Definition
An infectionof the endocardium and/or heart valves that involves
thrombus formation (vegetation) which then damage the endocardial
tissue and/or valves.
Includes acute, subacute bacterial endocarditis + non bacterial
endocarditis to include:
Viruses
Fungi
Autoimmunity
May occur on a previously healthy native heart
4.
Two important factors
A damaged area of endothelium (1)
Bacteraemia (even transient) (2)
Structural abnormalities in the heart with significant pressure gradient or
turbulence produce endothelial damage
Endothelial damage induces thrombus formation with deposition of sterile
clumps of platelets and fibrin (non bacterial thrombus)
Non bacterial thrombus provides a nidus for bacteria to adhere and
eventually form infected vegetation
Infective Endocarditis
NonbacterialThrombotic Endocarditis
Endothelial injury
Hypercoagulable state
Lesions seen at coaptation points of valves
Atrial surface mitral/tricuspid
Ventricular surface aortic/pulmonic
Modes of endothelial injury
High velocity jet
Flow from high pressure to low pressure chamber
Flow across narrow orifice of high velocity
Bacteria deposited on edges of low pressure sink or site of jet impaction
Venturi Effect
Platelet-fibrin
thrombi
Aetiology
Streptococci viridans(post dental procedure) and staphylococcus aureus
(normal native valve) are the leading causes
Group D enterococci – post lower bowel or genitourinary manipulation
CONS – indwelling central venous catheter
Pseudomonous/serratia – IV drug users
HACEK (Haemophilus, Actinobacillus, cardiobacterium, Eikenella and
Kingella) – neonates and immunocompromised children
Fungal endocarditis is a severe disease with poor prognosis
10.
Epidemiology
Patients withCHD in which blood is ejected at high velocities through a
hole or stenotic orifice are most susceptible
Often complicates RHD
May occur in children with normal valves and children with no cardiac
malformations
It is rare in infancy, but may occur post open heart surgery
11.
Risk factors
Cyanoticcongenital heart disease
Valvular lesions
Previous episode of bacterial endocarditis
Prosthetic valve
Central venous catheters
Residual cardiac defect post surgical or catheter intervention for that
defect
12.
Features of endocarditisare due to:
Bacteraemia
Local cardiac invasion by organisms leading to valve detruction and or
