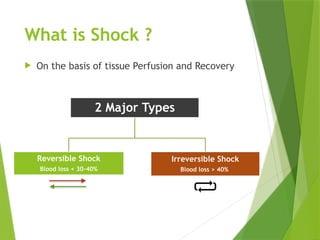
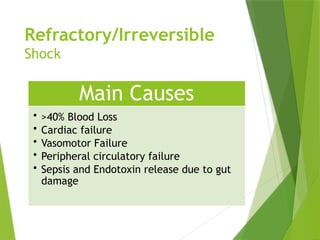
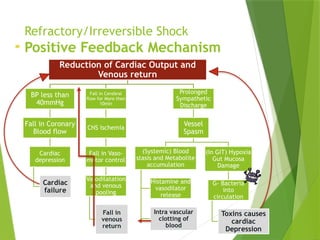
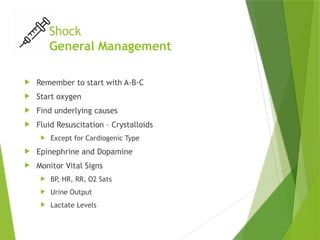
The document discusses irreversible shock, detailing its types, signs, symptoms, causes, and management strategies. It emphasizes the positive feedback mechanisms leading to persistent shock despite treatment, highlighting high mortality and poor prognosis. An illustrative case study is included to demonstrate the characteristics of refractory shock.











![APPROACH TO SHOCK [Auto-saved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/approachtoshockauto-saved-230707035943-4dc369a3-thumbnail.jpg?width=640&height=640&fit=bounds)













































