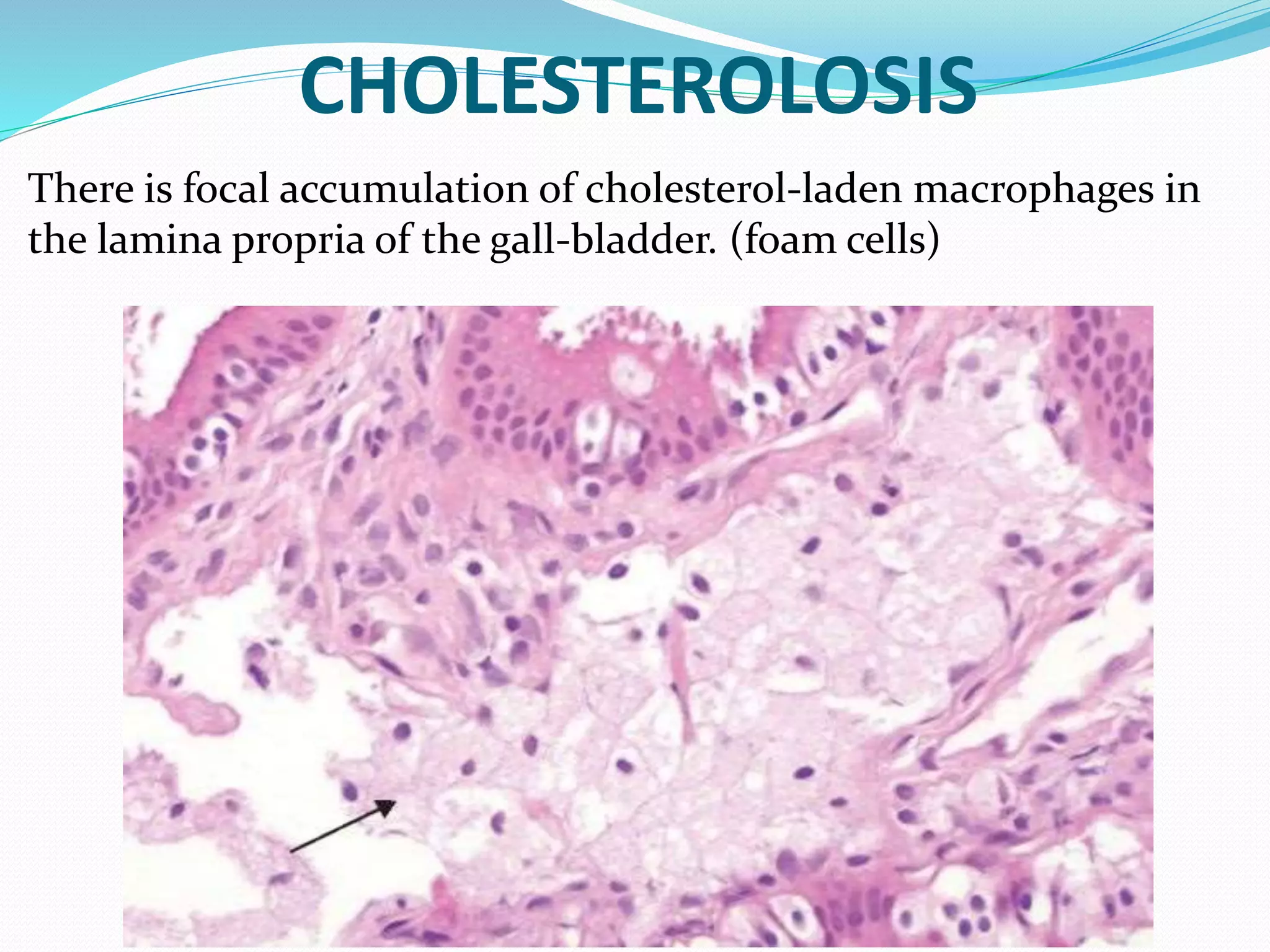
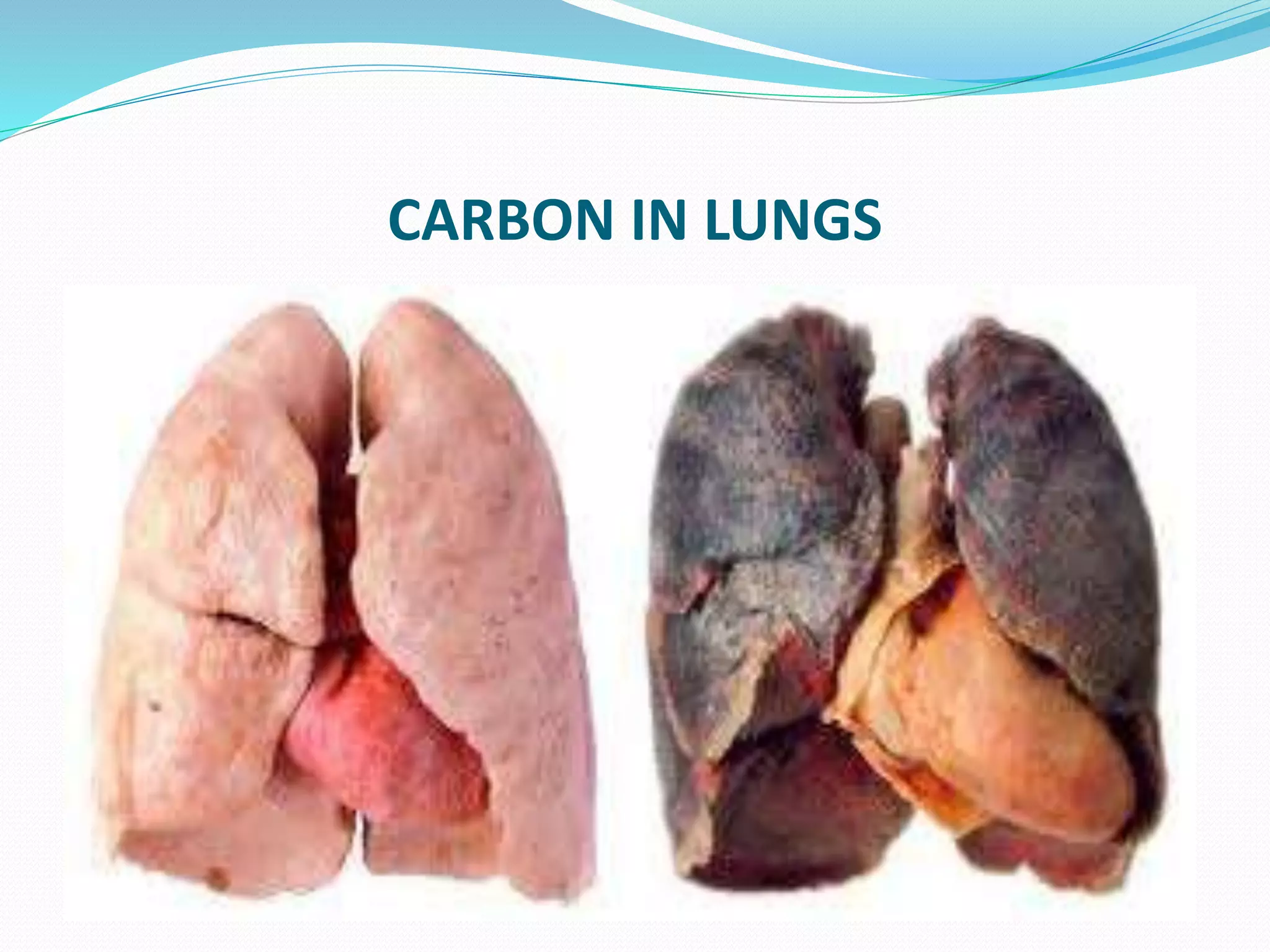
Intracellular accumulations occur when cells abnormally store substances endogenously produced or absorbed from outside the cell. Common types of accumulations include lipids like triglycerides and cholesterol, proteins, glycogen, and pigments. Accumulations can be harmless, but often correlate with cell injury. They result from imbalances between production or absorption of the substance versus the cell's ability to metabolize or transport it out. Certain genetic disorders can also cause accumulations by impairing the breakdown of metabolites.