rupture of chordae tendinae and hence acute HF
Peripheral embolizaton which may produce septic embolic phenomena
(osteomyelitis, meningitis and pneumonia)
Formation of immune complexes, in circulation will cause vasculitis
Manifestations
May beacute, sub acute or even chronic
May be very non specific with fevers going on for months
“B symptoms”
New or changing murmers with associated CCF
Skin manifestation..more common in the chronic type
Splenomegaly and petechiae
Stroke
Cerebral abscesses
Mycotic aneurysms
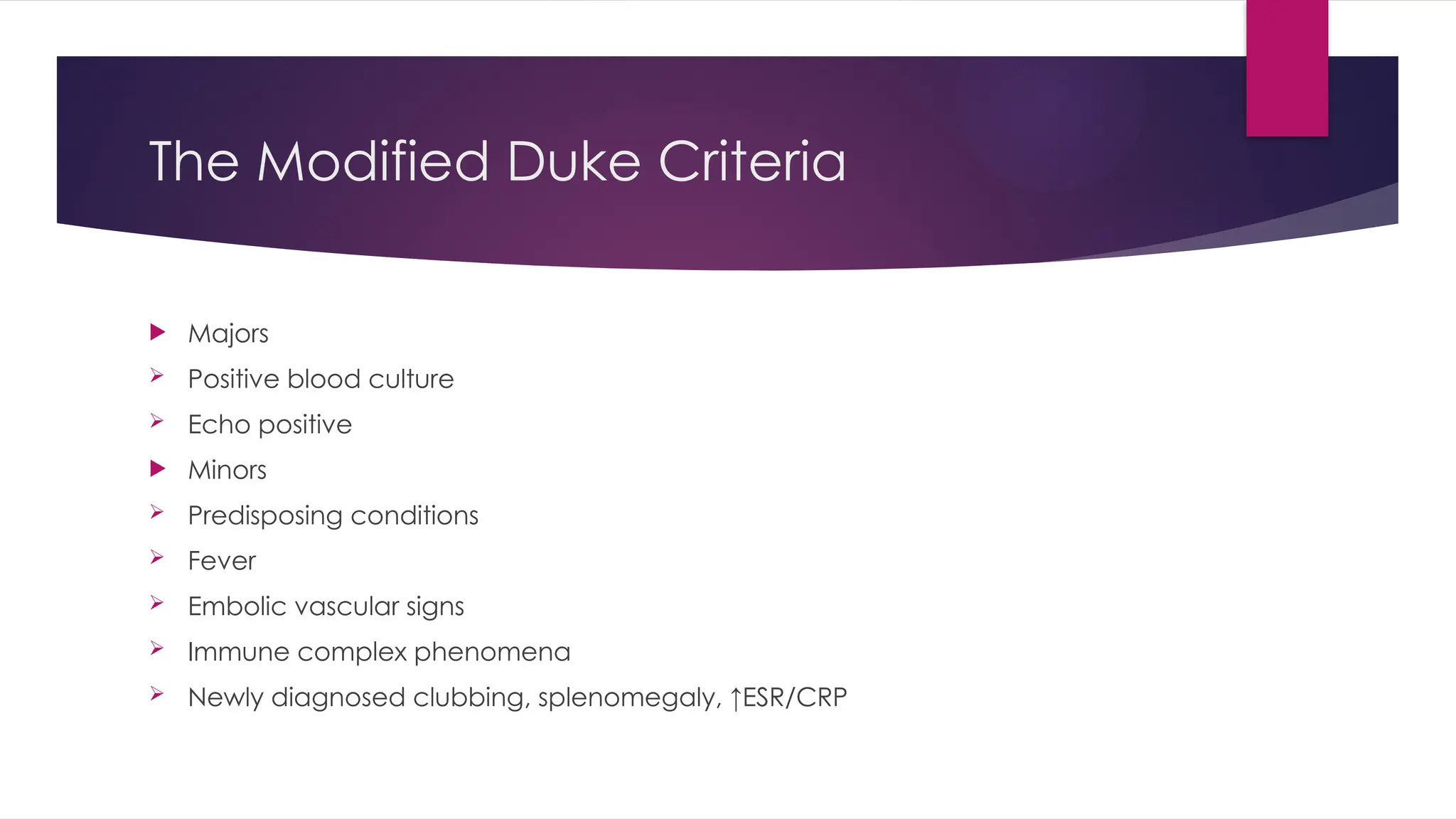
Diagnosis
BLOOD CULTURE,BLOOD CULTURE, BLOOD CULTURE!!
3 – 5 samples needed
Transthoracic + transoesophageal echo may help localize vegetations
Normal echo does not exclude endocarditis
24.
Laboratory Parameters
FBC– Anaemia in 70-90% (normocytic normochromic)
Leukocytosis – 50%
ESR –Elevated in 100% patients mean about 55mm/h
C-reactive protein – elevated in almost all patients. Decreases with
successful treatment and therefore can be used to monitor response to
antibiotic therapy
Urinalysis – proteinuria (50-60%); microscopic haematuria (30-50%)
25.
Prognosis and complications
Is fatal without antibiotics
Mortality still as high as 40% even with use of antibiotics
Severe CCF, life threatening arrhythmias
CNS emboli
26.
Treatment
Recognize thatvegetations house organisms that now become
inaccessible as these are avascular
Broad spectrum antibiotics 1st
line Xpen/Gentamicin
4 – 6 weeks duration
Treat the CCF (digoxin, salt restriction, diuretics)
Surgery may be indicated for severe aortic or mitral involvement
27.
Prevention
Good oral/dentalhygiene
Antibiotic prophylaxis for various procedures:
Dental cleaning or any form of dental manipulation
Scopic examinations: endo,broncho,cystoscopy
Editor's Notes
#8 The reduction in fluid pressure that results when a fluid flows through a constricted section






































![Infective Endocarditis Group [A7] Seminar](https://cdn.slidesharecdn.com/ss_thumbnails/infectiveendocarditisa7-250627114414-bb3356a5-thumbnail.jpg?width=640&height=640&fit=bounds)

























![Non-Communicable Diseases [Repaired].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/non-communicablediseasesrepaired-240730032431-732c7df7-thumbnail.jpg?width=640&height=640&fit=bounds)






















