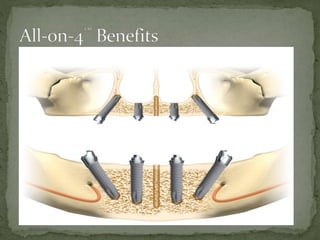
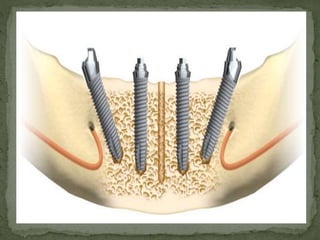
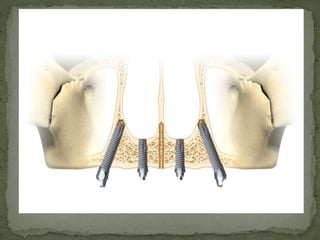
1) The document discusses the "All-on-4" technique for placing four dental implants (two tilted posteriorly and two anterior) to support a fixed prosthesis in edentulous maxilla or mandible.
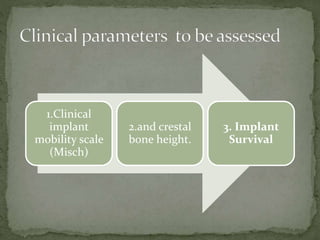
2) Previous studies have shown this technique to be predictable and successful with high implant survival rates and minimal bone loss.
3) Tilting the posterior implants provides benefits like avoiding anatomical structures and improving prosthesis support.