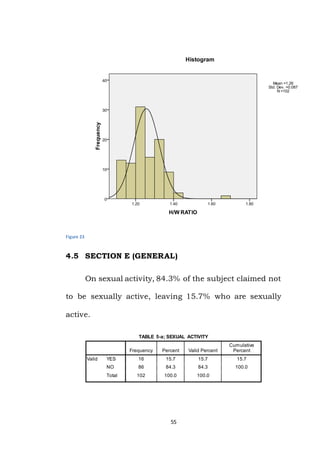

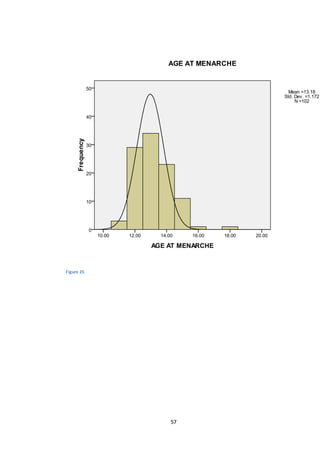

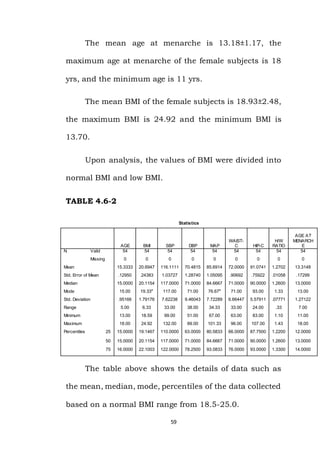
















This document discusses a study exploring the relationship between body mass index (BMI) and age at menarche. It begins with an introduction to BMI and its use as a standard measurement of overweight and obesity. It then reviews literature showing relationships between higher BMI, earlier menarche, and higher levels of body fat associated with earlier menarche. The study aims to determine if age at menarche is dependent on BMI. It involves measuring height, weight, waist circumference, hip circumference, and blood pressure of 102 female adolescents to calculate their BMI and examine its relationship to their reported age at menarche.






























































