Downloaded 91 times
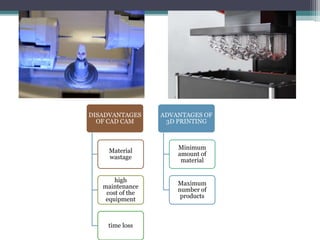
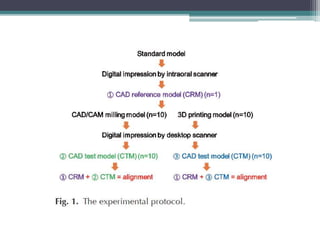
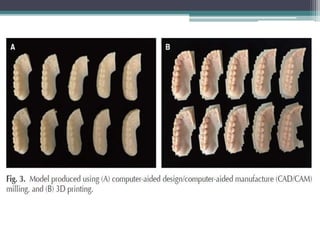
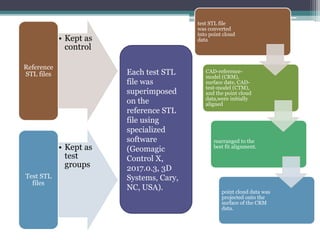
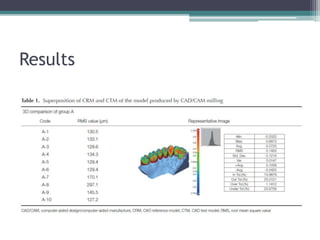
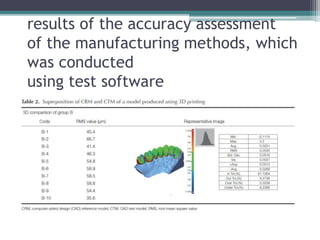
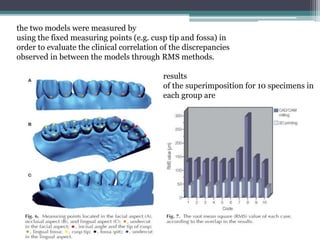
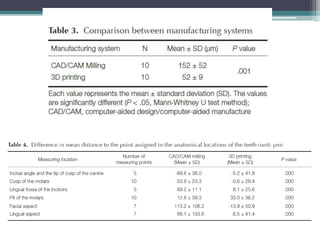
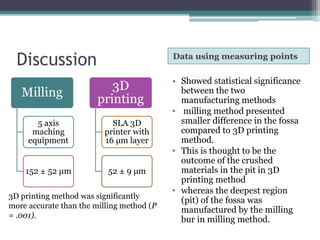


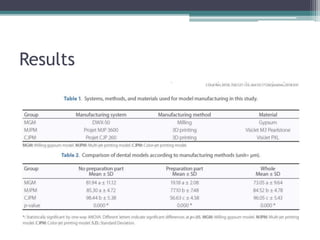
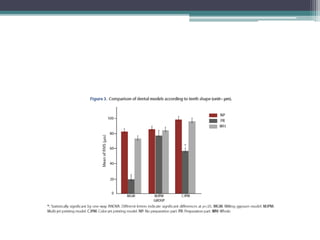
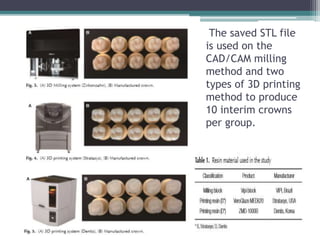
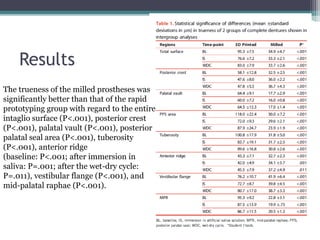
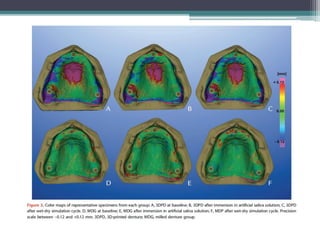
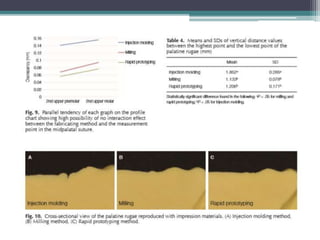
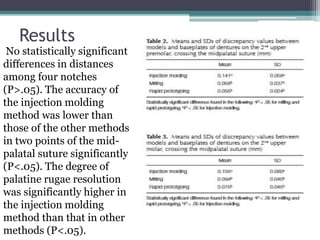
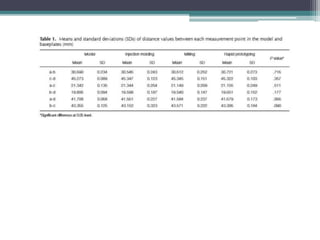

This document summarizes and compares the accuracy of dental models manufactured using CAD/CAM milling and 3D printing methods. It finds that 3D printing methods produced models with significantly higher accuracy than milling methods based on measurements of deviation between reference and test models. Specifically, 3D printed models showed average deviations of 52 μm compared to 152 μm for milled models. However, both methods still have limitations for producing working models. The document also reviews several related studies that found 3D printing generally produces more accurate dental restorations and models than CAD/CAM milling.







































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









