Download to read offline


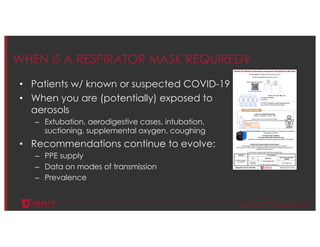
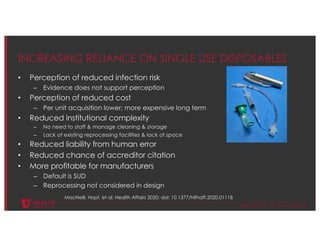

The document discusses infection control measures related to COVID-19, emphasizing the dual benefits for patient and healthcare professional safety. It critiques the widespread reliance on single-use disposables, highlighting their environmental impact and supply chain vulnerabilities. The document advocates for a transition to a circular economy in healthcare to reduce these negative effects and improve sustainability.









































































