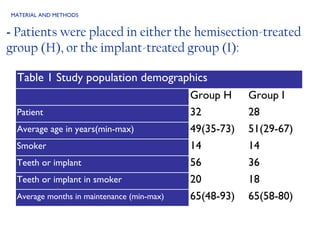
This retrospective study compares the long-term complication and survival rates of root-resected mandibular molars and dental implants in patients with grade III furcation involvement. Results indicate that while both treatments can achieve approximately six years of complication-free survival, root-resected molars exhibit a higher risk for complications. The study suggests that dental implants replacing periodontally involved molars result in fewer complications than hemisected molars, although further research is required for generalization.























































![Periodontal regeneration versus extraction and dental implant or [Autosaved]....](https://cdn.slidesharecdn.com/ss_thumbnails/periodontalregenerationversusextractionanddentalimplantorautosaved-230828130403-1847e62a-thumbnail.jpg?width=640&height=640&fit=bounds)



































