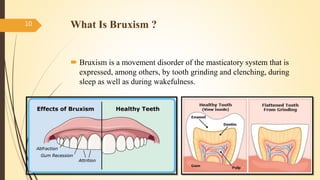
This document discusses implants in patients with bruxism. It defines implants and osseointegration. Bruxism can overload implants and cause biological and biomechanical complications like bone loss, screw loosening, and fracture. Bruxism is diagnosed through tooth wear, muscle hypertrophy, and jaw pain/fatigue. While some research shows bruxism does not affect implants, occlusal considerations are important for implant prostheses given their rigid fixation. Management of bruxism includes night guards and pharmacological therapies to reduce forces. More research is still needed on the effects of bruxism on dental implants.




![Pharmacological Approach
Low doses of the dopamine D1/D2 receptor agonist pergolide
finally resulted in a substantial and lasting reduction in the bruxism
The use of acetylcholine-inhibiting formulations such as botulinum
toxin
Benzodiazepam–type drugs and muscle relaxants have been
prescribed by clinicians in an attempt to reduce nocturnal bruxism
Dopaminergic medication also appears to demonstrate potential
utility in reducing nocturnal bruxism
24
[Guideline] Kato T, Thie NM, Montplaisir JY, Lavigne GJ. Bruxism
and orofacial movements during sleep.Dent Clin North Am. 2001
Oct. 45(4):657-84](https://image.slidesharecdn.com/clinicalmanagementofimplantprosthesesinpatientwith-151231034238/85/IMPLANTS-IN-BRUXISM-24-320.jpg)

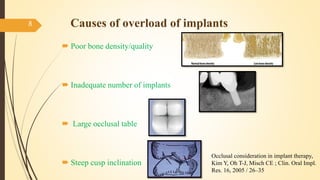
![ Occlusal consideration in implant therapy, Kim Y, Oh T-J, Misch CE ; Clin. Oral Impl. Res.
16, 2005 / 26–35
Effects Of Pergolide On Severe Sleep Bruxism In A Patient Experiencing Oral Implant
Failure, Jac. Van Der Zaag, Frank Lobbezoo, J Oral Rehabil. 2007;34(5):317-322.
Bruxism: Its Multiple Causes And Its Effects On Dental Implants – An Updated Review* F.
Lobbezoo, J. Van Der Zaag & M. NAEIJE, Journal Of Oral Rehabilitation 2006 33; 293–
300
[Guideline] Kato T, Thie NM, Montplaisir JY, Lavigne GJ. Bruxism and orofacial
movements during sleep.Dent Clin North Am. 2001 Oct. 45(4):657-84
Does bruxism contribute to dental implant failure? Zhou Y, Gao J, Luo L, Wang Y. A
systematic review and meta-analysis. Clinical Implant Dentistry and Related Research 2015
Management of Abutment Screw Loosening: Review of Literature and Report of a Case
Vinod Krishnan, C. Tony Thomas & Ipe Sabu Volume 14 Number 3 J Indian Prosthodont
Soc (2014) 14:208-214
27](https://image.slidesharecdn.com/clinicalmanagementofimplantprosthesesinpatientwith-151231034238/85/IMPLANTS-IN-BRUXISM-27-320.jpg)




































































